
Abstract
Introduction:
The intent was to evaluate time to match initial investment of a new, statewide correctional system telehealth program based upon cumulative savings by avoidance of transportation and custody-related costs.
Materials and Methods:
The setting was a statewide correctional system where prisoners received medical care through enhanced telemedicine technology supported by newly recruited specialty providers delivered through an open architecture system. The patients were incarcerated persons requiring nonemergent consultations in 10 specialties. A financial model was created to estimate transportation expenses, including vehicular use and custody staff, during the out of prison travel for traditional face-to-face care. Cost savings were then estimated by multiplying transportation expenses by the number of telehealth encounters (avoided cost) and summed cumulatively. Savings were mapped monthly. Private sector specialists were recruited, provided security clearance, trained in the use of the technology, and provided a secure site to provide services.
Measurements and Main Results:
Based on the financial model, 1.2 million dollars in savings, equaling the initial capital investment, were achieved at 32 months. The total number of patient telemedicine encounters increased from 2,365 (±98/month) to 3,748 during the first 32 months of operation (July 2013 through January 2016: ±117/month) with 89% of the established specialties performed by telemedicine technologies.
Discussion:
It was initially estimated to require 48 months to achieve the investment savings, but savings were achieved in 32 months, demonstrating greater adoption than expected. While finances were quantifiable, enhanced public safety by avoidance of out of prison time is unquantifiable, but judged to be significant.
“It is but just, that the public be required to care for the prisoner, who cannot, by reason of the deprivation of his liberty, care for himself.”
—Spicer v. Williamson, Supreme Court of North Carolina, 1926
Background
By the end of 2014, ∼6,851,000 individuals were under supervision of the correctional system in the United States. This included 4,708,100 in community supervision (probation: 3,864,100, parole: 856,900) with an estimated 1,561,500 prisoners in state and federal correctional facilities. 1 When combining those in prison (sentenced) and jail (unsentenced), this number increases to 2.3 million. 2 In the state of Maryland, there are about 22,000 inmates in a male: female ratio of about 20:1. 1 These inmates are the focus of this study.
According to the Department of Justice, persons entering jail or prison present a multitude of chronic and acute medical and/or mental health conditions. As a measure of prevalence of illness or initial undertreatment, only about 25% of those entering prisons are on antipsychotics, whereas 69% exit on antipsychotics. 3 As many as 76% of inmates have substance abuse or drug dependence, 17% are homeless, and up to 27% have a history of physical or sexual abuse. From 12% to 30% of inmates will be injured by interpersonal violence after admission and those with mental illness are two to three times more likely to be injured. 4 The frequency of HIV, hepatitis B, and hepatitis C is particularly high in the pretrial and prison population. 5 Many are undiagnosed and/or untreated until medical evaluation and treatment are begun once imprisoned. About half of state and federal prisoners and local jail inmates reported having a chronic medical condition, including cancer, high blood pressure, stroke-related problems, diabetes, heart-related problems, kidney-related problems, arthritis, asthma, or cirrhosis of the liver. Twenty-one percent of prisoner's and 14% of jail inmates reported having an infectious disease, including tuberculosis, hepatitis B and C, or sexually transmitted diseases. Among those who reported having a chronic condition, about a quarter (27%) of prisoners and a tenth (8%) of jail inmates failed to inform prison personnel at admission.
Correctional Health functions as a public health agency by identifying disease, initiating therapy, and providing ongoing medical care before the inmate is released into society. As a result, there is significant impact upon community health due to initiation of therapy for infectious diseases. 6 Despite episodic reports of problematic healthcare, 7,8 prisoners have a constitutional right to healthcare under the eighth amendment of the U.S. Constitution (prohibition of cruel and unusual punishment). 9 Therefore, it is incumbent upon the penal system and society at large to provide full medical care.
The correctional healthcare arena suffers from increasing expenses and pressures to reduce costs. The PEW foundation reported that correctional system healthcare costs topped 8 billion dollars in 2011. 10 Costs are somewhat driven by the 1976 landmark Supreme Court Estelle versus Gamble decision affirming the constitutional right of prisoners to appropriate healthcare. 9 In addition, inmates are aging and living longer, requiring additional medical attention.
Correctional facilities encounter difficulty recruiting providers willing to work with the prison inmate population and/or enter the correctional environment. 11 In addition, correctional facilities are commonly located in remote areas or are functionally remote due to the complexity of a controlled, but potentially dangerous, environment. Another variable unique to correctional medicine is public safety and risk to correctional officers when transporting potentially dangerous prisoners outside the controlled prison environment 12 : “Every prisoner, regardless of custody level, should be considered an escape risk.”
