
Abstract
Introduction:
e-Consultation provides a new way to deliver healthcare services online. With the help of e-Consultation services, patients can gain access to nationwide medical expertise that otherwise would not be available to them. As an online delivery approach, e-Consultation also provides a choice for patients to receive medical advice from online doctors immediately, no matter how far away from the hospital they may be or how late in the day it is. However, the adoption and usage of e-Consultation is still far from satisfactory. Therefore, understanding why and when patients use e-Consultation services are important research questions.
Materials and Methods:
Considering that the choice of a healthcare provider is a serious decision, this research uses the trust perspective to explain the e-Consultation service adoption phenomenon. Specifically, trust is conceptualized as a second-order construct consisting of two dimensions: competence and integrity. In addition, e-Consultation is viewed as a supplementary resource to traditional off-line consultation services, and disease type as a contextual factor is hypothesized to focus the context where e-Consultation services are more suitable. A scenario-based survey was conducted to test the proposed research model. We obtained a total of 190 valid questionnaires.
Results:
Our results indicated that trust (p < 0.01) had a positive effect on the intention to use an e-Consultation service. Meanwhile, our results also indicated that the higher the disease is in rarity (p < 0.05), severity (p < 0.01), or urgency (p < 0.05), the lesser the positive effect of trust is on the intention to use an e-Consultation service.
Conclusions:
Trust is the major driving force of an e-Consultation service adoption. When the disease is high in rarity, severity, or urgency, an off-line healthcare provider is less capable of providing meaningful, qualified, and immediate service. Therefore, there is a decreased positive effect of trust on the intention to use an e-Consultation service for those diseases.
Introduction
Use of the Internet as a new medium for seeking and delivering healthcare by patients, relatives, and physicians is increasing rapidly. 1 –3 Among these services, e-Consultation appears to be particularly attractive and increasing in popularity. 3 –5 Even in the absence of face-to-face contact between a patient and a provider, an online health consultation offers clear benefits to patients. Most importantly, patients can gain access to medical expertise that otherwise would not be available to them. This is especially valuable for patients who are homebound, in rural areas, in prison, or in other settings that limit their access to treatment. 6 In addition, it is likely to be a valued option for patients with rare medical disorders and patients seeking advice from leading national experts who are geographically far away. 6 Online medical visits also generate a written record of the communication and enable physicians to readily link patients to recommended information sites. In addition, some patients seek online contact with physicians they have not met because they value the anonymity of the clinical encounter for sensitive medical topics or conditions. Therefore, e-Consultation is the most preferred service for patients with Internet access. 7 E-Consultation has been shown to prevent an office visit for approximately 40% of the patients who signed up for the service, 8 and the availability of this service decreased spending on a clinic visit. 9 As highlighted in a recent report by the Institute of Medicine (IOM), online communication between patients and physicians can improve healthcare quality, making healthcare delivery more effective, patient centered, and timely. 6
Although e-Consultation websites have been increasing rapidly in recent years, they are not universally accepted by the public. A recent study showed that e-Consultation is only accepted by 30% of users in the United States. Therefore, understanding why and when patients use e-Consultation services are important research questions. However, very few studies focus on this important research topic. Extant studies mainly focus on e-Consultation system design, 10,11 the usage pattern of e-Consultation systems, 12,13 the e-Consultation practices in progress, 14 or evaluating the impact of e-Consultation services. 15 For example, Liddy et al. 10 proposed a ten-step approach to establishing an e-Consultation service in Eastern Ontario. Olajubu et al. 11 designed a telemedicine platform with mobile terminal devices for the vulnerable areas of developing nations. Pecina and North 12 examined e-Consultation usage patterns and found that a significant proportion of e-Consultations are converted to face-to-face consultations. Another study using a retrospective analysis of medical record use in e-Consultations determined that management questions appeared to be the most common reason for e-Consultation and that the e-Consultants frequently reviewed historical medical data that were older than 1 year at the time of the e-Consultation. 13 Shipherd et al. 14 reported the practice of applying nationwide interdisciplinary e-Consultation services for transgender care in the health administration of veterans. Keely et al. 15 investigated the utilization, benefits, and impacts of an e-Consultation service across diverse specialties and primary care providers.
The most related topic to this study is identifying the facilitators and barriers when implementing e-Consultation systems for organizations. For example, Tuot et al. 16 conducted key informant interviews to identify drivers, facilitators, and barriers of an e-Consultation system's implementation. They found elements of successful e-Consultation system implementation, including executive and clinician leadership, established funding models for specialist clinician reimbursement, and a commitment to optimizing clinician workflows. However, Tuot's study was entirely from the health provider's perspective. Research on e-Consultation adoption from the user or patient perspective is still lacking. In addition, Tuot's study focused on Internet-delivered healthcare interventions (also known as an eVisit service) where the consultation occurs between a doctor and a patient with an existing relationship. 17 An eVisit service provides patients with access to a series of structured, secured message exchanges with a physician using portal technology, providing an alternative for onsite office visits and nonreimbursed phone-based care. 18 However, in this research, we are more interested in the consultation between a doctor and a patient without an established relationship. 4 In this context, trust is a major issue for user adoption because the patient and doctor are unknown to each other; therefore, the user will perceive a high uncertainty regarding the service quality.
