
Abstract
Objective:
To evaluate the cost-effectiveness of a pilot telehealth program applied to a wide population of patients with chronic obstructive pulmonary disease (COPD).
Design:
Vital signs data were transmitted from the home of the patient on a daily basis using a patient monitoring system for review by community nurse to assist decisions on management.
Setting:
Community services for patients diagnosed with COPD.
Participants:
Two Primary Care Trusts (PCTs) enrolled 321 patients diagnosed with COPD into the telehealth program. Two hundred twenty-seven (n = 227) patients having a complete baseline record of at least 88 days of continuous remote monitoring and meeting all inclusion criteria were included in the statistical analysis.
Intervention:
Remote monitoring.
Methods:
Resource and cost data associated with patient events (inpatient hospitalization, accident and emergency [A&E], and home visits) 12 months before, immediately before and during monitoring, equipment, start-up, and administration were collected and compared to determine cost-effectiveness of the program.
Main Outcome Measures:
Cost-effectiveness of program, impact on resource usage, and patterns of change in resource usage.
Results:
Cost-effectiveness was determined for the two PCTs and the two periods before monitoring to provide four separate estimates. Cost-effectiveness had high variance both between the PCTs and between the comparison periods ranging from a saving of £140,800 ($176,000) to an increase of £9,600 ($12,000). The average saving was £1,023 ($1,280) per patient per year. The largest impact was on length of stay with a fall in the average length of inpatient care in PCT1 from 11.5 days in the period 12 months before monitoring to 6.5 days during monitoring, and similarly in PCT2 from 7.5 to 5.2 days.
Conclusion:
There was a wide discrepancy in the results from the two PCTs. This places doubt on outcomes and may indicate also why the literature on cost-effectiveness remains inconclusive. The wide variance on savings and the uncertainty of monitoring cost do not allow a definitive conclusion on the cost-effectiveness as an outcome of this study. It might well be that the average saving was £1,023 ($1,280) per patient per year, but the variance is too great to allow this to be statistically significant. Each locality-based clinical service provides a service to achieve the same clinical goal, but it does so in significantly different ways. The introduction of remote monitoring has a profound effect on team learning and clinical practice and thus distorts the cost-effectiveness evaluation of the use of the technology. Cost-effectiveness studies will continue to struggle to provide a definitive answer because outcome measurements are too dependent on factors other than the technology.
Introduction
Amajority (70%) of the total health and social care budget is spent on treatment and care of patients with long-term conditions (LTC). 1 Telehealth services are suggested as a solution to control the spiraling cost and improve clinical outcomes. This involves installing equipment in patient's homes to measure daily physiological parameters. These are assessed by clinicians (a nurse, a doctor, or a medically trained technician) to determine the potential for deterioration in health status and assess their well-being.
Measurements for health monitoring can include blood glucose, blood pressure, weight, saturated blood oxygen (SpO2), and electrocardiogram (ECG). Social care monitoring can include activity monitoring, bed and chair usage, fall alarms, and use of utilities. Telehealth equipment can be configured in many ways, and the level and complexity of monitoring technology can vary from a simple phone call to report data through to the use of videoconferencing. 2
The term telehealth is used interchangeably in this document with telemonitoring and remote monitoring. We will refer exclusively to telehealth. Many advantages of telehealth are reported in the literature: improved clinical outcomes, reduced number of unplanned hospital and accident and emergency (A&E) admissions, 3 efficient handling of caseloads, and facilitation of self-management of condition by patients. A meta-analysis confirms these findings. 2,3
Exploiting technology to good effect proves complex because service redesign and clinical engagement are found to be both expensive and challenging. High-quality studies on cost are few and inconclusive. In a review of studies on cost-effectiveness of telehealth, Mistry reports that many studies lacked adequate methodological rigor and details of design. 4 Mistry argues that this lowered the overall quality and further that most studies were pilot in nature and presented findings on small sample size (100 patients or less). 4 Polisena et al. also concluded that although telehealth might hold the potential to reduce cost, the quality of studies assessing and reporting telehealth cost was poor. 5 Whitten et al. in a review of cost-effectiveness of telemedicine intervention similarly conclude that there was a lack of evidence demonstrating cost-effectiveness. 6 A recent review on telehealth continues to report that the evidence for cost-effectiveness of telehealth is “weak and contradictory.” 7
