
Abstract
Background:
Healthcare systems are interested in technology-enhanced interventions to improve patient access and outcomes. However, there is uncertainty about feasibility and acceptability for groups who may benefit but are at risk for disparities in technology use. Thus, we sought to describe characteristics of Internet use and technology-related attitudes for two such groups: (1) Veterans with multi-morbidity and high acute care utilization and (2) informal caregivers of Veterans with substantial care needs at home.
Materials and Methods:
We used survey data from two ongoing trials, for 423 Veteran and 169 caregiver participants, respectively. Questions examined Internet use in the past year, willingness to communicate via videoconferencing, and comfort with new technology devices.
Results:
Most participants used Internet in the past year (81% of Veterans, 82% of caregivers); the majority of users (83% of Veterans, 92% of caregivers) accessed Internet at least a few times a week, and used a private laptop or computer (81% of Veterans, 89% of caregivers). Most were willing to use videoconferencing via private devices (77–83%). A majority of participants were comfortable attempting to use new devices with in-person assistance (80% of Veterans, 85% of caregivers), whereas lower proportions were comfortable “on your own” (58–59% for Veterans and caregivers). Internet use was associated with comfort with new technology devices (odds ratio 2.76, 95% confidence interval 1.70–4.53).
Conclusions:
Findings suggest that technology-enhanced healthcare interventions are feasible and acceptable for Veterans with multi-morbidity and high healthcare utilization, and informal caregivers of Veterans. In-person assistance may be important for those with no recent Internet use.
Introduction
Internet technology has the potential to improve access to care and health information for patients. Technology-enhanced interventions may reduce the impact of barriers on healthcare access (e.g., distance to medical facilities) and there is some evidence that such interventions can improve clinical outcomes. 1 National mandates to implement Internet technology for healthcare have included Centers for Medicare and Medicaid Services requirements for patient access to their electronic health records and messaging portals, leading to increased incorporation of technology in healthcare. 2 Veterans Health Administration (VHA) has similarly invested in technology to enable patient access to their health records, pharmacy requests, and communication with healthcare teams via the Internet. 3
However, despite the important potential benefits of such technology in healthcare, there are persistent concerns about the “digital divide”—disparities in technology use and access, particularly affecting those with lower socioeconomic status and older adults. 4 –6 In a 2014 survey of U.S. adults, 97% of those with college or higher education reported using the Internet, compared with 76% of those with high school education or less. 4 Among Medicare beneficiaries aged 65 and older, both higher income and more education were associated with increased use of Internet for health-related reasons. 6 Older adults have also reported lower readiness to use Internet sites, e-mail, and videoconferencing for healthcare purposes, compared with younger counterparts. 7 If not adequately accounted for and addressed, disparities in access and comfort with technology could limit implementation of technology-enhanced interventions, especially for older adults and those with lower socioeconomic status.
Previous studies of Veterans have largely focused on exposure and Internet access, 8 –10 and few have addressed Veterans' attitudes toward incorporation of technology in healthcare. Studies that looked at technology for healthcare have also targeted Veterans with specific diagnoses (e.g., diabetes mellitus 11 ), leaving a substantial gap in our knowledge about Veterans with multi-morbidity and high acute healthcare utilization. This group of patients accounts for a disproportionate share of healthcare costs and are often at higher risk for adverse health outcomes. 12,13 Thus, these patients have been the focus of clinical interventions to improve outcomes and reduce utilization. 14,15 Internet technology may improve communication and healthcare access for this important at-risk group of patients, but such patients may also be more likely to have limited exposure and comfort with technology. Understanding technology-related beliefs for this group would help us determine the feasibility and acceptability of technology-enhanced clinical interventions.
Technology-enabled interventions targeting informal caregivers (i.e., family members or friends who provide unpaid care in the home for individuals with significant care needs) could also benefit higher risk patients, in addition to providing needed support for caregivers. Currently, around 5.5 million Veterans have informal caregivers; in the general U.S. population, 34 million receive informal care. 16 Informal caregivers are often responsible for communicating with healthcare teams, following medical recommendations, and transporting patients to clinical visits. 16,17 Given the substantial complexity of coordinating care, often competing with life demands of informal caregivers, technology-enabled interventions may offer significant benefits in access, communication, and decreased burden for caregivers and the patients they care for. However, to our knowledge, there have been no studies focused on Internet use or technology-related attitudes among informal caregivers.