Because the choice of a healthcare provider requires a serious decision and its adoption entails the first usage behavior of an e-Consultation service, this research uses the trust perspective to explain the e-Consultation service adoption phenomenon. We are especially interested in the components that users trust regarding e-Consultation and whether these components are all positively related to the intention of e-Consultation usage. Therefore, the first research question of this study can be interpreted as follows:
RQ1: What is the composition of a user's trust regarding an e-Consultation service? Does trust affect a user's intention to use e-Consultation services?
There is no denying that e-Consultation acts as a supplement to traditional healthcare service in off-line hospitals. However, we are unclear about which conditions an e-Consultation will have an increased supplementary effect and which conditions patients will have a high intention to use e-Consultation services even if not enough trust is met. Therefore, the second research question of this study can be interpreted as follows:
RQ2: If a patient's disease is high in rarity, severity, or urgency, will the supplementary effect of an e-Consultation be greater than for other diseases? In addition, with a disease that is higher in rarity, severity, or urgency, will this have a decreased positive effect of trust on the intention to use an e-Consultation service?
To answer these research questions, this study proposes a research model based on the trust perspective. Trust is conceptualized as a second-order construct consisting of two dimensions: competence and integrity. In addition, disease type (rarity, severity, and urgency) is hypothesized to negatively moderate the impact of trust on intention of use. A survey was conducted to test the proposed research model.
The remainder of this article is organized as follows: (a) research model and hypotheses; (b) research methodology; (c) data analysis and results; and (d) the major findings, contributions, and implications of this research. Finally, this article concludes with a discussion on the limitations of the study and directions for future research.
Research Model and Hypothesis Development
To bridge the gap, address the limitations of prior research, and answer the proposed research questions, a research model was developed and is shown in Figure 1. Trust is conceptualized as a second-order construct consisting of competence and integrity. Disease severity, rarity, and urgency are used as moderators. The control variables include age, gender, income, Internet experience, and relation with off-line doctors.
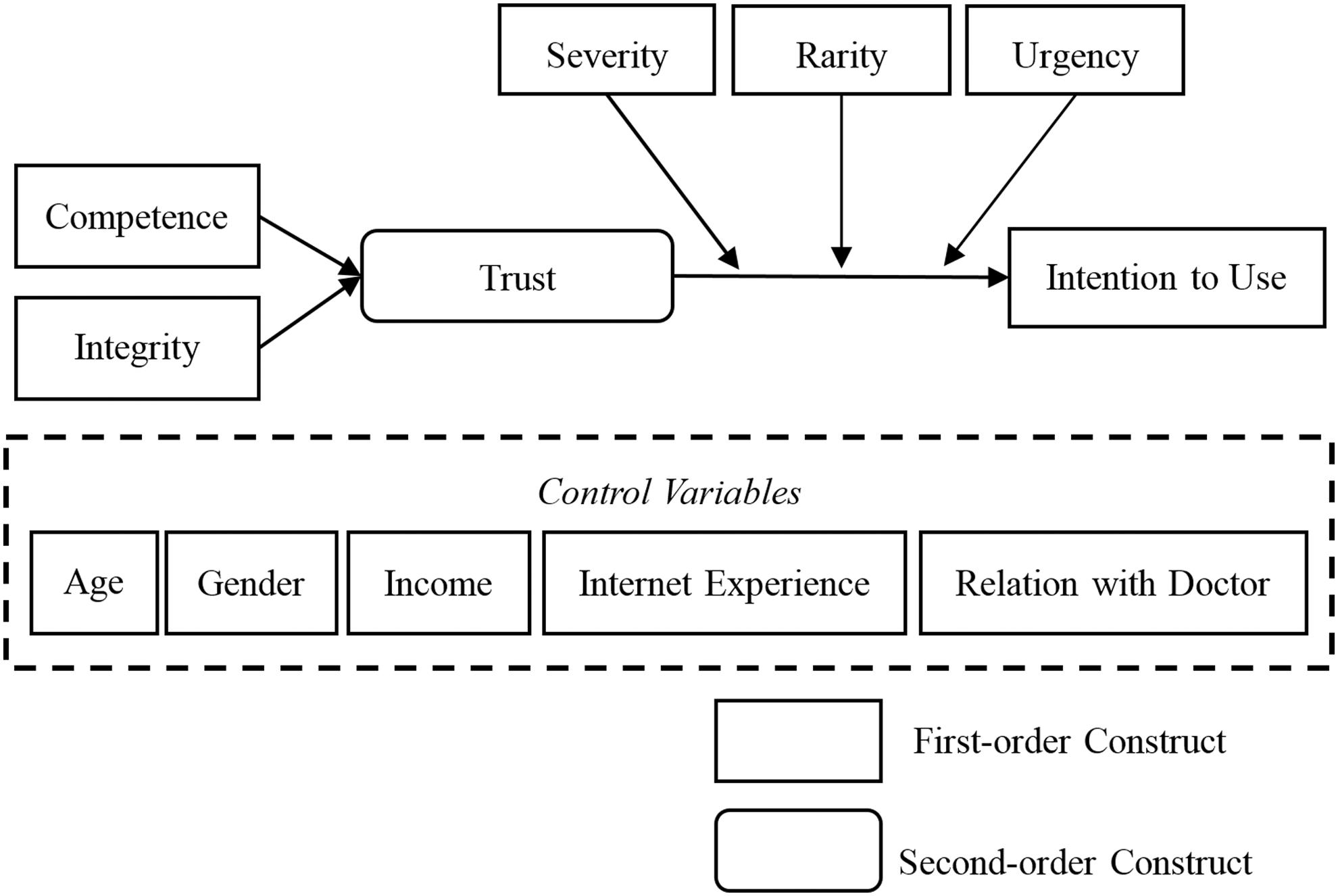
Research model.
Trust has been explored in many contexts relevant to uncertainty and risk. 19 In this study, trust means the users' perception that e-Consultation providers are trustworthy and would offer consultation services that are beneficial to users. Trust is a multifaceted concept. Adapting the definitions of trust from Wang and Benbasat 20 and McKnight et al., 21 we define trust in an e-Consultation service as an individual's beliefs in an e-Consultation service's competence and integrity. Competence belief means that an individual believes that the trustee has the ability, skills, and expertise to perform effectively in specific domains; and integrity belief means that an individual believes that the trustee adheres to a set of principles (e.g., honesty and promise keeping) that he/she finds acceptable. 21