The primary concern is that outcomes are based on small pilot studies that run over short periods of time (typically 3–6 months), 7 and with little consideration of the impact of services introduced by the pilot. Outcomes are expected to be different when at scale over a prolonged period and integrated into normal healthcare services. To establish whether this is true, the Whole System Demonstrator project in the United Kingdom undertook a randomized trial with 6,000 patients. The conclusion is that a telehealth service in combination with standard care is not cost effective when compared with standard usual care. However, only savings are published without any comparison with the costs of the telehealth services. The authors recommend that future research on cost-effectiveness of telehealth should be “targeted towards specific patient population and sub population” and should explore the “association between area level factors, patient characteristics (demographics, needs levels for each index condition), and the variation in their service use and cost.” 8
Further studies 9 also conclude that additional home telemonitoring care is not cost effective compared to usual care. This study 9 also reports variation in cost for the groups; there was significant difference in costs before and during the project; and many patients had no admission to hospital during the period of the study.
In contrast, this article reports on the cost-effectiveness of a telehealth program when applied to a wide population of patients with chronic obstructive pulmonary disease (COPD). It takes into account the characteristics and structure of service delivery.
Methods
Program Description
National Health Service Direct (NHSD) launched a pilot telehealth program for patients with COPD in two Primary Care Trusts (PCTs; November 2010 in PCT1 and March 2011 in PCT2) to evaluate cost-effectiveness of a service. The remote monitoring was managed centrally through NHSD.
PCTs were the administrative bodies in England responsible for commissioning primary, community, and secondary health services from providers. Until May 31, 2011, they also provided community health services directly. Collectively PCTs were responsible for spending around 80% of the total National Health Service (NHS) budget. PCTs were abolished on March 31, 2013, as part of the Health and Social Care Act 2012, with their work taken over by Clinical Commissioning Groups.
The NHSD telehealth program included the following: (1) planning and administration of the program, developing operating policy and procedures and technical requirements, (2) device commissioning and management of the installation process, (3) developing clinical process workflow for the call center, and (4) reporting and management of data elements for evaluation. The PCTs were responsible for (1) the operational and service elements of the program at their respective sites and (2) participation in planning and reporting of results for program evaluation.
Evaluation for the NHSD telehealth program was designed by the joint research team of Brunel University and Chorleywood Health Centre, with input from NHSD and the PCTs. The evaluation was designed so that the majority of data from the patient were gathered through the Health Buddy to simplify implementation (no paper), reduce impact on PCT staff workload, and make the project as close to normal service as possible. The PCTs were selected on the basis of having well-established community teams to manage patients with COPD. In this way we would be able to determine the impact of introducing the technology and not the introduction of service. Ethical approval was gained from NHS Research Ethics Committee.
The BOSCH® Health Buddy remote monitoring system was used for the program. Peripheral devices included temperature, weight, oxygen level, and blood pressure. It also provided structured questionnaires on symptoms for respiratory distress, cough and sputum, their severity, and user acceptability for both patient and nurse professionals. Health education messages were transmitted to the patient.
Population Identification
The evaluation was commissioned by NHSD to determine cost-effectiveness and other outcomes of a telehealth program. Two PCTs participated and a total of 321 patients were enrolled into the monitoring program. Of these, 227 were included for statistical analysis using the criteria of having a complete baseline record of at least 88 days of continuous remote monitoring.
The decision to refer a patient to the telemonitoring service was made by the PCT, and was based on the inclusion criteria as in the Inclusion Criteria for Receiving the Monitoring section.
Inclusion criteria for receiving the monitoring
Patients having a primary diagnosis of COPD and at least one of the following: • Two or more admissions or emergency attendances in the 12 months. • Difficulty following a medication regimen. • Difficulty following a treatment regimen.
