
Abstract
Purpose:
The accessibility of ophthalmologists appears to influence the quality of screening for diabetic retinopathy (DR). The principal objective of this study was to analyze the effect of automobile travel time to the closest ophthalmologist on the time to DR screening.
Methods:
This historical cohort study used reimbursement databases from the principal national health insurance fund. Patients were included if they had been reimbursed at least thrice for oral antidiabetic medications in the 12 months before the study start date. Patients were followed up from January 1, 2008, for 4 years. The expected event was a DR screening by an ocular fundus examination. The automobile travel time to the nearest ophthalmologist was calculated by the distance between communes, estimated by appropriate software. A Kaplan–Meier curve and a multivariate Cox model were used to model the effect of travel time on the time until DR screening. A sensitivity analysis of travel time described the results of the Cox model.
Results:
At the start of 2008, 6,573 patients living in 328 different municipalities were included. The multivariate model found that patients living 60 min or more away from an ophthalmologist had a lower instantaneous probability of DR screening than those living <30 min away (adjusted risk ratio = 0.82; 95% confidence interval 0.71–0.95; p = 0.009). The sensitivity analysis showed that this difference became significant at 35 min of travel time.
Conclusion:
Increased automobile travel time for patients with diabetes to the nearest ophthalmologist was associated with a longer time to DR screening.
Introduction
The prevalence of treated diabetes is increasing in France, rising from 3.78% in 2006 to 4.6% in 2012. 1 The long-term complications of this disease, such as diabetic retinopathy (DR), cause disabilities that can impair patients' quality of life and generate large healthcare costs. 2 DR evolves toward a progressive decrease in visual acuity caused by macular damage or sudden blindness through the proliferation of microvessels. 3,4 In European countries, DR is one of the five principal causes of blindness, together with cataracts, age-related macular degeneration, glaucoma, and degenerative myopia. 5 It is the leading cause of blindness before the age of 60 in developed countries. 6 In a representative national sample of French patients with type 2 diabetes treated pharmacologically in 2007, the prevalence of DR was 7.9%. 7 The cumulative incidence of blindness and severe visual impairment (acuity visual <20/40) 10 years after the onset of diabetes is reported to be 1.8% and 9.4% in patients with type 1 diabetes and 4% and 24% in those with type 2 diabetes. 8,9
Glycemic control, strict blood pressure control, and panretinal photocoagulation at early stages of proliferative retinopathy and moderate macular edema can help to prevent the aggravation of DR. 10 Screening is essential in view, especially, of the possibility of intravitreous antivascular endothelial growth factor (ranibizumab) treatment. Treatment of eyes with proliferative DR by ranibizumab resulted in visual acuity that was not inferior to panretinal photocoagulation treatment at 2 years. Although longer term follow-up is needed, ranibizumab may be a reasonable treatment alternative, at least through 2 years, for these patients. 11,12 Screening is thus indicated. It is routinely performed by ophthalmologists, by indirect ophthalmoscopy with a slit lamp and pupil dilatation or by fundus photography, with or without pupil dilatation. French guidelines, like those in most countries, recommend annual screening for DR for all patients diagnosed with type 2 diabetes and for those with type 1 diabetes starting 10 years after its onset. For those patients who do not have DR, are not treated by insulin, and have quarterly HbA1c levels that meet treatment objectives and adequate blood pressure control, screening may be performed every other year. 13
This screening is insufficient in France; only 44% of patients with diabetes had an ocular fundus examination in 2007, although the objective is 80%. 7 Several patient-related factors negatively influence this screening: male sex, low socioeconomic status, 14 fear of discovery of an abnormality, and the feeling that screening is useless. 7 Other obstacles are associated with healthcare availability: long waiting times for appointments, 7 low density of ophthalmological services, 15 and difficult geographic access. 16 There have been few studies of the latter, even though they have become modifiable, since the development of fundus photography and telemedicine has made DR screening more widely available.