To address acceptability and feasibility of technology-enabled interventions for these two important groups, we performed a secondary analysis of survey data on technology use and related attitudes from two ongoing randomized clinical trials: (1) a nurse-led case management intervention for Veterans with multi-morbidity and history of high acute care utilization and (2) a skills training program for informal caregivers of Veterans with substantial in-home needs. We first describe characteristics of Internet users compared with nonusers, frequency of Internet use, and devices utilized. Then, we present information on participants' willingness to communicate with healthcare teams via videoconferencing, for Internet users and nonusers. Finally, we evaluate characteristics associated with being comfortable with new technology devices “on your own,” as well as those associated with being comfortable only with in-person assistance.
Materials and Methods
Setting and Participants
Participants were enrolled in one of two ongoing randomized controlled trials at the Durham VA Medical Center (DVAMC): (1) a nurse-led telephone support program for Veterans with a recent emergency department (ED) visit and risk factors for repeat ED visits (DISPO ED, 18 NCT01717976) and (2) a skills training program for informal caregivers of Veterans with substantial in-home care needs (HI-FIVES, 19 NCT01777490). DISPO ED eligibility criteria were having established primary care at DVAMC, at least two chronic medical conditions, and at least one previous ED visit or hospitalization within 6 months before index ED visit. In HI-FIVES, Veterans with primary care at DVAMC and ongoing home care needs (i.e., at least one referral to home and community-based care or geriatric clinic consult in prior 6 months) were asked to identify primary caregivers by using the questions: “Do you have someone, a family member or a friend, who helps care for you due to your health problems?” and “What is the name of the family member or friend who cares for you most with daily activities?” In addition to the primary caregiver, 32% also had a paid caregiver. Eighty-eight percent of caregivers lived in the same house as Veterans, and 9% needed to drive to the Veterans' residences.
These studies were approved by the DVAMC Institutional Review Board.
Measures
Demographics and general health
Age, gender, race, and highest level of education were self-reported on enrollment. To address economic security, participants were asked “Which one of the following statements best describes your own personal economic situation?” Response options included “I am in good shape…,” “I am okay…,” “I am barely getting by…,” “I am falling behind…,” and “I am in serious financial trouble…” General health was assessed with the question “In general, how would you say your health is now?” Response options were “excellent,” “very good,” “good,” “fair,” or “poor.”
Internet use and technology-related attitudes
Participants reported their use of the Internet, willingness to communicate with healthcare teams via videoconferencing, and comfort with new technology devices (see Appendix for exact questions and response options). Briefly, Veterans and caregivers were asked whether they used the Internet in the past year, and if so, how often they accessed the Internet and what type of device they used. Participants also reported whether they had ever used videoconferencing, and if they would be willing to use videoconferencing via a variety of devices (Likert scale 1–5, anchored by 1 = “not at all willing” and 5 = “very willing”). We dichotomized responses with 4 or 5 as indicating willingness to use videoconferencing and other responses as not willing. Finally, comfort with attempting to use new technology devices was assessed for separate scenarios: if given in-person assistance, with telephone-based assistance, or “on your own.” Responses for each question were on Likert scales 1–5, anchored by 1 = “not at all comfortable” and 5 = “very comfortable.” We dichotomized responses with 4 or 5 indicating comfort with new technology in each of the scenarios, and other responses as not comfortable. Because we wished our outcome to clearly define positive willingness and comfort with technology, we did not include responses of 3, which was the mid-point on the scale, as indicating willingness or comfort. In addition, we created a dichotomized variable, using responses for all three scenarios with new technology, to determine which participants were only comfortable with in-person assistance (i.e., responded 4 or 5 with in-person assistance, but 3 or less for “on your own” and telephone assistance). Given that in-person assistance is likely the costliest and most challenging to implement, we wanted to better understand which participant characteristics may indicate that someone needed this higher level of assistance.
Statistical Analyses
We provide descriptive statistics of demographics and general health separately for Veteran and caregiver participants overall, as well as for Internet users and nonusers within each group. We performed bivariate comparisons of characteristics between Internet users and nonusers. We used two-sample t-tests for age and either χ 2 tests or exact Fisher's test for categorical data. We defined statistical significance as p-value <0.05.