This study focuses on initial trust beliefs that are formed after customers have a first impression regarding an e-Consultation service. Although we recognize the importance of the evolving nature of trust, this article focuses on initial trust because when users are not familiar with e-Consultation services during the initial contact, their perceptions of uncertainty and risk regarding using computer agents are the major concerns. 21 Without initial trust, users have a slight chance of using the e-Consultation service at all, and thus, the e-Consultation service has no opportunity to improve their trust in other interactions.
Trust has been investigated by many studies as the determinant of technology adoption. 22,23 Users often hesitate to interact with online providers because they are unfamiliar with the suppliers. 21 This is especially true in the context of healthcare, where each decision made is a serious one. As a consequence, lack of trust affects users' use of e-Consultation services. Therefore, trust plays an important role in the adoption of healthcare services because it can eliminate the uncertainty concerning the undesirable behavior of providers. The positive relationship between trust and use intention has been validated by several studies. 21,22,24 E-Consultation is a new IT delivering healthcare service; its acceptance involves the trust in providers of the e-Consultation service. Because health is a sensitive issue, people may pay more attention to providers of this service than Web-based providers in an e-commerce context. This means that the requirement of trust in a provider of an e-Consultation may be strengthened. Hence, we argue for a positive relationship between trust and e-Consultation adoption. Therefore, we have proposed the following hypothesis:
H1: Trust will be positively associated with the intention to use e-Consultation services.
In most cases, an e-Consultation acts as a supplement to traditional off-line healthcare services. The e-Consultation and off-line consultation are thus competitive and alternative to each other. If off-line consultation services satisfy user demands, then the intention to use e-Consultation services will be reduced. In contrast, if off-line consultation services cannot satisfy user demands, then the intention to use e-Consultation services will be strengthened.
In this study, we identify disease type as the contextual factor that may impact how user demand will be satisfied by off-line healthcare providers. In other words, a disease attribute as a contextual factor may confine the context where e-Consultation services are more suitable. In this study, we focus on the following three disease type attributes: severity, rarity, and urgency.
A rare disease is any disease that affects a small percentage of the population. According to the Rare Diseases Act of 2002, a rare disease is any disease or condition that affects fewer than 200,000 people in the United States or approximately 1 in 1,500 people. 25 When the focus disease is rare, the patient may experience difficulties in finding a suitable healthcare provider locally that has the treatment capability or experience. Therefore, the patient must turn to other healthcare solutions such as an e-Consultation. An e-Consultation provides a convenient way to reach national experts who have the knowledge, skills, and experience to cure a rare disease. Even if the patient has limited trust toward e-Consultation platforms or online doctors, the patient will still have a strong intention to use an e-Consultation service simply because he/she cannot find the appropriate healthcare providers locally. Therefore, we have proposed the following hypothesis:
H2: The higher the disease is in rarity, the lesser the positive effect of trust is on the intention to use an e-Consultation service.