Applicability: Teleretinography
The French health authorities have assessed a screening strategy that includes teleretinography (or delayed-reading retinography). 13 According to the working group, screening based on teleretinography should be promoted because it will help to improve screening for DR. The reduction in travel time toward the closest retinography equipment and the absence of the need for an ophthalmologist's presence to take the images will enable more patients to be screened. Ophthalmologists should thus be more available for the most serious cases, which require a standard visit. Teleretinography is already widely used in some countries. Studied in the first decade of this century in the very rural province of Alberta in Canada, it was finally adopted nationwide 17 and has enabled numerous Canadians living in very isolated areas to receive DR screening. Similar campaigns have taken place in some communities in the United States, 18,19 Australia, 20 Germany, 21 Canada, 22 and the United Kingdom 23 and have shown the value of itinerant screening in rural areas that lack ophthalmologists. In France, the first campaign to screen for DR by itinerant teleretinography using a specially equipped van took place in the region of Burgundy in 2004. Our hypothesis for this study is that when a physical distance separates the patient from the specialist performing an examination, here of the ocular fundus, it is performed less often.
France has a deficit of ophthalmologists (mean national density 8.8/100,000) that will worsen over the next decade, since 70% of ophthalmologists are more than 50 years old (
The principal objective of the study was to analyze the effect of automobile travel time to the nearest ophthalmologist's office on the time to DR screening.
Materials and Methods
Design of the Study and Database
We conducted a historical cohort study of records covering the 4-year period between 2008 and 2011. The source population was all individuals covered by the French national health insurance fund for employed workers who lived in two mountainous districts of France: Alpes de Haute Provence and Hautes Alpes. This health insurance fund covers around 75% of the French population. 24 The study used databases of reimbursements paid to patients for medical and drug costs, as well as for laboratory and medical procedures. These databases record all the drugs dispensed by private pharmacies, all laboratory tests performed by private laboratories, and all medical procedures performed on an outpatient basis by physicians (i.e., ophthalmoscopy, retinal evaluation using a biomicroscope, fundus photography, or direct ophthalmoscopy), regardless of their specialty or type of practice (private or hospital). It does not include the procedures and care performed on an inpatient basis, during hospitalizations.
Inclusion and Censoring
Patients with diabetes were included according to a previously used algorithm. 25 To be included at the study start date, patients had to be at least 18 years of age and have received at least three reimbursements for medications for diabetes dispensed at different dates during the previous 12 months, that is, during the 2007 calendar year. This algorithm included reimbursement for all oral antidiabetic medications (OADMs) and insulin. Benfluorex was excluded from the algorithm. Recognition of the serious cardiac and pulmonary toxicity of benfluorex led to the discontinuation of its marketing in several countries in the 1990s, but it was removed from the market in France only in 2009. Significant conflicts of interest resulted in its inappropriate licensing for the treatment of diabetes, although it was actually an anorectic and was prescribed off-label to young women wishing to lose weight. Introducing it into our algorithm would induce a selection bias. During the follow-up period, right censoring was applied for patients who died, moved, or changed their health insurance fund.
Individual Data
At inclusion the following variables were available for each patient: municipality of residence, age, sex, attribution of chronic-disease status (affection de longue durée [ALD]) (granted to people with specific and expensive chronic diseases, entitling them to 100% reimbursement for treatment), complementary universal health insurance (CMUC) coverage status (a program that exempts individuals with annual incomes below 9,000 € from any out-of-pocket costs and, thus, a proxy for low income), 26 visits to/from a general practitioner during the year preceding inclusion, visits to an endocrinologist (at least one during the year preceding inclusion), and the severity of diabetes, assessed by the maximum number of different drugs dispensed on a single date during the year before inclusion: a single OADM for mild diabetes, two different OADMs for moderate diabetes, and more than two different OADMs and/or insulin for severe diabetes. The standard combination OADMs were taken into account.
