
Abstract
Background:
Equality in healthcare between urban and rural areas is problematic in France. Telemedicine networks are expected to improve equality in expertise assessment. We aimed to evaluate the use and impact of a regional rural French telemedicine network, dedicated to medical and surgical neurological emergencies, on interhospital patient transfers.
Methods:
Eight community hospital emergency departments were remotely connected to the only university hospital in Franche-Comté, France. We prospectively obtained data from all patients consecutively admitted to emergency care departments in the region and who received medical or neurosurgical expertise by telemedicine from January 2002 to December 2015. The reasons for requesting expertise, number of requested neurological opinions, and interhospital patient transfers were analyzed. Economic savings were determined by estimating the cost of avoided transfers.
Results:
A total of 23,710 patients had telemedicine consultations in the region. The network was used by every community hospital (independently of the existence of local neurological teams). These consultations were overwhelmingly for cases of stroke (30%) and head or spinal injuries (36%). Cerebral tumors represented 9% of teleconsultations. In 2015, 75% of patients admitted to the remote hospitals that did not have onsite neurological expertise nevertheless received neurovascular tele-expertise. The rate of thrombolyzed patients dramatically increased within 13 years regionally (9.9%) and 33.5% of thrombolyses were performed by telemedicine. The number of patients examined by telemedicine and admitted for head or spinal injuries also increased over the 13-year period (12% vs. 21%). Secondary interhospital transfers were halved for both pathologies. The estimated saving is ∼€3.5 million.
Conclusion:
Telemedicine networks facilitate acute-phase neurological assessment and prevent unnecessary secondary interhospital transfers.
Introduction
Neurological emergencies are frequent in emergencies departments. 1 –3 The number of practitioners has been decreasing for decades all around France and even more in rural areas. 4 Thus, telemedicine appears as the way of enabling equality to neurological expertise assessment. Moreover, telemedicine reduces costs and avoids useless or risky transfers. 5
If studies demonstrating the usefulness of telestroke at the acute stage are now numerous, less is known about the efficiency of a mutualized network dedicated to neurological, neurosurgical, or neuroradiological emergency. 6 –10
We report the evaluation of a 13-year-old regional telemedicine network specialized in every kind of neurological emergencies. The aim of the study was to describe the evolution of neurological expertise and of interhospital transfer rates since the network deployment.
Materials and Methods
RUN-FC telemedicine network
Réseau Urgences Neurologiques de Franche-Comté (RUN-FC) is a cooperation of the only academic hospital of the region with eight community hospitals having an emergency care department with at least a computed tomography (CT) scan. It is a drip and ship network. It was planned to enable neurological, neuroradiological, or neurosurgical assessment all over Franche Comté. Franche Comté is a French rural and hilly region. This region spans 16,202 km2 and its estimated population is around 1,177,906 inhabitants. Before the implementation of the network, only a comprehensive stroke unit and a department of neurosurgery existed through the region. At the network launch, only three community hospitals had a department of neurology but no stroke unit. Today, four community hospitals have a department of neurology among them are two stroke units (created, respectively, in 2010 and 2012). The four others have no local neurological expertise and no neurosurgical expertise since no other department of neurosurgery has been created. Each emergency care department of every community hospital had a room equipped with telemedicine systems.
The onsite physician phones the neurologist, the radiologist, or the neurosurgeon expert at the academic hospital. Patients are examined in real time by bidirectional videoconference (high-speed videoconference system). Digital data of CT or magnetic resonance imaging examinations are transferred. Written summaries are faxed or sent electronically to the enquiring hospital just after finishing the consultation and are validated by the remote physician. The system runs on dedicated stationary workstations. All members of the remote emergency rooms and experts of the academic hospital underwent training to the telemedicine system used.
Patients
We prospectively obtained data from all patients consecutively admitted to emergency care departments of the region and who had an expertise given by telemedicine from January 2002 to December 2015. In addition, discharge diagnoses were collected regularly for those patients by an independent remote nurse. Standardized information gathered were ground of appeal, location of the emergency care service, sociodemographic characteristics, treatment strategic, and transfer decision. Moreover, number of patients admitted to these hospitals with a final diagnosis of stroke or head injury was obtained, thanks to the International Classification of Diseases quotation. Codes used were I60, I61, I62, I63, I64, and G45, SO61–69.
Analyzed parameters and statistical analysis
Four groups of pathologies were done: stroke, head injuries, spinal injuries, and tumors. We analyzed the evolution of the number of calls for each group through the years but also through the region. Two periods were distinguished: 2002–2008 (the estimated training period) and 2009–2015 (the routine period), and community hospitals were divided into two groups: Neuro-pos and Neuro-neg. Neuro-pos refers to the hospitals with a department of neurology and Neuro-neg refers those without department of neurology. The χ2 test was used for differences in binary data. The rate of neurological or neurosurgical expertise done via telemedicine in each group was also estimated by the ratio of the patients who underwent telemedicine expertise out of those admitted from the same pathology, and the savings were estimated by the cost of avoided transfers.