Disease severity measures the serious consequences of a disease. Disease severity can be measured by the following aspects: disease progression, likelihood of death, likelihood of high inpatient expenses, likelihood of lengthy hospital stay, burden of disease (e.g., presence of comorbidities), etc. Because a severe disease may lead to unbearable consequences, the user perceives high risk when disease severity is high. To reduce this perceived high risk, the user is inclined to choose a better doctor because the patient usually believes a better doctor equals a better outcome. However, severe diseases are usually difficult to manage. Therefore, it may be challenging for the patient to find a qualified doctor locally and finding a nationwide famous expert may be necessary. Because an e-Consultation provides a convenient way to reach doctors nationwide, it is a supplemental way for the patient to address their severe disease. Even if the patient has insufficient trust toward e-Consultation platforms or online doctors, the patient will still have a strong intention to use e-Consultation services simply because he/she wants to reach nationwide exceptional experts. Therefore, we have proposed the following hypothesis:
H3: The higher the disease is in severity, the lesser the positive effect of trust on the intention to use an e-Consultation service.
Urgent diseases have ailments requiring urgent care and immediate attention. When the focus disease is urgent, the patient has no time to thoroughly compare different healthcare service providers. In urgent cases, ailments must be taken care of immediately because any delay may cause serious consequences. However, the patient may have difficulty finding a local healthcare provider (e.g., too far away or unavailable at the time). Therefore, alternative healthcare solutions, such as e-Consultations, would be ideal. Even if the patient has insufficient trust toward e-Consultation platforms or online doctors, the patient will still have a strong intention to use e-Consultation services because he/she needs immediate medical advice. Therefore, we have proposed the following hypothesis:
H4: The higher the disease is in urgency, the lesser the positive effect of trust is on the intention to use an e-Consultation service.
Research Methodology
In this section, we first discuss our data collection and then describe measures for the constructs.
Data collection
A scenario-based survey was conducted to test the proposed research hypotheses. A survey is well suited for testing human behavior related hypotheses and is thus the appropriate method for this study. The data for this study were collected through an online questionnaire. Previous findings indicate that data collected through online questionnaires have higher concurrency and predictive validity and less random and systematic measurement error. 26 The subjects were recruited voluntarily from a public forum in China. To better motivate the subjects, each subject who successfully completed the survey was rewarded with a 30-Yuan (approximately $5) rechargeable telephone card.
In the scenario-based survey, each subject was asked to recall a disease recently encountered by him/herself, his/her friends, or relatives. Based on that scenario, each subject was asked to evaluate the disease rarity, severity, and urgency using a 1–7 Likert scale. In addition, each subject was asked to answer the perceived trust of an e-Consultation service and his/her intention to use that service if he/she encountered the same disease again at this time. The demographic information of each subject was also collected in the survey.
We obtained a total of 190 valid questionnaires after removing incomplete cases. Participants belonged to different age groups and came from different positions. Demographic information of the subjects is presented in Table 1.
Respondent Demographics
Measure
Measures for the constructs are based on previous studies with adjustments to fit with the specific research context. All items were measured on a seven-point Likert-type scale with anchors of strongly disagree (one) to strongly agree (seven). The measures for the constructs are shown in Table 2.
Constructs and Items
ITU, intention to use; TCOM, trust competence; TINY, trust integrity.
Data Analysis and Results
For data analysis, we first analyzed the reliability and two types of validity, that is, convergent validity and discriminant validity. Then, we assessed the structural model and tested the hypotheses. In our research, the analysis of both a measurement model and a structural model was provided by SPSS and SmartPLS, which estimates the parameters in outer and inner models and is appropriate when the purpose of the research is exploratory. 28
Measurement Model
Reliability is the consistency of a set of measurements revealing a strong mutual interrelation between two outcomes measured by similar methods of the same construct. 29 To assess the reliability of the constructs, we verified the composite reliability (CR) and the average variance extracted (AVE). 28,30,31 As shown in Table 3, the CR exceeds 0.90, which is well above the suggested cutoff value of 0.70; the AVE is equal to or greater than 0.711, which exceeds the accepted threshold of 0.50, indicating good construct reliability. 28,30,31
Reliability and Convergent Validity
AVE, average variance extracted; CR, composite reliability.
Convergent validity relates to the degree to which a scale measuring the same construct provides the same results. 32 The item loadings are examined to assess the convergent validity of constructs, and a value less than 0.7 is considered insufficient. 21,22,33 The item loadings in our research ranged from 0.821 to 0.922, which were higher than 0.70 and in support of convergent validity.