Patients had to satisfy the following criteria: • Have a telephone. • Reasonable cognitive ability that enables them to report observations. • Be able to understand English (to use the Health Buddy). • Reasonable dexterity (to use the Health Buddy and peripherals). • Not have a severe visual impairment.
Inclusion in the statistical data set
• Completion of all baseline measures.
• Three months (88 days) of continuous remote monitoring.
Patient Management
Each PCT was responsible for referring a patient to the telemonitoring service and how the patient was managed within the service. Each patient was provided with the Health Buddy unit and a finger pulse oximeter and instructed to take one SpO2 measurement each day. In the same measurement session, the Health Buddy would ask questions relating to the symptoms of COPD, such as the type of cough and sputum production. Devices to monitor other vital signs were provided according to the needs of the patient. Data were reviewed daily by the nurse and were used to assist decisions on the management of the patient.
Resource and Cost Utilization
Resource utilization data were obtained from multiple sources and include A&E visits, ambulance usage, and hospitalization. Cost reports were submitted by NHSD, PCT1 and PCT2.
For comparative purposes, each patient acted as his or her own control. To avoid the effects of seasonal variation and expected deterioration in health, two control periods were compared. For each patient we selected an equal period of monitoring taken to start 12 months before monitoring and so cover the same time of the year (seasonal) and an equal period taken to end immediately before the start of the remote monitoring (deterioration). The levels of service usage for each patient were found for both these periods and the monitoring period.
For the comprehensive cost analysis, pertinent information was defined as useful by the project partners. Two templates were made for the project; the first recorded data about patient usage of health services other than home monitoring and the second recorded data about the telemonitoring service. These were completed by the PCTs. Analysis of resource usage was separated into two recognizable groups defined by clinical event outcomes, all-cause and COPD-specific clinical events. This was based on coding whenever possible. Identifying trends and changes attributable to remote monitoring was to be aided by comparing the service user data of high-cost users (as defined by a priori admission to hospital) before and during monitoring. Two data collections were made, one midway through the project to verify methods and data quality and at the end for final analysis. Resource utilization and costs included those to establish the program (training, planning meetings) and for ongoing running (administration).
Health resource utilization
Analysis of health resource utilization was performed by using each patient as his or her own control and comparing metrics before and during monitoring. To compensate for seasonal effects and because COPD is a degenerative disease, data were taken for an epoch of equal duration 12 months before the monitoring period and immediately before monitoring.
Healthcare system cost
The telehealth program targeted a population of patients with known high cost and likelihood of future high cost. The eligibility criteria were designed to select those having high resource utilization and consequent cost. The purpose of the investigation was to compare the savings in resource with the cost of the program.
Cost data included the initial cost for start-up (attending planning meetings, staff training), ongoing management of the program, and increased personnel time to examine data and visit patients. We assumed a monthly service charge of £100 ($125) per patient was made by NHSD to provide the equipment, manage the data, and provide the service. The cost also included installation and decommissioning.
Healthcare system cost-effectiveness
For this study, we chose to define cost-effectiveness as a comparison between the costs to provide the remote monitoring service and the direct savings in health cost that could be attributed to the introduction of the service. Service costs included equipment, remote monitor service costs, and additional staff resources; direct savings were attributed to reduction in utilization of health service resource, including hospitalization avoided, reduced in-hospital stay, and reduced contacts with health services.
Our data did not include quality of life, and so we were unable to undertake cost/benefit analysis.
Results
Baseline Data
Based on the inclusion criteria, 107 patients from PCT1 and 120 patients from PCT2 were included in the statistical data set. The average length of monitoring in PCT1 was 203 days and in PCT2 was 215 days, giving a total of 21,738 and 25,764 monitoring days for each PCT, respectively. The mean age of patients on entry to monitoring was 70.9 ± 8.9 with 112 male and 112 female participants, and was the same for each PCT. Data on gender were not provided for three patients.
Health service utilization data used in this study were provided by the PCTs. Resource usage for hospitalization and A&E visits was separated by cause of admission (COPD, all other causes).