Videoconferencing has long been utilized within correctional institutions to facilitate court appearances, parole hearings, family visits, and medical consultations. 13 In 2004, The Michigan Department of Corrections performed over 10,000 correction-related videoconferences. However, medical consultations through telecommunications technology have been hampered by lack of financial support (transitory governmental grants), 14 expensive dedicated transmission lines, 15 and complex and restrictive nature of telecommunication networks, all of which contribute to high cost and poor physician acceptance.
The Maryland Department of Public Safety and Correctional Services (DPSCS) houses over 22,000 inmates in 24 state facilities. The DPSCS includes pretrial (jail) and postsentencing (prison). Regarding the pretrial jail, the Baltimore City booking center is the sixth largest in the country and one of the most crowded; processing 45,000 to 60,000 persons each year, all potentially needing medical care. 16
In 2012, enhancement of the DPSCS Telehealth program became a top priority for the state. The primary thrust was to enhance quality and ease of real-time consultations between medical specialties (outside the walls) and primary medical teams behind the walls by bringing the specialist and the inmate face-to-face through telehealth technology while keeping all in their respective homes. While the concept of telehealth within the correctional systems is not new, the open architecture is unique.
Materials and Methods
In July 2012, the Maryland State DPSCS awarded a medical contract to Wexford Health Sources (Wexford Health Sources, Pittsburg, Pennsylvania). The contract included a state mandate to expand and enhance an existing telehealth program with the aim to reduce costs and improve access to specialty medical care, while reducing risk to correctional system employees and the public primarily by reduced transports.
Baseline line data were obtained during the 12-month period of July 2011 to end of June 2012 before initiation of the upgraded telemedicine program. During the baseline period, DPSCS incurred an expense of over $7 million dollars in combined vehicular costs and correctional officer costs during transport of prisoners for 8,684 visits to various outside-the-walls medical clinics and/or emergency departments.
Defining Physician Needs
To establish the priority of medical and surgical specialists needed, a retrospective review was done of all medical transports to outside medical facilities that occurred from June 1, 2012, to May 31, 2013. The analysis of these data identified the following most utilized specialties: • Emergency department triage • Ophthalmology • Cardiology • Urology • Gastroenterology • Endocrinology • Hematology/Oncology • Surgery • Orthopedics • Surgical/nonsurgical wound management • Infectious diseases (HIV and Hepatitis C)
Subsequent to defining physician needs, specialists from each field were recruited from the private sector with the agreement from Wexford Health to provide quick efficient reimbursement for services with minimal administrative burden for the physicians.
Defining Technology Needs and Procurement
After reviewing existing telemedicine equipment, a wish list of equipment and capabilities was established to include the following: • Secure Web-enabled telecommunications devices: open architecture • Electronic stethoscopes • General examination cameras • Digital ophthalmoscopes or retinal cameras • *Electrocardiogram (EKG) that integrate with the telecommunications devices • *Digital pulse oximetry • High-quality 24 × 7 information technology support
A request for proposal (RFP) was developed and sent to four of the largest vendors with subsequent vendor interviews and demonstrations. Ultimate selection was InTouch Health technology (InTouch Health, Santa Barbara, CA). Purchased equipment included InTouch Health RP-Lite® units with installed electronic stethoscope (Telehealth Technology, Boston, MA) and general examination camera (Global Med, Scottsdale, AZ). The goal of integrated EKG and pulse oximetry was not met. In lieu of ophthalmoscopes, the funding was used to purchase two high-level retinal cameras that were deployed to strategic sites. RP-Lite units were placed at 19 correctional institutional originating sites (where the patients are located) (Figure 1).