End Point
The principal end point was the interval between inclusion (January 1, 2008) and the first DR screening. The French healthcare system allows ophthalmologists to charge fees above the normal ceiling for reimbursement; some ophthalmologists bill for visits at this additional fee without necessarily reporting the ocular fundus examination. For this reason, we chose to treat all visits to ophthalmologists by patients with diabetes as including DR screening.
Ophthalmologists and Automobile Travel Time
The national council of physicians helped us to identify all of the ophthalmologists practicing in the two study districts and in all of the districts bordering them. We contacted each ophthalmologist by telephone to verify that they performed ocular fundus examinations, had not closed or changed their practice, or moved during the study period. We also verified with healthcare facilities that no teleophthalmology programs had begun during the study period. The distance between municipalities was calculated with ODOMATRIX® software, version 2013. 27 This software models the French road network with several layers of geographic information describing the roads, the relief, and the land use. A driving speed is attributed to each road segment. The automobile distance between all possible pairs of municipalities is described by a matrix. We collected for each patient the travel time by automobile between the patient's municipality of residence and the municipality of practice of the closest ophthalmologist. Given the small number of municipalities with heavy road traffic, travel time was calculated for off-peak hours. We verified for each patient whether travel time to the ophthalmologists in neighboring districts was longer than intradistrict travel time; we used the former if it was faster. The minimum travel time was estimated at 5 min if the patient's home and ophthalmologist's office were in the same municipality.
Statistical Analyses
For the descriptive analyses and in the absence of earlier studies on this topic, we chose to divide automobile travel time to the closest ophthalmologist arbitrarily into three categories: <30; ≥30 and <60; and ≥60 min. The differences between the patients in each of these three categories were compared with a Chi-squared test for the categorical variables and Student's t test for the continuous variables.
The effect of travel time on the time to ocular fundus examination was described graphically by the Kaplan–Meier method with a log-rank test. Next we used a Cox model for a univariate and then a multivariate analysis. The variables of adjustment were sex, age (six categories), ALD status (yes/no), diabetes severity (three categories), number of general practitioner (GP) consultations in the year before the study (continuous variable), and endocrinologist consultation in the year before the study (yes/no). The variables with statistical associations with a p-value <0.2 in the univariate analysis were introduced into the multivariate analysis. The proportional risk hypothesis was verified with the Schoenfeld residual test 28,29 for each variable, with a graphic representation of the residues as a function of time.
The strength of the association between travel time to the ophthalmologist and DR screening was tested by a global sensitivity analysis that used the multivariate model described above. The instantaneous adjusted relative risk (aRR) for DR screening was estimated by increasing travel time to the ophthalmologist successively in 5-min increments.
The statistical analyses were performed with SAS® software, version 9.4 (SAS Institute, Inc., Cary, NC). The threshold of significance for the statistical tests was set at p < 0.05. The Cox model was created with the PROC PHREG procedure. Our study used secondary data held by French national health insurance fund for which we were granted access by the French Data Protection Authority (Commission Nationale de l'Informatique et des Libertés [CNIL]) and permission to conduct this prespecified analysis (authorization n°1196790). As our study was an analysis of secondary data without personal identifiers for which authorization had been already granted by the relevant statutory authority (CNIL), the Ethics Committee of the University of Marseille deemed that ethical approval was not required. This is in line with the Declaration of Helsinki and nonidentifiable data.
Results
Ophthalmologists
We identified 19 ophthalmologists practicing in the 2 districts, in 6 municipalities: Sisteron (2 ophthalmologists), Manosque (8), Digne-les-Bains (1), Gap (5), Briançon (2), and Embrun (1) (Fig. 1). Telephone calls confirmed that all of them performed ocular fundus examinations, either by indirect examination with a slit lamp or by fundus photography, and that during the study period, none had begun or stopped practicing or moved.

Map illustrating the automobile travel time to the nearest ophthalmologist for each French municipality in the two study districts.