The study was designed to evaluate service, rather than a controlled trial, and patients were enrolled and withdrawn based on clinical judgment. This resulted in wide variation length of participation. We chose the minimum period for inclusion in the data set to be of sufficient duration that we might capture clinical events and was comparable to the period of monitoring in other home monitoring services, such as used for hospital discharge. This period is typically 90 days, but inspection of the data showed that a choice of 88 days of continuous remote monitoring would include several further patients.
Initial and Start-Up Costs
Each PCT provided detailed costs associated with establishing the program. This included a breakdown of the impact on all staff involved, together with all aspects such as training, attending meetings, planning meetings, additional administration, and travel. These costs are reported in Table 1.
Resource Utilization and Cost
H, hours; PCT, Primary Care Trust.
There were differences in approaches and costs between the PCTs. PCT1 allocated all COPD patients to a member of its LTC team, whereas PCT2 allocated the less severe patients to its community matrons and the more severe patients to the respiratory team. PCT1 also allocated significantly greater time to training than PCT2. It also appears that they appointed dedicated administration support. As a consequence, PCT1 reported significantly higher start-up costs.
Comparison of Outcomes
We determined that inpatient stays were the single dominant cost for health resource utilization. Changes seen in A&E and outpatient usage were small and thus savings were small in comparison. Cost analysis was only performed for inpatient stays.
Health Resource Utilization—Inpatient Stays
Total resource utilization data (Table 2) indicate a decrease in total inpatient bed days during the monitoring period when compared with both the period 12 months before (34%) and immediately before monitoring (31%). This results in savings of £131,200 ($164,000) and £117,120 ($146,700), respectively. There is a difference in the cause of the savings made. The savings made during monitoring when compared with data from 12 months before are due largely to reduced average length of stay (−40%) despite a comparative increase in the number of stays (11%). Comparison of hospital usage data during monitoring and immediately before monitoring shows a reduction in the number of admissions (−29%) with a negligible reduction in length of stay (−3%).
Overall Health Resource Utilization
A&E, accident and emergency; COPD, chronic obstructive pulmonary disease.
The PCT1 data (Table 3) show a significant decrease in total inpatient bed days in the monitoring period when compared with both the period 12 months before (62%) and immediately before monitoring (47%). This resulted in savings of £140,800 ($176,000) and £78,080 ($97,800), respectively. The savings made during monitoring when compared with data from 12 months before are due largely to reduced average length of stay (−43%) along with a reduction in the number of stays (−32%). Comparison of hospital usage data during monitoring and immediately before monitoring shows a reduction in the number of admissions (−45%) and a very small reduction in the length of stay (−4%). The data for “all other” clinical causes for admissions showed a reduction. We also observed reductions for inpatient bed days of 22% and 60%, respectively.
Health Resource Utilization Primary Care Trust 1
The PCT2 data (Table 4) show that during the monitoring period there was an increase in the number of inpatient bed days when compared with the period 12 months before monitoring (6%) but a decrease for the period immediately before monitoring (−19%). This resulted in an increase in cost of £9,600 ($12,000) and savings of £39,040 ($48,900), respectively. The increased spending seen when the monitoring period data are compared with the period 12 months before monitoring may be explained by the 50% relative increase in the number of admissions although its impact was perhaps eased by a reduction in length of stay (31%). For “all other causes,” there was a reduction in patient bed days during the monitoring period when compared to the period 12 months before (9%) but an increase (10%) when compared to the period immediately before monitoring.
Health Resource Utilization Primary Care Trust 2
Other Outcomes
The cause of A&E visits in PCT2 could not be found in the data and it was not possible to count visits caused by either COPD or “all other causes.” The number of visits due to COPD in the PCT1 data was too small to provide statistically significant changes. Outpatient appointments had a consistent reduction of about 15% for PCT1 but the change was inconsistent for PCT2. Numbers were too small to have significant impact on the cost when compared to inpatient stays.