Discriminant validity is the extent to which the measurement differs between two different constructs. 21,32 From prior research, discriminant validity is tested by comparing the square root of the AVE and the correlations of this variable with any other model's constructs. 28,30,34 In Table 4, we determined that all of the square roots of the AVE were higher than the correlations; therefore, discriminant validity is acceptable. Therefore, our measurement model has been verified as reliable.
Discriminant Validity
The bold diagonal data refer to the square roots of the average variance extracted.
The validity of the second-order formative construct collective efficiency was evaluated by comparing the weights and variance inflation factors (VIF). 35 As shown in Table 5, the weights for all three dimensions were significant, and the VIF for all dimensions were below 5, suggesting that the validity of the second-order construct was suitable.
Second-order Formative Constructs
p < 0.01.
VIF, variance inflation factors.
Structural model
To examine the impacts of trust (the interaction effect of trust and rarity, the interaction effect of trust and severity, and the interaction effect of trust and urgency), we compared the Partial Least Squares (PLS) regression results of five models (as shown in Table 6). In Model 1, only the control variables were included. The results showed that five factors (age, income, sex, Internet experience, and relation with patient) explained 8.2% of the variance of the dependent variable, while Internet experience was found to be significant. In Model 2, trust (β = 0.770, p < 0.01) was further included, and the results showed that its impact on intention to use was significant, lending support to H1. The inclusion of trust increased the R-square value from 0.082 to 0.626 (ΔR 2 = 0.544, f2 = 0.593), suggesting that trust has a significant effect on intention to use e-Consultation services.
Partial Least Squares Results
Cohen's f2-statistic =
p < 0.05.
p < 0.01.
In Model 3, the interaction effect of trust and disease rarity is included. The results showed that the interaction effect was significant (β = 0.251, p < 0.05), lending support to H2. The inclusion of the interaction effect increased the R-square value to 0.652 (ΔR2= 0.026, f2 = 0.070). This result suggests that trust and disease rarity have a significant interaction effect on the intention to use e-Consultation services. As disease rarity increases, trust has a less positive effect on the intention to use an e-Consultation service. This interaction effect is also illustrated in Figure 2.
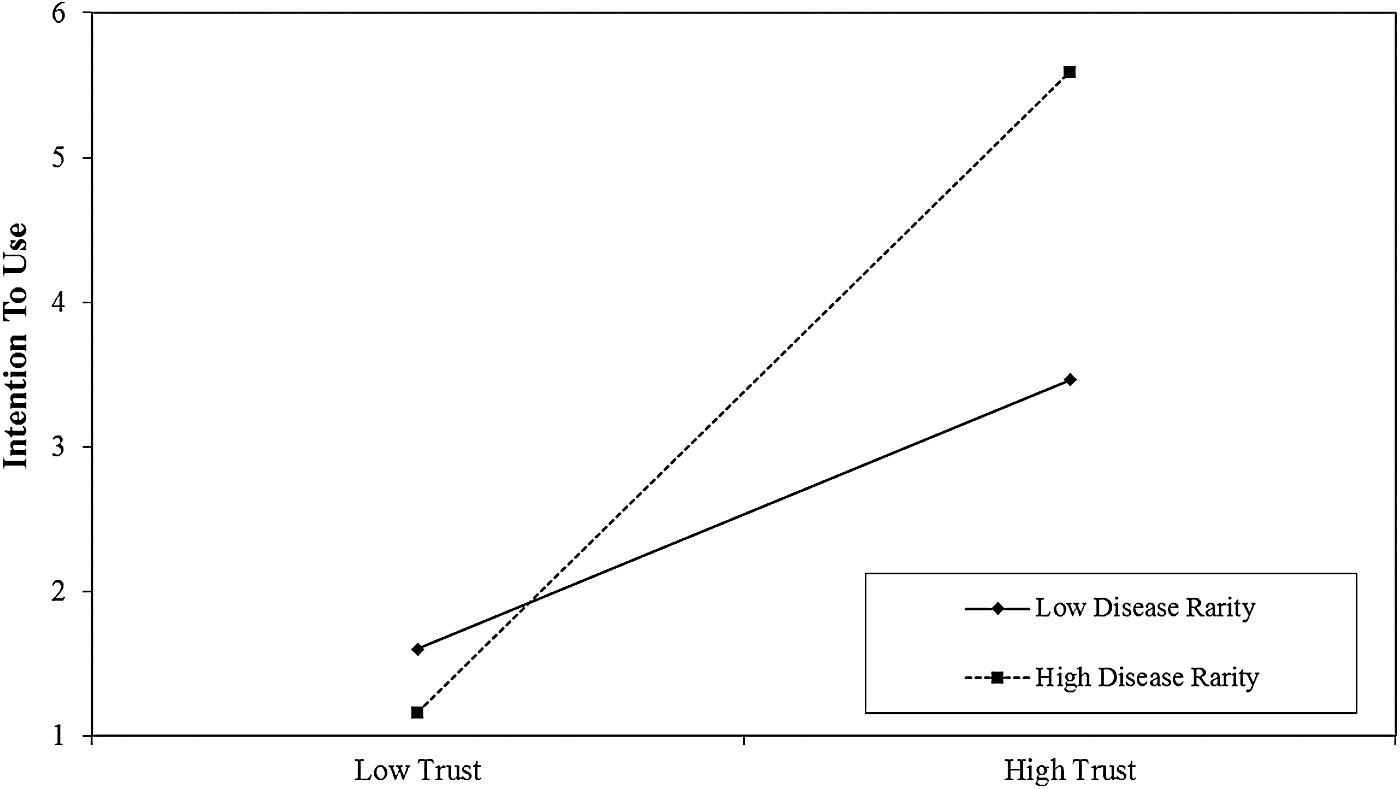
Interaction effect between trust and disease rarity.