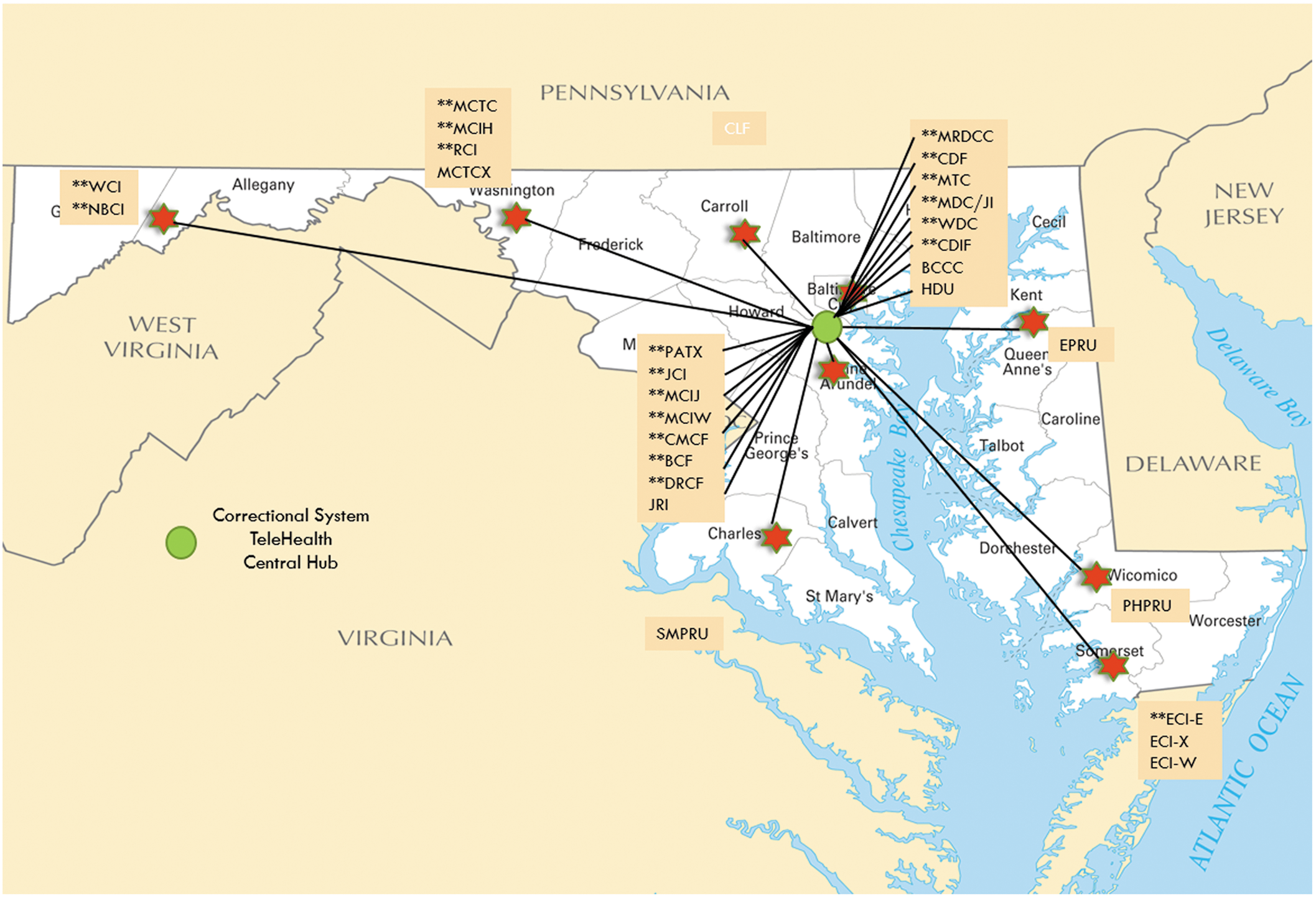
Maryland correctional institutions: Abbreviations are defined in Supplementary Table S1 (Supplementary Data are available online at
A distant site (where the remote providers are located) was established at a hospital facility within Baltimore City, which already housed a secured locked ward. A secured locked ward is a security-guarded, locked, and monitored unit that houses offenders within a hospital. The distant site was equipped with control stations with embedded software and stethoscope headset with earphones.
Physician Staffing
Specialists were enlisted to provide consultative services from the distant sites. Specialists were able to provide care either by telehealth technology or on-site at the Baltimore secured locked ward. The specialists were educated on the unique elements of working through the correctional system and trained on the use of specific telecommunication devices. Each consultant became an independent contractor with Wexford Health. Credentialing was completed by Wexford Health following Maryland state guidelines, industry standard policy, procedure, and performing all first sourcing. There was a single credentialing process and single credential required for all correctional facilities within the state.
Reimbursement, Documentation, and User Access for Telehealth Process
Physicians submitted a claim directly to Wexford Health on a fee-for-service basis. Remote providers had Maryland DPSCS-approved access to the prison Electronic Patient Health Record to obtain and review clinical information and to document. Telehealth equipment was distributed to the remote providers and assigned a unique user access ID after successful training.