Results
A total of 23,710 patients underwent a telemedicine expertise for a neurological emergency from 2002 to 2015. As shown in Figure 1, the number of calls had tripled within the first six years and has rounded since then to 2,000 calls per year. The demands for expertise came from the entire region and all the community hospitals used the system. The needs of expertise were independent of the existence of a department of neurology.
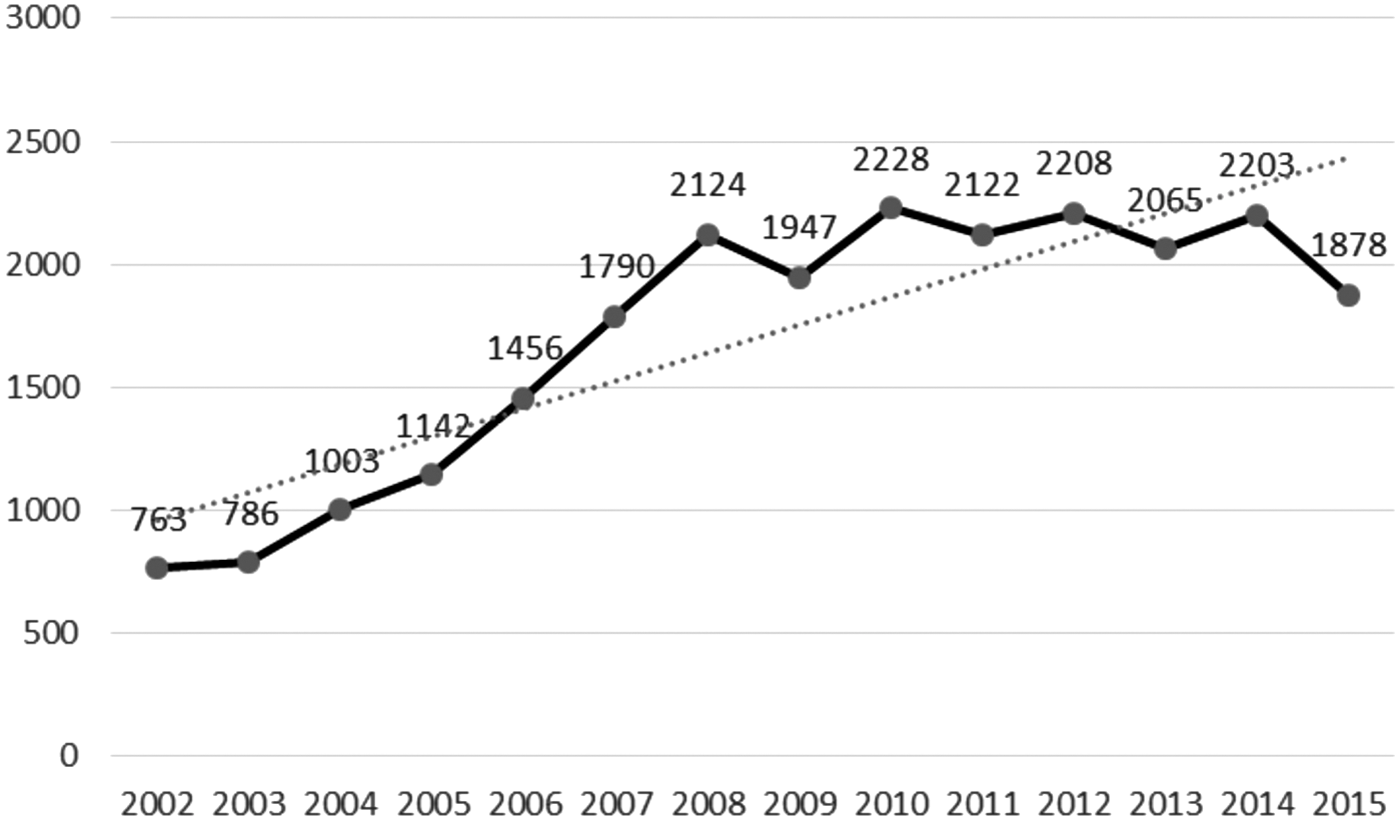
Evolution of calls.
Reason to call was in 30% stroke suspicion, in 36% head or spinal injury, 9% cerebral tumor discovery, and 24% other requests (headache, seizures, etc.), and this distribution had not changed within the 13 years analyzed.
The evolution of calls for each group of pathology during the two periods studied and according to the category of hospital that requested are summarized in Table 1.