In Model 4, the interaction effect of trust and disease severity was included. The results showed that the interaction effect was significant (β = 0.368, p < 0.01), lending support to H3. The inclusion of the interaction effect increased the R-square value to 0.656 (ΔR2= 0.030, f2 = 0.080). This result suggests that trust and disease severity have a significant interaction effect on the intention to use e-Consultation services. As disease severity increases, trust has a less positive effect on the intention to use an e-Consultation service. This interaction effect is also illustrated in Figure 3.
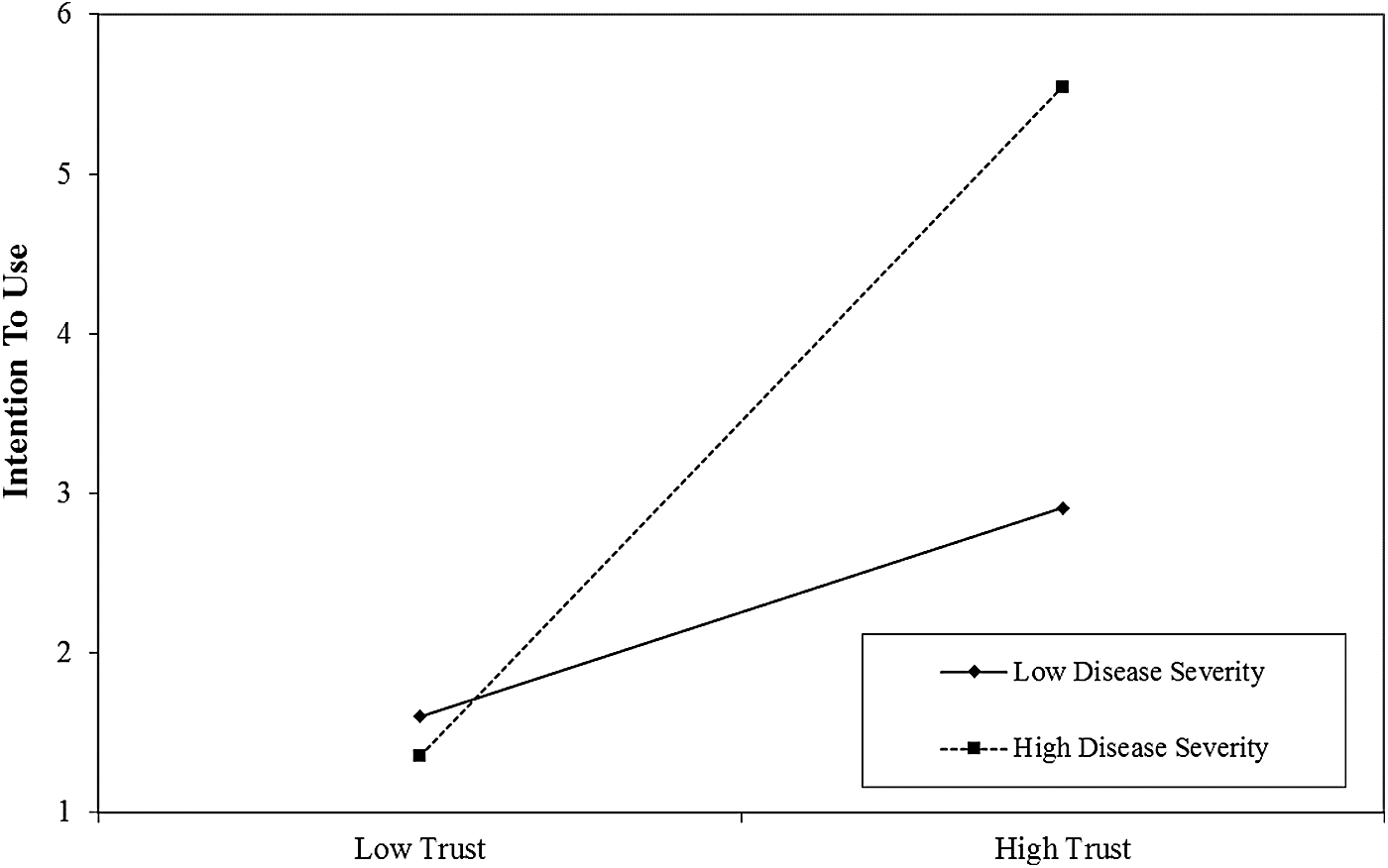
Interaction effect between trust and disease severity.