We used two multivariable logistic regression models to examine associations of participant characteristics (described above) with two different dichotomous outcomes: (1) comfort on one's own with new technology devices or not and (2) comfort only with in-person assistance or not. We included Veteran and caregiver data in the same models, as we had no reason to believe that characteristics would be differentially associated with the outcomes, depending on Veteran or caregiver status. To assess for multi-collinearity among covariates, we examined covariate correlations and variance inflation factors. All analyses were conducted by using R version 3.2.4.
Results
The average age of Veteran participants was 59 years (standard deviation [SD] 12, range 25–88 years), 22% were women, and 49% were black. Nineteen percent had bachelor's degrees or postgraduate education, and 30% completed high school or less. Fifty-three percent reported that their economic situation was good or okay, 31% were barely getting by, and 17% were either falling behind or in serious trouble. Only 10% reported excellent or very good general health, 31% had good health, whereas 41% and 18% had fair and poor health, respectively.
The mean age among caregiver participants was 61 years (SD 11, range 27–85 years), 88% were women, and 44% were black. Thirty percent had bachelor's degrees or postgraduate education, and 28% had completed high school or less. Fifty-one percent of caregivers reported good or okay economic situation, 36% were barely getting by, and 13% were falling behind or in serious trouble. Twenty-nine percent had excellent or very good general health, 40% had good health, and 31% had fair or poor health.
The vast majority of participants used the Internet within the past year (81% of Veterans and 82% of caregivers). Table 1 summarizes the characteristics of Internet users compared with nonusers. For both Veterans and caregivers, educational status was different between Internet users and nonusers; age and gender were different only among Veterans; and race was different only for caregivers (Table 1). Forty-two percent of Veterans and 58% of caregivers had experience with videoconferencing; almost all those who had used videoconferencing also reported Internet use in the past year (98% and 96% for Veterans and caregivers, respectively).
Participant Characteristics
Characteristics of Internet users and nonusers were compared by using two-sample t-tests for age and either χ 2 tests or exact Fisher's test (for variables with cell counts of 5 or less) for remaining data.
Other includes American Indian or Alaska Native, Asian, Native Hawaiian, or Pacific Islander, or selection of multiple responses. Among Veterans, 17 had missing data on race.
Fourteen Veterans and one caregiver had missing data on economic security.
Six Veterans and one caregiver had missing data on general health.