Process of Care
Each prison has a primary site or infirmary, established to provide telehealth services within a secured Health Services Unit with an RP-Lite unit. The locked and secure environment includes clinics where face-to-face examinations are conducted.
Behind the Walls
Each prison medical unit has a primary care physician on-site. When the primary care provider determines that a nonemergent consultation is required, a request is submitted to the Wexford Medical Director of Utilization Management for approval (gatekeeper). If approved, an authorization number is provided for scheduling, tracking, and reimbursement. Inmates must provide consent for any telehealth appointment. Appointments are scheduled with appropriate specialists. Centralized scheduling for each specialist was developed to improve efficiencies and maximize the number of patients scheduled for each clinic. Block clinic time was established for remote physicians located at the Baltimore city site to see both on-site and telehealth appointments. Initial consultations were generally performed with the correctional primary care provider and the inmate-patient at the prison (originating site) and the remote community provider at the distant site. Subsequently, when procedures are indicated, the inmate-patient is transported to the outside Baltimore City Medical facility, and once the procedure is completed, the inmate-patient is transported back to their prison facility. A subsequent specialty follow-up appointment is scheduled generally through a telehealth virtual visit.
Process of Inmate Transport
Two armed custody officers are always required when an inmate-patient is transported off-site. The vehicle is a commercially available van that contains a partition between the driver and inmate, windows with mesh metal grills, and a strong padlock system on the outside of the rear doors. The vehicle is not upgraded to be bulletproof or have uniquely puncture-resistant tires. During some long-distance transports, the inmate-patient may require a layover at an interim prison facility in closer proximity to the medical facility, thereby adding to the transport time, costs, and increasing the logistical complexity.
Cost-Saving Estimates
Cost-saving estimates were based completely upon avoidance of inmate-patient transport (Table 1). With directives from the Maryland Office of Inmate Health Services, the following cost model was provided:
Estimated Cost Per Inmate-Patient Trip to a Medical Facility
Vehicular cost is based upon DPSCS transportation department data.
DPSCS, Department of Public Safety and Correctional Services.
The cost savings can be described by a simple equation:
The savings were summed each month and added to the prior month's cumulative savings and the data presented graphically. The intent of the evaluation was to determine how many months were required to pay back the initial investment of $1,200,000.
Results
It took about 32 months to reach the break-even cost of $1.2 million dollars cumulative cost savings during which 3,356 telemedicine specialists' consultations were performed and therefore 3,356 transportations were avoided (Table 2).
Breakdown of Medical Visits During the Initial 32 Months of Telemedicine
Graphically (Figure 2), the return on initial capital investment is shown below which demonstrates a relatively linear graph, but with a gradually more positive slope over time, suggesting progressive greater acceptance, adoption, and utilization.

Cumulative cost savings by avoidance of transport of correctional system inmates to medical facilities when care is provided remotely through telemedicine. Blue line: actual cost avoidance. Green line: calculated cost avoidance including on-going expenses (equations 3, 4 or 5).
Assuming a continuously linear utilization, the above curve can be approximated by
where A1 is the slope of the curve and X is the time duration in months. Using total savings of $1,200,000 over 32 months yields a slope of 37.5K, suggesting average monthly travel/transport savings of $37,500 per month.
Ongoing Operational Costs
Half-time positions for this program included the Telehealth Director and the Information Technology Administrator. However, both these positions existed before installation of the new technology and are not included in the analysis. New operational costs are outlined in the Table 3 below.
Telemedicine Operational Costs
When incorporating the new ongoing operational expenses, the cumulative “cost avoidance” equation can be represented by:
where A2 = monthly expenses. When providing empirically derived numbers for A1 and A2, the equation evolves to the following:
Simplifying equation (3) with the addition of empirically derived data becomes
Then, solving the equation for number of months to save $1,200,000 when accounting for ongoing new operational expenses reveals that 66 months would be required to recapture the capital investment.
Discussion
According to the 1976 Supreme Court decision (Estelle vs. Gamble), “Deliberate indifference by prison personnel to a prisoner's illness or injury constitutes cruel and unusual punishment contravening the 8th and 14th amendment mandating due process.” As a consequence, prisoners are a unique population of U.S. citizens with mandated healthcare. Additionally, the correctional system patients are unique in being a controlled population of patients.