Costs of the Service
Each of the PCTs was asked to provide details of direct costs that could be attributed to setting up and running the service. This included staff time spent on planning meetings, travel to planning meetings, administration, and education sessions. PCT1 estimated costs to be £47,000 ($58,900) and PCT2 estimated costs as £28,000 ($35,000). A separate estimate of ongoing costs of providing the service (administration) is shown in Table 1.
NHSD assumed a cost of £100 ($125) per patient per month to provide the service (or £3.29 [$4.12] per day). PCT1 ran the service for 16.9 months for 107 patients and accrued a cost of £180,000 ($225,600) to provide the monitoring service for the duration of the project. PCT2 ran the service for 17.9 months for 120 patients and accrued a cost of £215,000 ($269,400) to provide the monitoring service for the duration of the project.
Discussion
Overall Outcomes
The project aim was to determine the cost-effectiveness of using a telehealth service delivery model to manage patients with severe COPD. Our project includes two separate pilot sites and by taking the prior monitoring period from two separate periods into account, we have created four independent data sets for comparison.
The most striking observation is the significant difference in outcome from the data sets, with high variance both between the PCTs and between the comparison periods. This result would support the observation of poor correlation that is reported in meta-analysis of cost-effectiveness studies. Within our data, we see outcome ranging from a saving of £140,800 ($176,500) to an increase of £9,600 ($12,000). The cause of this variation may be related to the process utilized within the PCT and additional research on the impact of other variables that influence patient outcomes is needed.
Cost-Effectiveness
PCT1 made a saving of £140,800 ($176,500) at a cost of £180,000 ($225,600). PCT2 made a saving of £39,040 ($48,900) at a cost of £215,000 ($269,500). The saving for each patient for a year in PCT1 was £2,366 ($2,965; 12 months before) and £1,312 ($1,645; immediately before). In PCT2, a loss occurred of £136 ($170; 12 months before) and a saving of £552 ($690; immediately before).
There are a number of factors that would affect cost-effectiveness. No allowance was made for the reuse of equipment and the actual number of monitoring devices used was not reported. For example, if equipment could be hired for only each day, it was used for monitoring the monitoring cost; for PCT1 would then have been £71,518 ($89,600) rather than £180,000 ($225,600) and for PCT2 £84,760 ($106,200) rather than £215,000 ($269,400).
The reported costs to establish and run the monitoring service were additional to the usual cost of providing a COPD service in the community and were particular to the project. The actual cost of providing a telehealth program that was integrated fully into the usual service provision would be less than that reported. One hundred fifty of the patients, approximately, were never admitted to hospital and therefore would not have resulted in savings and would skew the findings of costs and savings. Overall implementation and administrative strategies as well as deployment factors may have influenced the cost differences noted between the two PCTs.
Impact on Hospital Admissions
Despite the possibility that the admission policies of each acute trust had changed over the 12 months before monitoring, the telehealth program appeared to have an effect on the number of admissions and the clinical outcomes. It can be argued that the latter is shown by the finding of a fall in the average length of inpatient care: in PCT1 from 11.5 days in the period 12 months before monitoring to 6.5 days during monitoring, and similarly in PCT2 from 7.5 to 5.2 days. There is no evidence to explain these changes. It had not been possible to conduct a study of the patient care pathways that might have shown the impact of home monitoring on either patient or professional carer education or an earlier recognition of exacerbations leading to more prompt hospital admission. If the latter was the case, it can be assumed that inpatient management would be more effective allowing earlier hospital discharge. In addition, the professional skills and clinical effectiveness of the community team may have developed over the year before monitoring and that there was more effective patient management irrespective of monitoring.
To understand how the length of stay was being affected by the monitoring, we considered the profile of the length of stay for each of the periods of interest; 12 months before, immediately before, and during monitoring. Figure 1 shows that many of the short stays of 3–5 days were reduced to 2 days, and the number of stays of 12–15 days was reduced. We assume that prompt admission may result in a much reduced stay and having the technology in the home gave confidence for early discharge. Figure 1 also shows that many patients were not admitted to hospital during the periods of interest (0 days).