Patients
On January 1, 2008, the study included 6,573 patients residing in 328 municipalities. Follow-up was complete for 5,761 (87.6%), either to the end of the study period or until DR screening. There were 812 patients censored: 5.5% (of the total patients) because they moved, 4.2% because they changed insurance funds, and 2.6% who died. The mean automobile travel time to the nearest ophthalmologist's office was 18.6 min (standard deviation [SD] = 17.8). Overall, 83% patients lived less than 30 min by automobile from the ophthalmologist's office, 12.9% from 30 to 60 min away, and 4.1% more than an hour away. These three subgroups did not differ significantly for sex, age, percentage of CMUC recipients, percentage with ALD status, or severity of diabetes (Table 1). Patients living at least an hour from the ophthalmologist saw a GP more often than the others; inversely, they saw an endocrinologist less often. The three groups did not differ significantly for the three reasons for censoring: moving, change of insurance, and death.
Global Characteristics of the Sample and Then Characteristics as a Function of Automobile Travel Time to the Nearest Ophthalmologist (N = 6,573)
p-Value from a Chi-square test assessing the difference in distribution of patient characteristics as a function of travel time to the nearest ophthalmologist.
Number calculated for the subgroups younger than 65 years because above this age the minimum old age pension for the poorest individuals is higher than the threshold for receiving CMUC.
Proxy for severity: intensity of prescribed treatment: a single OADM for mild diabetes, two OADMs for moderate diabetes, and more than two OADMs and/or insulin for severe diabetes.
Variables calculated for the 12 months before the study started.
CI, confidence interval; CMUC, complementary universal health insurance; OADM, oral antidiabetic medication; SD, standard deviation.
Analysis of the End Point
The median time from study start to DR screening was 13 months for the patients living less than 30 min from the ophthalmologist's office, 14 months for those living 30 to 60 min away, and 18 months for those at least an hour away (Fig. 2). The log-rank test significantly rejected (p = 0.013) the null hypothesis that the survival curves (Fig. 1) were identical for the three travel-time categories. The cross-sectional description at 12 months shows that 47% of the patients living less than 60 min away from the nearest ophthalmologist had had a DR screening, compared with 37% of those an hour or more away.