SD, standard deviation.
Most participants who used the Internet in the past year reported being comfortable with it (73% for Veterans and 80% for caregivers). The majority of Internet users accessed the Internet at least a few times a week (83% for Veterans and 92% for caregivers, Fig. 1), and most used a computer within their home (81% for Veterans and 89% for caregivers, Fig. 2). Nearly a quarter of Internet users accessed the Internet by using multiple devices, including cellphone, tablet, and computer at home (Fig. 2). In addition, among Veterans who used the Internet, four participants accessed the Internet solely through a computer outside of the home.
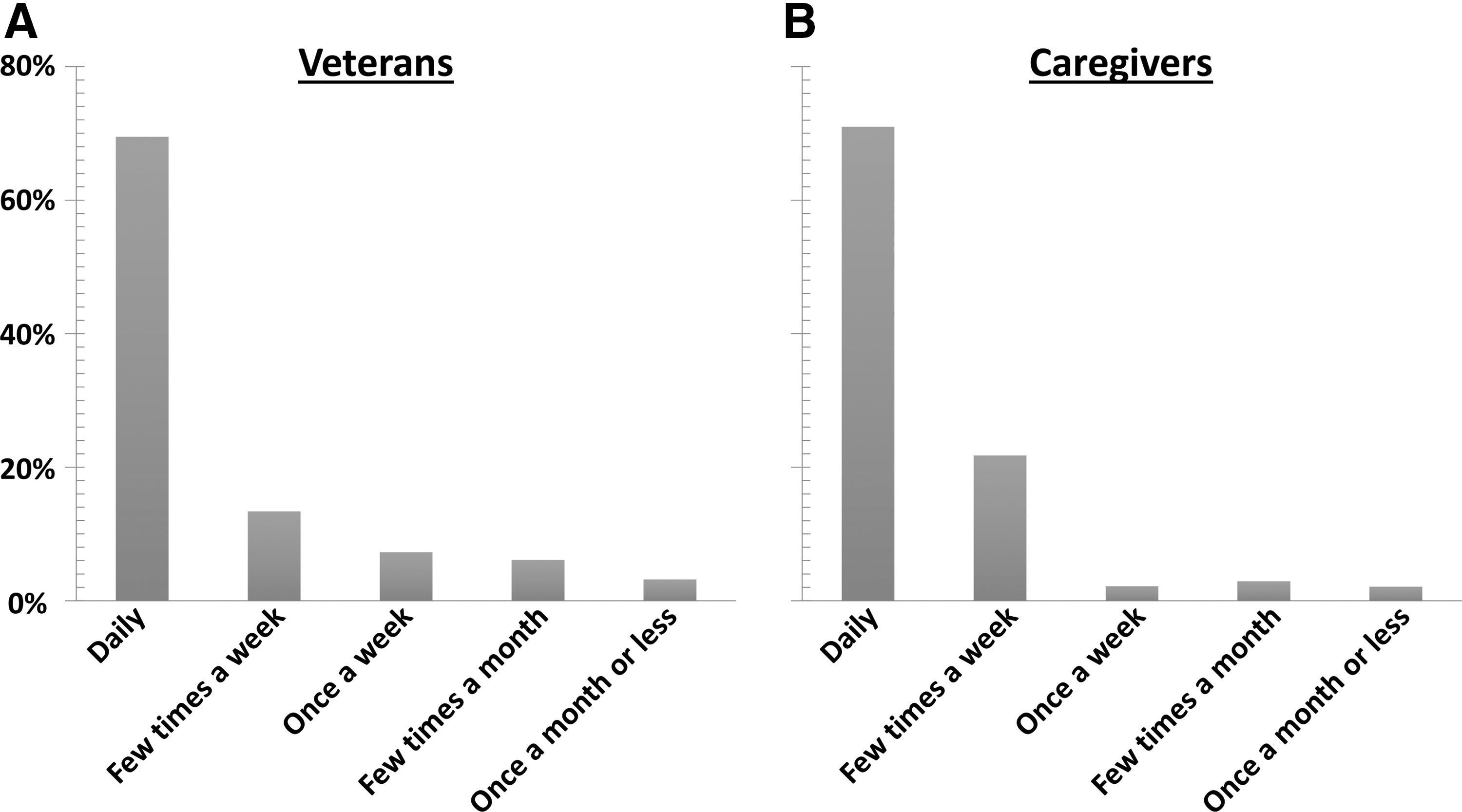
Frequency of Internet use. Proportion of Internet users among Veterans

Devices used to access Internet. Venn diagrams of different devices used by Veterans
A majority of participants were willing to communicate with their healthcare team via videoconferencing, if using a private device (77–82% of Veterans and 78–83% of caregivers, for cellphones, tablets, laptop, or other computer in home, Fig. 3). In contrast, 51% of Veterans and 41% of caregivers would be willing to communicate via videoconferencing through a computer outside of the home. A greater proportion of those who had used Internet in the past year were willing to use videoconferencing, no matter the specified device, compared with those who were nonusers (Fig. 3).

Willingness to communicate with healthcare team by videoconference. Proportions of Veterans
Eighty percent of Veterans and 85% of caregivers reported that they would be comfortable attempting to use a new technology device, if given in-person assistance. Fewer Veterans and caregivers were comfortable “on your own” (58% and 59%, respectively), or with assistance by phone (64% and 66%, respectively). Fourteen percent of Veterans and 17% of caregivers were comfortable with new technology only with in-person assistance, whereas 12% of Veterans and 10% of caregivers were not comfortable in any of the assistance scenarios. In multivariable logistic modeling, increased age was associated with lower odds of being comfortable on one's own (odds ratio [OR] 0.98, 95% confidence interval [CI] 0.96–0.99) and higher odds of being comfortable only with in-person assistance (OR 1.03, 95% CI 1.01–1.06; Table 2). Our model predicted that a 10-year increase in age (e.g., a 65-year-old person compared with a 55-year-old person) was associated with a 42% decrease in odds of being comfortable on one's own (OR 0.58) and a 100% increase in odds of being comfortable only with in-person assistance (OR 2.0). In contrast, having used Internet in the past year was associated with increased odds of being comfortable on one's own (OR 2.76, 95% CI 1.70–4.53; Table 2), but not with being comfortable only with in-person assistance.