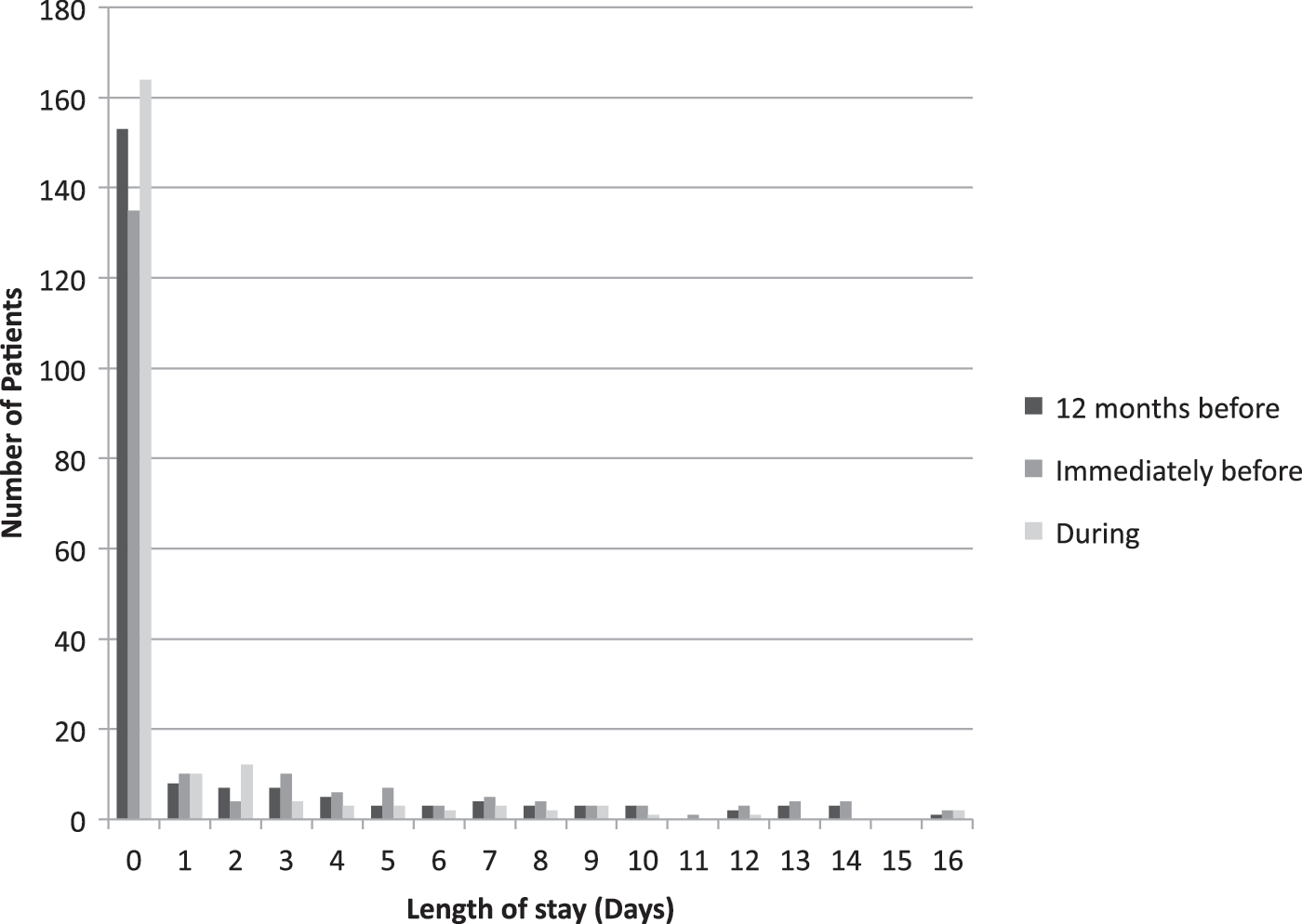
Length of hospital stay for the periods 12 months prior, immediately prior, and during monitoring.