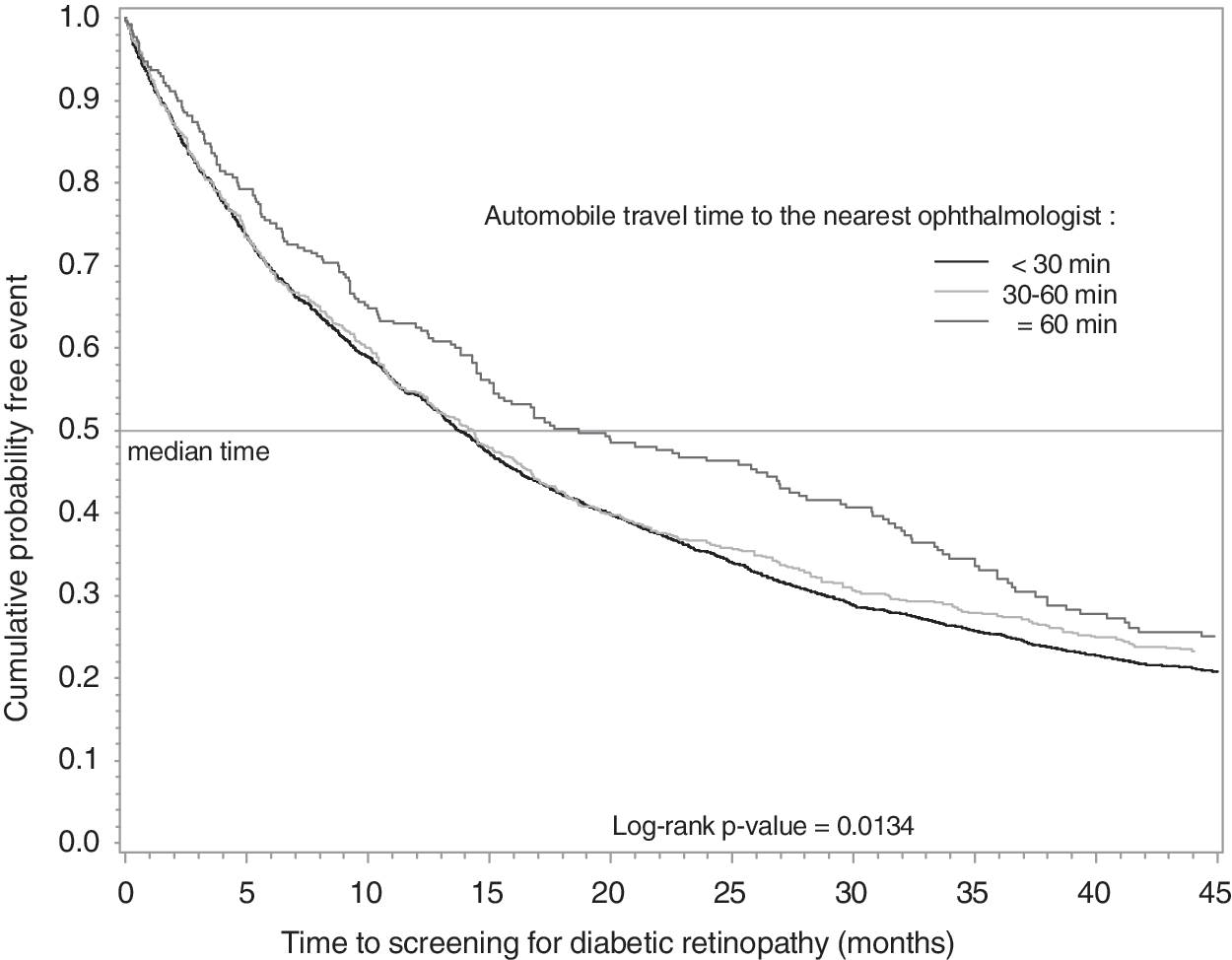
Kaplan–Meier curve expressing the effect of travel time (in three categories) on the time to screening for diabetic retinopathy.
Cox Model
The graphic representation of the residues for all the variables as a function of time shows that their distribution did not vary significantly over time and did not require correction (results not shown but available from the authors). All the variables were retained by the univariate analysis and were thus introduced into the multivariate model (Table 2). The multivariate model found that patients living 60 min or more from an ophthalmologist had a lower instantaneous probability of DR screening than those living less than 30 min away (aRR = 0.82; 95% confidence interval [CI] 0.71–0.95; p = 0.009). The patients living between 30 and 60 min from an ophthalmologist also had a lower instantaneous probability of DR screening, but this difference was not statistically significant (aRR = 0.97; 95% CI 0.86–1.06; p = 0.57).
Association Between Patients' Characteristics and the Time Until Screening for Diabetic Retinopathy, Instantaneous Relative Risks Expressed by a Cox Model
Proxy for severity: intensity of prescribed treatment: a single OADM for mild diabetes, two OADMs for moderate diabetes, and more than two OADMs and/or insulin for severe diabetes.
Variables calculated for the 12 months before the study started.
ARR, adjusted relative risk; CMUC, complementary universal health insurance; RR, relative risk.
Sensitivity Analysis
The sensitivity analysis (Fig. 3) showed that the instantaneous aRR for a DR screening became significantly less than 1 for patients living more than 35 min from an ophthalmologist, that is, for 12% of the sample. The relationship between the instantaneous probability of DR screening and travel time to an ophthalmologist's office was linear. The very small number of patients living more than 90 min away was responsible for the instability of the results longer than that.