In Model 5, the interaction effect of trust and disease urgency was included. The results showed that the interaction effect was significant (β = 0.333, p < 0.05), lending support to H4. The inclusion of the interaction effect increased the R-square value to 0.656 (ΔR2= 0.018, f2 = 0.048). This result suggests that trust and disease urgency have a significant interaction effect on the intention to use e-Consultation services. As disease urgency increases, trust has a less positive effect on the intention to use an e-Consultation service. This interaction effect is also illustrated in Figure 4.
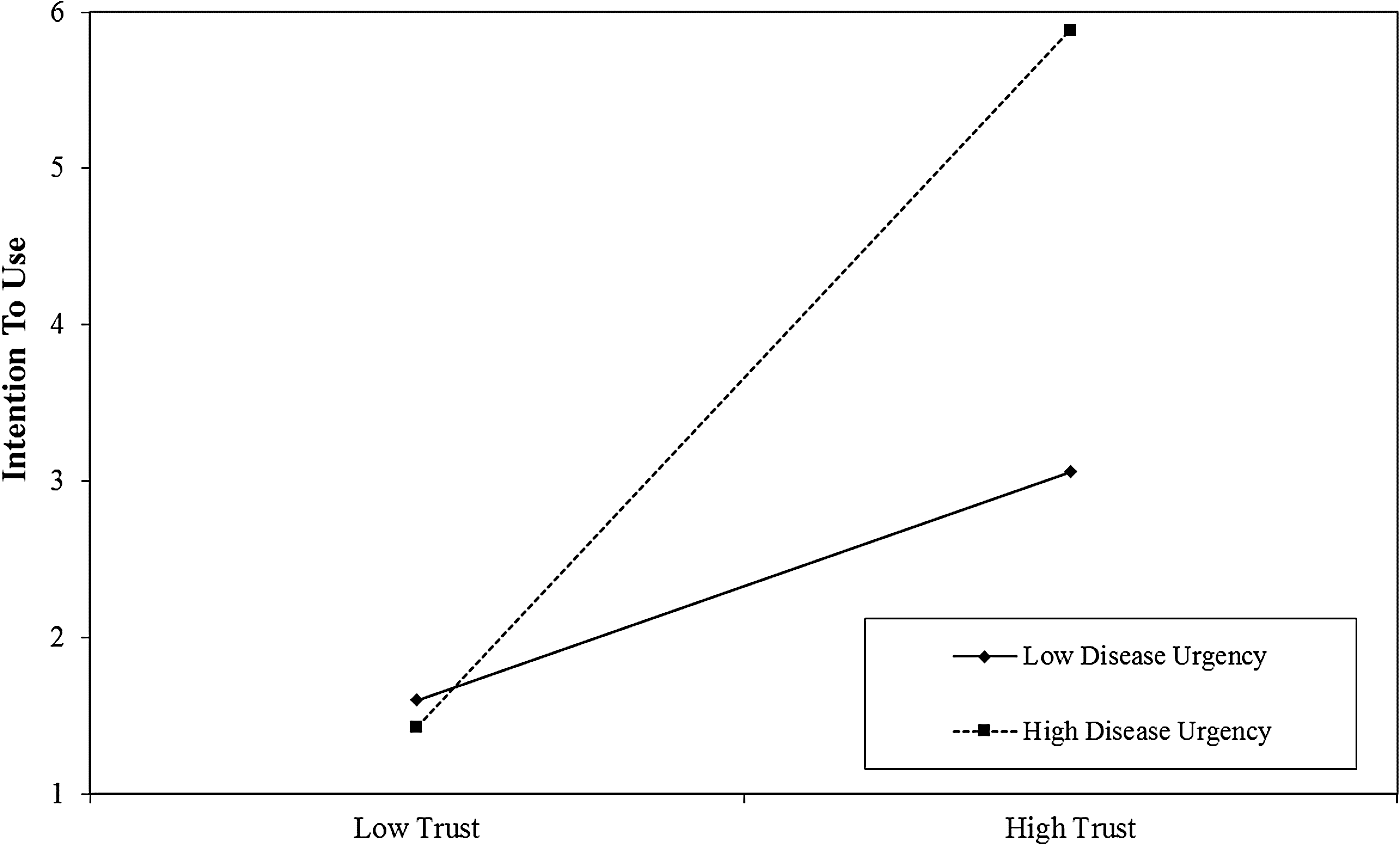
Interaction effect between trust and disease urgency.