Figure 2 depicts the change in the total length of stay for each patient and shows the difference between the total length of stays immediately before monitoring and the total length of stays during monitoring. The difference for each patient is shown as a histogram of the change (note that the change for 0 days is suppressed). The greatest peak occurs for a decrease of 2 days and many of the lengthy stays (normally arising from complications) are eliminated. We may also propose that by having monitoring available, patients are being released early.

Change in length of stay for each patient compared to length of stay in the period immediately before monitoring.
Limitations of This Study
The study has a number of recognizable limitations that must affect the results of the study. Although the average length of monitoring was 200 days, there was a wide variation in monitoring times with a minimum monitoring period of 88 days. This will have impacted on capturing health resource usage. Illness will wax and wane and resolves when disease is cured or causes death. COPD is a chronic LTC that is progressive and is affected by seasonal change and the well-being of patients can be changed markedly by other comorbidities and social factors. The study design attempts to compensate for this by comparing data from the monitoring period with both the period 12 months before and the period immediately before monitoring. There was anecdotal evidence from the research team of professional learning and team development in both PCTs. As the project progressed, it is believed that the nurses developed better management of their patients. This alone may have had an impact on their recognition and treatment of a sudden deterioration in a patient's condition and the need for admission and leading to greater clinical effectiveness. For example, PCT1 showed a saving of £60,000 ($75,000) without any monitoring. In this study, the telemedicine service was added as an “additional” layer of service making it difficult to discern which element of the combined service had the greatest impact. Others have reported large gains in terms of cost savings and improved clinical outcomes with telemedicine in less well-developed community health services.
Analysis of health resource was restricted to the data from the patient administration system (PAS). A fuller analysis with data from the patient's clinical record could have revealed greater detail about the causes of admission, reasons for extended stay, and clinical outcome.
The project was to have evaluated cost/benefit by applying SF-12v2 to all patients at baseline and at period intervals. However, a system error resulted in the questionnaire being given to only 14 patients. Analysis of this small set of data showed no significant change in health.
We made no attempt to evaluate the project from a user perspective, and so we were unable to determine how patient management strategy had changed as a result of monitoring being introduced.
Implications Derived From This Study
The study provides a number insights and lessons to be learned. Future evaluations of cost-effectiveness, and clinical effectiveness for that matter, of remote patient monitoring have to be different because such evaluations seen in this study and in others are highly variable, and thus unreliable. Despite the fact that each locality-based clinical service provides a service to achieve the same clinical goal, they do so in significantly different ways, with varying levels of investment and skill. The introduction of remote monitoring itself has a profound effect on team learning and clinical practice and thus distorts the cost-effectiveness evaluation of the use of the technology.
There was a wide discrepancy in the results from the two PCTs. This places doubt on outcomes and may indicate also why the literature on cost-effectiveness remains inconclusive. Others 9 have similarly reported that statistical parameters for the respective cohorts are not stationary.
Moreover, to gain a true assessment of the cost-effectiveness of remote patient monitoring, the effect of the service must be considered in how the experiment is established, and how outcomes are interpreted, in order that the effect of the technology alone is assessed.
The analysis of length of stay shows a marked decrease that could be attributed to the early discharge of patients to a home where monitoring is available. This suggests a need for systems to be deployed rapidly with the patient on discharge.
The wide variation in savings and the uncertainty of monitoring cost do not allow a definitive conclusion on the cost-effectiveness as an outcome of this study. It might well be that the average saving was £1,023 ($1,280) per patient per year, but the variation is too great to allow this to be statistically significant.
The authors conclude that cost-effectiveness studies will continue to struggle to provide a definitive answer because outcome measurements are too dependent on factors other than the technology. This question could be answered by developing standardized measures of clinical and organizational activity that can be considered in addition to basic costs and thereby minimize the effect of cultural, educational, and financial differences between healthcare services on the outcomes of studies.
Footnotes
Acknowledgment
This research was part funded by NHSD.
Disclosure Statement
No competing financial interests exist.