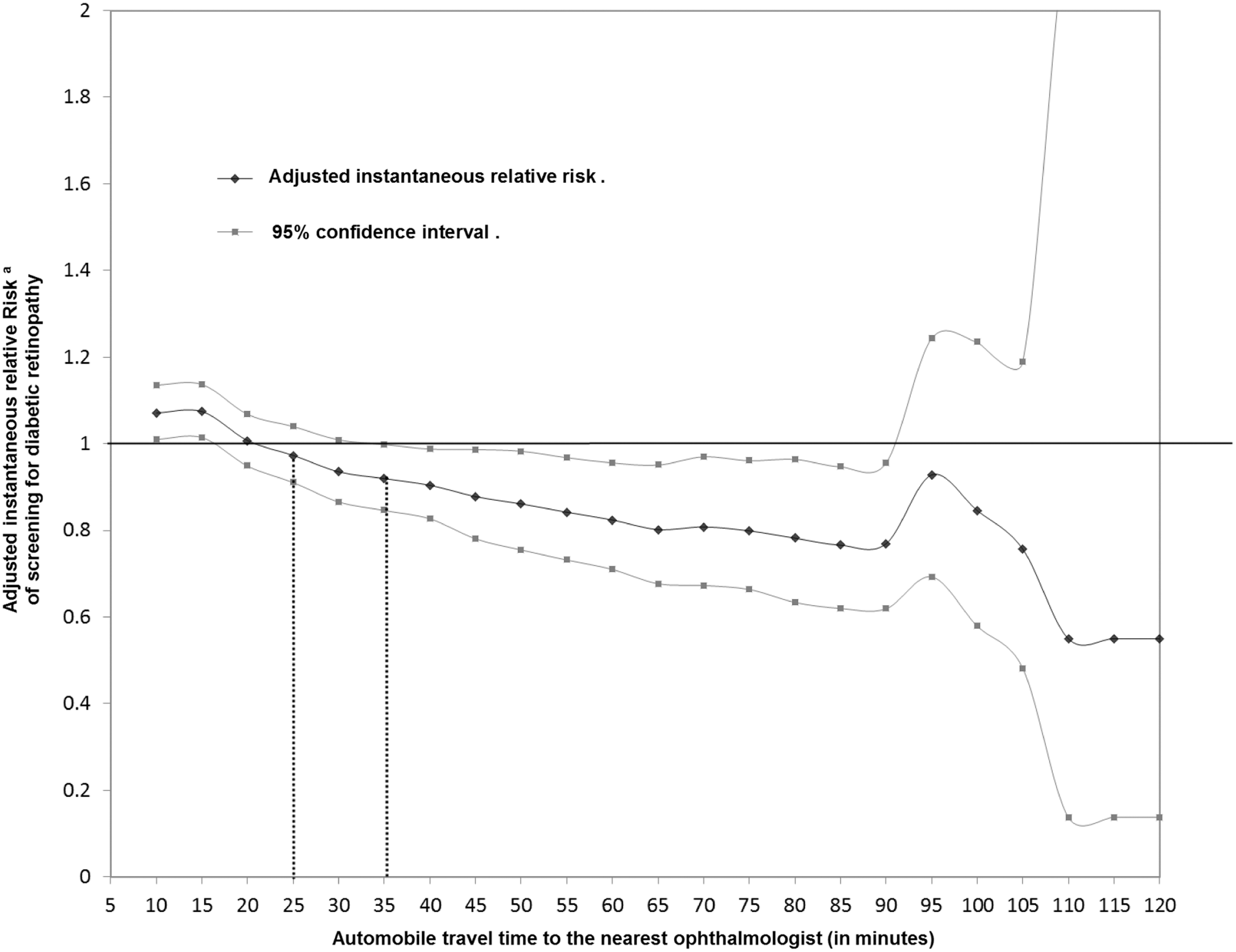
Sensitivity analysis of the effect of travel time to the nearest ophthalmologist on screening for diabetic retinopathy, with a multivariate Cox model.a aThe variables of adjustment were sex, age (six categories), ALD status (yes/no), diabetes severity (three categories), number of GP consultations in the year before the study (continuous variable), and endocrinologist visit in the year before the study (yes/no). GP, general practitioner.