The three priorities from the state of Maryland were public safety, decrease medical transportation costs, and achieve return on the initial capital investment. The graph in Figure 2 demonstrated achievement of return on investment (ROI) within 32 months, satisfying the cost imperative. In describing the accumulated savings mathematically, we assumed a linear relationship. However, review of the graph suggests that there may be an increasing slope, which would then lead to greater monthly savings. Ongoing costs (connectivity fee, tech support, user access fee, and yearly software upgrades) were factored in equations (3), (4), and (5). The slope of equation (5) represents the monthly savings in directly measured dollars and could be a tool for others to estimate savings when establishing similar telehealth programs.
It is likely that the cost savings are underestimated. The cost estimates assume an average and do not include extreme outliers. For example, the transport of prisoners with a high risk of escape, such as gang members, requires an additional follow vehicle with two additional officers, thereby doubling the cost of transport. Layovers before and after outside medical facility appointments for long-distance prisoners are another unknown cost that is not added to the calculations. Finally, we were provided the state of Maryland vehicular costs, thereby limiting ability to adjust for greater traveling distances, variations in the cost of fuel, or vehicular depreciation.
Purchase Versus Lease Equipment
Regarding hardware, the state of Maryland made the decision to purchase the telehealth hardware outright, as opposed to a leasing agreement. Had the state chosen a lease option, the discussion of ROI Investment would have only been modestly different. The operational fees would have been largely eliminated as such fees are generally included in the leasing fee. On the other hand, with outright purchase, the state incurs issues of depreciation and eventual replacement costs.
Telehealth and Public Safety
We were unable to quantify a dollar value to public safety regarding injury and loss of property or life. A study from the New York State Police Department revealed that overall 40% of prisoner escapes occurred during transport with 68% escaping despite being in a caged vehicle with an associated 12% injury rate to security guards. 17 The case of inmate William Morva being transported for evaluation of a minor sprain on August 21, 2006, is illustrative. He was able to overpower the correctional officer, taking the correctional officer's sidearm, killing a hospital security guard, and later killing a local county sheriff before being recaptured. 18 The case of Woosen Assaye, an inmate who was being transported from the Alexandria Virginia County Jail to Innova Fairfax Hospital, where he slipped out of his manacles leading to a complete hospital lockdown before recapture. 19 These cases demonstrate an enormous social impact of escapes during medical transports, mandating very serious efforts to avoid out of prison transports. In both cases, the escapes would have been avoided by the use of telehealth.
The open architecture telehealth program allows the contracted Managed Healthcare organization, Wexford Health, two significant advantages. First, remote physicians can work from almost any site. Thus, the potential recruitment pool of remote physicians, while still requiring Maryland state licensure, would have no geographic restrictions and could expand to other states. Competitive characteristics of the free market can come to bear in the recruitment of remote providers. Remote providers utilizing telehealth would then experience fewer barriers to working with the correctional system, as opposed to working in the correctional system. The second advantage of an open architecture system is the flexibility to allow the managed care organization to establish a single remote specialty medical site and network to all the Maryland correctional facilities, thereby reducing overhead, staffing, and technical costs.
Finally, regarding the presented data, the achievement of 89% participation in telehealth was highly successful within the specific specialties chosen. This analysis was restricted to those patients being seen within such chosen specialties and for the established cadre of specialists. Those patients requiring consultations with specialties such as neurology, nephrology, or ortho-spine were not included in the analysis because those remote specialties had not yet been recruited.
The overall impact of a telehealth program is exemplified by a typical cardiac patient. The first consultation regarding a cardiac symptom could be done remotely without transport. If determined that a cardiac catheterization is required, then the patient would be transported to a medical facility, undergo catheterization, and be quickly transported back to prison. The subsequent visits could generally be done remotely. Therefore, instead of a minimum of three trips to complete a cardiac evaluation, there could be as few as one transport.
In summary, this process and the documented outcomes illustrate meeting the priorities of the state of Maryland: increase public safety, decrease transport costs, and demonstrate to the Maryland state legislators that the return of the initial capital investment could be realized in an acceptable period of time. This process and the documented outcomes could also be helpful with either establishing or expanding telehealth programs within the greater correctional healthcare space nationally or internationally. Ultimately, savings to public safety greatly trumps the more easily calculated financial savings.
Footnotes
Disclosure Statement
H.N.R. previously served as consultant and speaker for InTouch Health®. E.S.R. and T.L. are full-time employees of Wexford Health, a nationwide, for-profit Managed Health Care Organization for Correctional Systems. S.B. is a full-time employee of the State of Maryland Department of Public Safety and Correctional Services.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.