Characteristics Associated with Comfort Attempting to Use New Technology Devices (N = 561)
Separate multivariable logistic models examined associations between baseline characteristics and two outcomes: (1) being comfortable on one's own, and (2) being comfortable only with in-person assistance. Being comfortable on one's own would indicate those who could fairly easily learn new applications or technology, and thus, would need minimal support when implementing new healthcare technology interventions. This outcome was defined as responding 4 or 5 (response options were 1–5, 1 = not at all, and 5 = very comfortable) to “How comfortable would you feel attempting to use a new technology device on your own?” In contrast, the second outcome of being comfortable only with in-person assistance would indicate that someone may need substantial help when introducing new technology in healthcare settings. We used a combination of participant responses to define this category—responses of 4 or 5 to “How comfortable would you feel attempting to use a new technology device with in-person assistance?” and 1–3 for similarly worded questions for “on your own” and “with over the phone assistance.” Modeling was performed for 561 participants who had complete data on baseline characteristics and outcomes of interest. The C-statistics were 0.683 and 0.605 for logistic models examining comfort “on your own,” and only with in-person assistance, respectively.
Compared with caregiver as the referent.
Other includes American Indian or Alaska Native, Asian, Native Hawaiian, or Pacific Islander, or selection of multiple responses.
CI, confidence interval; OR, odds ratio.
Discussion
We found high prevalence of Internet use among two groups who may benefit from technology-enabled interventions: (1) Veterans with multi-morbidity and history of acute healthcare utilization and (2) informal caregivers of Veterans with substantial in-home care needs. Consistent with previous results for Veterans and the general U.S. population, 5,8,10,11,20 most participants used the Internet at least weekly, via devices at home. Tsai and Rosenheck 8 found that 71% of Veterans reported Internet use, with 64% of these accessing the Internet daily. For Veterans with specific medical conditions, Cho et al. 11 reported that 59% of Veterans with diabetes had Internet access at home, and 62% of these used the Internet daily. For Veterans with serious mental health conditions, 70% reported Internet use, 58% of these with daily use, and 97% via a computer at home. 10 Our results also confirm that age and education are associated with differences in Internet use. 4 –6,8
In contrast with past results on technology use by Veterans 8 and Medicare beneficiaries, 6 health status was not different between Internet users and nonusers in our study. This difference may be due to poorer health of our Veteran participants, 58% of whom reported fair or poor health (Table 1). Past studies of Veterans had a majority with better health and not enrolled in VHA. 8,9 In addition, the study on Medicare beneficiaries included older participants (mean age 75 years), but only 25% of these reported fair or poor health. 6
Economic security also was not different between Internet users and nonusers, for both Veteran and caregiver participants. Past work looked at the association of self-reported household income with technology use for both Veterans 8 and the general U.S. population, 4 finding a higher likelihood of Internet use with each increase of $20,000–$25,000. We assessed perceived economic difficulty, and although less than half of Veterans and caregivers reported some difficulty (Table 1), it is plausible that many of our participants had fairly low incomes. Previous studies on Veterans have shown that those enrolled in VHA have lower incomes than both Veterans not enrolled in VHA and the general U.S. population (e.g., in 2010, 70% of VHA-enrolled Veterans, compared with 44% of non-VHA Veterans, had incomes less than $50,000, 8 the median income for U.S. households).
We also found that most Veterans and caregivers were willing to videoconference with their healthcare teams, but fewer were willing to do so via computers outside of home. In ongoing qualitative interviews with Veterans, multiple participants noted privacy concerns with videoconferencing on a device outside of home (data not shown). Despite the presence of such concerns, it is notable that half of Veterans and two-fifth of caregivers reported that they were willing to use computers outside of home for videoconferencing. This level of acceptability for videoconferencing may be due to the high prevalence of Internet exposure, or reflect substantial perceived benefits in increased access and flexibility of contact by participants.
Internet users were somewhat more willing to videoconference, and Internet use was associated with higher odds of being comfortable on one's own with new technology. In a previous study examining patient use of secure messaging portals, Internet use was also found to mediate differences in portal use associated with income, educational status, and race. 5 Recent Internet use reflects participants' ability to access the Internet and likely familiarity with various devices; thus, assessing recent Internet use would be a straight-forward way to identify people who are likely to engage in technology-enhanced healthcare interventions with little assistance.
In contrast, older age was associated with lower odds of being comfortable on one's own with new technology and higher odds of being comfortable only with in-person assistance. This is consistent with previous work showing that older adults have less Internet exposure and are more likely to report barriers to using new technology. For example, LeRouge et al. 7 found that only 26% of adults 65 and older reported that they “would have no problem using” videoconferencing, compared with 53% of those 64 and younger.