Analysis of the Adjustment Variables
Women had a higher instantaneous probability of DR screening than men: aRR = 1.14; 95% CI 1.07–1.20. The youngest patients in the sample (<45 years), as well as the oldest (>85 years), were screened least often. ALD status increased the instantaneous probability of DR screening (aRR = 1.179; 95% CI 1.070–1.299). This probability also increased with the severity of diabetes (moderate aRR = 1.085; 95% CI 1.085–1.163; severe aRR = 1.172; 95% CI 1.091–1.258). For each additional GP visit, this probability increased by 0.005%. Finally, endocrinologist visits also improved DR screening (aRR = 1.655; 95% CI 1.531–1.790).
Discussion
Principal Results
The automobile travel time to the nearest ophthalmologist's office significantly influenced the time to DR screening in this study sample. The sensitivity analysis showed that living more than 35 min from an ophthalmologist's office significantly reduced the aRR for DR screening, and 12.05% of our sample lived that far away. Beyond 35 min, the instantaneous probability of DR screening decreased linearly with the increase in travel time.
The choice of two mountainous districts with an especially low density of ophthalmologists (6.7/100,000 compared with 8.8/100,000 nationally) facilitated our observation of these results. The lower density of ophthalmologists together with the rugged terrain resulted in highly variable travel time. The proportion of patients living more than 30 min from an ophthalmologist was substantially higher in our sample (17%) than nationally (6%). As of now, the authorities have decided that screening campaigns by teleretinography must be organized at the local level, according to the specificities of each district. The methodology of our study can be reproduced in other French areas that may have similar difficulties of access to ophthalmologists. The choices of geographic sites for this instrument may be based, in each area, on the results of studies similar to ours.
Secondary Results
Other factors influenced the time to DR screening: sex (female), age (45–85 years), severity of diabetes, and ALD status improved the quality of screening (i.e., shortened time to screening) to a statistically significant level. The intensity of GP monitoring, measured by number of GP visits, also shortened time to ophthalmological screening linearly. The descriptive analysis of the sample shows that patients who lived an hour or more from their ophthalmologist saw their GP more often than those living less than 30 min from the eye specialist. This finding suggests that in remote areas GPs substitute for specialists in the follow-up of complex chronic diseases. Nonetheless, the lack of technical equipment and facilities prevents some preventive care, including DR screening.
Because private-practice endocrinologists, like ophthalmologists, tend to work in large cities, we considered the possibility of overadjustment before introducing endocrinologist visits into the model. When this variable was removed from the multivariate model, the strength of the association between travel time and time to DR screening increased to a minimal extent (results not presented). We finally decided to retain the endocrinologist visit variable because the confounding factor associated with improved quality of follow-up in patients with diabetes with easier access to endocrinologists seemed to us to present a greater risk of overadjustment.
Comparison with the Literature
Some studies have clearly shown that accessibility to ophthalmologists influences the frequency of ophthalmic care and follow-up. In 2008, Lee and Kumar 30 compared patients with diabetes without DR living more or less than 12 km from an ophthalmologist in the Miami (Florida) region. Patients living more than 12 km away underwent DR screening less often (OR = 0.36; 95% CI 0.14–0.86). These results were nonetheless questionable because of the classification bias in that study: subjects with an unknown DR screening status were considered not to have been screened. A U.S. study 31 examined the access to ophthalmological care of patients older than 65 years with DR, glaucoma, age-related macular degeneration, or cataracts. Patients living more than 20 miles (32 km) away were less likely to visit an ophthalmologist (aRR = 0.63; 95% CI 0.43–0.95 in the multivariate analysis) than those who lived closer. Gibson. 32 showed that in the United States, the density of ophthalmologists was significantly associated with the probability of an annual ocular fundus examination in patients with diabetes and without retinopathy; the probability increased by 10% for each additional ophthalmologist per 100,000 inhabitants (OR = 1.05; 95% CI 1.00–1.10). Finally also in the United States, Chou et al. 15 showed the positive influence of ophthalmologist density on DR screening among patients with diabetes. Analysis of the literature shows that accessibility to ophthalmologists depends on both distance and their density.