Research Analysis and Discussion
Key findings
There are several major findings of this study. First, trust has a positive effect on the intention to use e-Consultation services. Trust regarding e-Consultation platforms and online doctors consists of two dimensions as follows: competence and integrity. The higher the trust of competence and integrity, the higher the intent of use toward an e-Consultation service.
Second, the higher the disease is in rarity, severity, or urgency, the lesser the positive effect of trust is on the intention to use an e-Consultation service. That is because when the disease is high in rarity, severity, or urgency, an off-line healthcare provider is less capable of providing meaningful, qualified, and immediate service. Therefore, an e-Consultation service will have a higher supplementary effect for rare, severe, or urgent diseases.
Theoretical Contribution
This study makes several theoretical contributions. First, this is the first empirical study investigating the important and emerging phenomenon of e-Consultation adoption. Although e-Consultation services are rapidly growing, very few studies have focused on early adoption. Previous studies investigating the drivers and inhibitors of e-Consultation success are mainly from the healthcare provider's perspective.
Second, this study uses a trust perspective to explain the e-Consultation service adoption phenomenon. Previous studies on HIT (Healthcare Information Technology) adoption usually extend a well established theory (e.g., Technology Acceptance Model) to a new healthcare context. In this study, we consider choosing a healthcare provider as a serious decision, and trust acts as the central role in the process. Therefore, a trust-based perspective rather than a system usage perspective is used in this study.
Third, based on the resource supplementary perspective, this study, for the first time, links medical variables to the information system adoption research. Previous studies on IT adoption in healthcare seldom consider the domain context (i.e., healthcare) variables. In this study, we identify three disease variables (rarity, severity, and urgency) that moderate the impact of trust on e-Consultation adoption. Our results demonstrate that the link between trust and usage intention will decrease when disease rarity, severity, and urgency are high.
Implications
The findings of the current study provide several practical implications. First, trust plays a central role in a user's adoption of e-Consultation services. In addition, trust of e-Consultation services can be further divided into two dimensions as follows: capacity trust and integrity trust. E-Consultation websites that want to attract more users must build user trust on both capacity and integrity dimensions. Namely, the platform must send signals to users that online doctors not only have enough knowledge, skills, and experience to address complex medical encounters but also follow consistent rules that are suitable for the patients.
Second, the results of this study indicate that e-Consultation platforms can use their services for rare, severe, or urgent diseases or place more efforts on these diseases. That is because rare, severe, or urgent diseases are more suitable for an online context and have higher supplemental effects compared with traditional off-line healthcare providers.
Limitations and Future Research
There are several limitations of this research. First, all variables used in this study contain only self-reported data. Future studies should include the actual usage behavior (rather than the intention to use in this study) to increase research validity.
Second, this study investigates only the moderating effect of disease type on trust. In addition, other variables (e.g., doctor's off-line position and title, online reputation) may moderate the relationship between trust and usage intention. Therefore, future studies could benefit from investigating the moderating effects of these variables.
In this study, we investigate important and emerging researching questions, such as why and when customers use e-Consultation services. Considering that the choice of a healthcare provider is a serious decision, this research uses the trust perspective to explain the e-Consultation service adoption phenomenon. Specifically, trust is conceptualized as a second-order construct consisting of two dimensions as follows: competence and integrity. In addition, an e-Consultation is viewed as a supplementary resource to traditional off-line consultation services, and disease type as a contextual factor is hypothesized to confine the context where e-Consultation services are more suitable. A survey was conducted to test the proposed research model. The results indicate that trust has a positive effect on the intention to use an e-Consultation service. Meanwhile, the higher the disease is in rarity, severity, or urgency, the lesser the positive effect of trust is on the intention to use an e-Consultation service.
If website managers better understand the mechanisms and antecedents of e-Consultation usage, they can take actions to create a better reputation for users that online doctors not only have enough knowledge, skills, and experience to address complex medical encounters but also have consistent rules that are suitable for patients. In addition, managers should also invest their limited resources more into rare, severe, or urgent diseases because e-Consultation services have higher resource supplementary effects on those diseases.
Footnotes
Acknowledgment
This research was supported by the National Natural Science Foundation of China with grants 71371005, 71471064, and 91646205.
Disclosure Statement
No competing financial interests exist.