Problems related to technology are common during initiation of technology-enhanced interventions, 21,22 and in-person assistance offers the most support for trouble-shooting and reassurance of participants. Previously, in-person and remote technical assistance were included in chronic disease management group visits via videoconferencing. 21,22 In another study of a Web-based psychoeducation program for informal caregivers of adults with dementia, participants were trained to use devices during initial home visits, and had telephone-based support afterward. 23 Such assistance may be particularly beneficial for older participants and those without recent experience with the Internet. In addition, although very few of our participants accessed the Internet less than once weekly, individuals with such low frequency use may lack skills and comfort with technology in a healthcare context; thus, they may also benefit from assistance with technology-enhanced clinical interventions.
In our study, if in-person assistance were available, 29% more Veterans and 27% more caregivers would be comfortable with new devices, as compared with the scenario “on your own.” If telephone assistance were available, 15% more Veterans and 14% more caregivers would be comfortable with new devices. Thus, telephone assistance would improve the number of individuals who would be comfortable with new technology, but did not appear to help to the same degree as in-person assistance. However, given savings in cost and increased feasibility, particularly for participants who reside far from clinical sites, telephone-based support may be the best option in certain situations. Other ways to provide technical support include peer consultants, used as part of implementation of a secure VHA patient portal, 24 and proactively engaging family members or other social support who are familiar with Internet technology. Thus, offering various forms of technical support could improve uptake of existing Internet-based VHA applications that have had limited penetrance (e.g., secure patient portal 25 ), in addition to aiding the implementation of technology-enhanced interventions that are not yet widely available within the VHA (e.g., videoconferencing with patients at home 26,27 ). It will also be important to examine the effectiveness of different modes of technical support and assistance specifically for healthcare technology applications, which may be less flexible and/or more cumbersome due to requirements for privacy and other institutional concerns (e.g., need for scheduling appointments or additional equipment needed at home 26 ). Further, for technology-enhanced interventions to increase access and improve delivery of patient-centered care, it will be critical that technology applications can integrate with existing clinical services and health records.
There are several limitations to our study. Our participants were all recruited at a single site, and they were not nationally representative of Veterans and their caregivers. There are also significant differences between Veteran and non-Veteran patients, 12,28 and there may be differences between caregivers of Veterans and those caring for non-Veterans; our results may not generalize to non-Veteran U.S. patients and their caregivers. Self-reported information on participant characteristics and Internet use may have been affected by recall and/or social desirability bias. In addition, our results describe attitudes and perceptions, and they may not correspond with actual behavior when participants were asked to engage with new technology in the healthcare context. We asked about any Internet use in the past year and experience with videoconferencing in general; thus, we do not know whether these were health-related and if participants were satisfied with these experiences. However, we assessed for willingness to engage in videoconferencing specifically for healthcare communications, which directly addresses acceptability of such technology for health reasons. It is also plausible that comfort with new devices, in general, would be applicable to technology used in healthcare settings, but future studies should specifically examine such questions. Finally, we did not address the acceptability of videoconferencing and other Internet-enhanced healthcare interventions from the perspective of clinicians. Future work should seek to better understand provider and staff factors that promote or reduce uptake of such technologies.
Despite these limitations, our results support feasibility and acceptability of technology-enhanced interventions for Veterans with multi-morbidity and high acute care utilization, and informal caregivers of Veterans. Internet use was highly prevalent, and the vast majority was willing to use videoconferencing to communicate with healthcare providers, if done so in a private setting. This work indicates that those without recent Internet use and older participants may particularly benefit from in-person assistance when introducing new technology as part of clinical interventions. Future work should determine the most effective strategies for incorporating in-person and/or telephone-based technical support for technology-enabled interventions.
Footnotes
Acknowledgments
The authors wish to thank Katina Morris and Laurie Marbrey for help with administration of surveys examining Internet use and attitudes toward technology. Funding was provided by VA Health Services Research & Development (HSR&D) for DISPO ED (IIR 12-052, PI Hastings) and for HI-FIVES (IIR 11-345, PI Van Houtven). This work was also supported by the Center of Innovation for Health Services Research in Primary Care (CIN 13-410). Fellowship support for W.D.-P. was provided by grant number TPH 21-024 from the VA Office of Academic Affiliations. The sponsors had no role in the design or conduct of this study. Views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the VA or the U.S. government.
Disclosure Statement
No competing financial interests exist.