Study Strengths and Limitations
The source population was a strength of this study, for the insurance fund whose database we used covered more than 75% of the population of the area studied. The sample can be considered representative of the population of people with diabetes treated in that area. The reimbursement databases of the national health insurance fund provide high statistical power and enable the use of a robust adjusted statistical model. The algorithm did not allow us to identify patients with diabetes managed only by dietary and lifestyle measures, but this group accounts for only 0.6% of the general population aged 18–74 years. 33 False positives were rare (mainly associated with biguanides used to treat polycystic ovary syndrome). The variable of travel time provided more precision compared with distance used in earlier studies. Depending on the road infrastructure and season, it can take more or less time to travel the same distance. Finally, the linear relationship between travel time to an ophthalmologist's office and the instantaneous probability of DR screening is epidemiologic evidence of robustness.
The principal limitation of the study is that the waiting times for ophthalmologist appointment were not taken into account, although they affect patients' choices between specialists. The national institute of statistics and economic studies (l'Institut national de la statistique et des études économiques; INSEE) has reported that in metropolitan France, only 67% of patients visit the ophthalmologist nearest to their home. 34 These long waiting times, associated with the low density of ophthalmologists, have led to a reorganization of this healthcare pathway. Patients sometimes make longer trips to have their DR screening performed within an acceptable period. Patients' socioeconomic status was not taken into account in these analyses, although it modifies the quality of follow-up for diabetes. 7 The only marker of socioeconomic status available was CMUC, and it is not available to subjects older than 65 years; its consideration would have excluded 60% of the sample. Nonetheless, the proportion of CMUC recipients did not differ significantly between the three subgroups of patients younger than 65 years. The bias that might have been induced by the strong social disparities in the suburbs of large metropolitan areas was minimized by the choice of these two study districts, where the size of towns remains small. This enabled us to limit the “center” effect of large urban area. Finally, this study did not take into account any ocular fundus examinations that might have been performed while patients were hospitalized. Nonetheless, they are rarely performed for screening purposes in inpatients, and these missing data are marginal.
Conclusion
An automobile travel time longer than 35 min to visit an ophthalmologist appeared to affect the time intervals between ophthalmological follow-up of patients with diabetes. Teleophthalmology has made this travel time a modifiable variable. In addition to reducing travel time and healthcare costs associated with medical transport (ambulances), it also makes it possible to increase the number of DR screenings performed without an ophthalmologist present. The benefits of retinography at a distance should thus be examined in medical-economic cost-effectiveness studies; the extent to which it improves patients' quality of life should also be studied to demonstrate its interest to decision makers.
Availability of Data and Material
The data that support the findings of this study are available from L.C., but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of Dr Marie-Christine Banide (Head of the Department of Analysis and Treatment of Medical Information).
Footnotes
Acknowledgments
The authors thank Jo Ann Cahn for reviewing the article and advising on English translation. This study was conducted with funding from the Provence-Alpes-Côte d'Azur Regional Health Agency under the “Contrat Pluriannuel d'Objectifs et de Moyens 2012–2013” (a multiyear funding program for healthcare).
Author Contributions
C.M., H.C., and A.J. were major contributors in interpretation of data and in writing the article. P.V. was responsible for collecting and extracting data from the insurance fund; it has contributed its expertise to the construction of the Cox model. L.C. coordinated the project, carried out the statistical analyses, drafted the request for an ethical agreement, and was a major contributor in writing the article. All authors approved the final version and agreed to be accountable for the contents and integrity of this article.
Disclosure Statement
No competing financial interests exist.