Evolution of Calls Second to the Period and Presence or Not of Local Neurological Expertise
Stroke patients
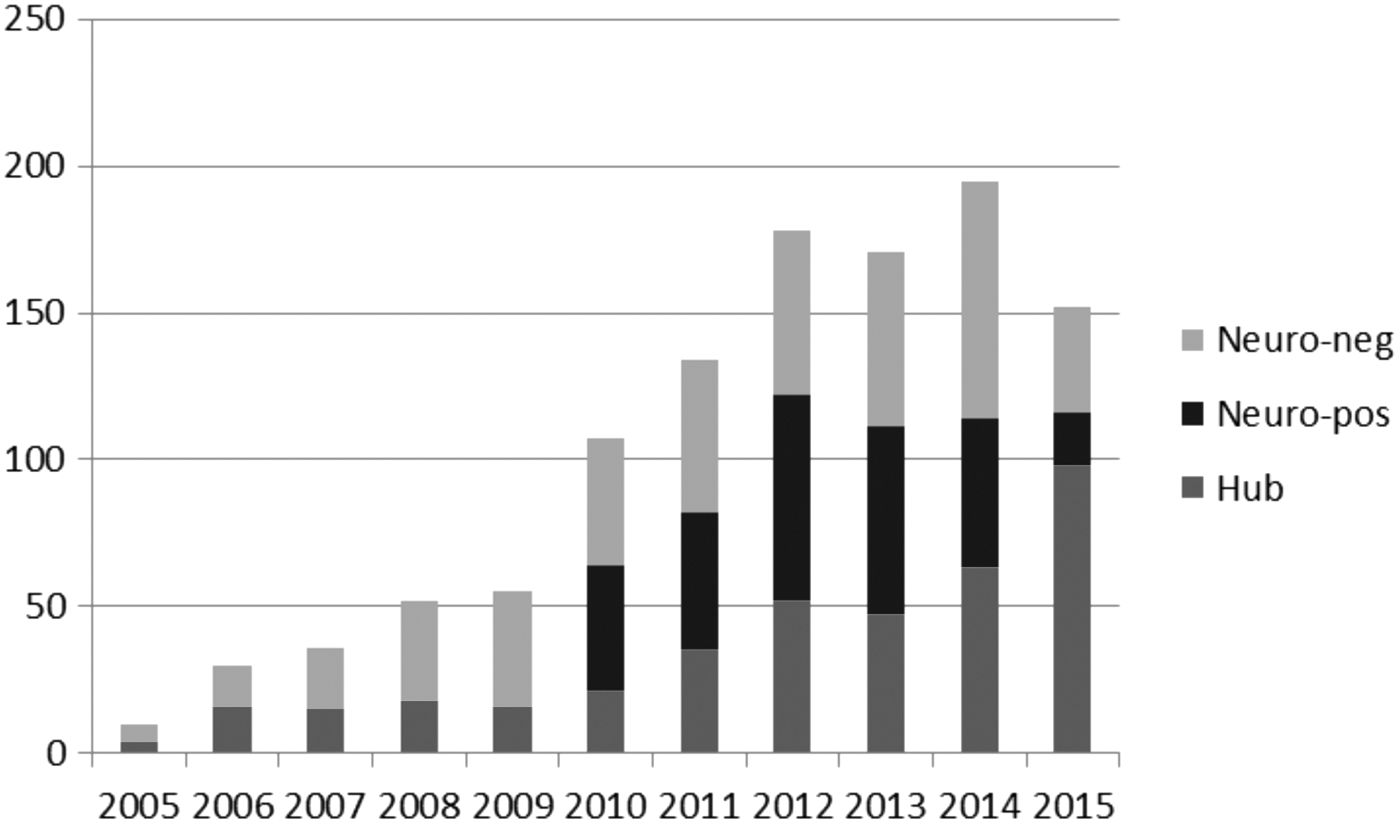
In the stroke group, the ratio of patients admitted for stroke and who underwent telemedicine stroke neurologist expertise peaked from 16% to 75.3% in the community hospital without neurologists on site. The evolution of calls for stroke had significantly increased between the two studied periods with a higher rate of tele-expertise for patients admitted in Neuro-neg community centers (Fig. 2).

Evolution of ratio of neurovascular expertise Neuro-neg and Neuro-pos.
Since 2005, telethrombolyses were started. In 2015, the regional rate of thrombolysis was 9.9%. The number of telethrombolyses has increased dramatically. At the end of 2009, 29% of all thrombolyses were administered by telemedecine in Neuro-neg centers. At the end of 2015, 33.5% were done after a teleconsultation (Fig. 3).
Evolution of thrombolysis.
Head injuries
Neurosurgeon expertise had also been required in head injury cases (Fig. 4). Comparing, the periods studied, the number of calls was significantly higher for Neuro-neg than for Neuro-pos between both periods.

Evolution of neurosurgeon expertise in head injury.
The telemedecine network had also been used for patients suffering spinal traumatism with a significant increase of calls between both periods for patients admitted to emergency care department without neurological assessment (12% vs. 21%). Telemedecine use was less frequent for tumors and the increase noted between the studied periods was not significative (15% vs. 18%).
Evolution of transfers
Transfers have decreased for all pathologies since the creation of the network and had been divided by half through the first period (Fig. 5). The difference between the studied periods is statistically significant. During the same period, savings done by keeping patients on site were estimated to be 3.5 million euros (42 million USD).
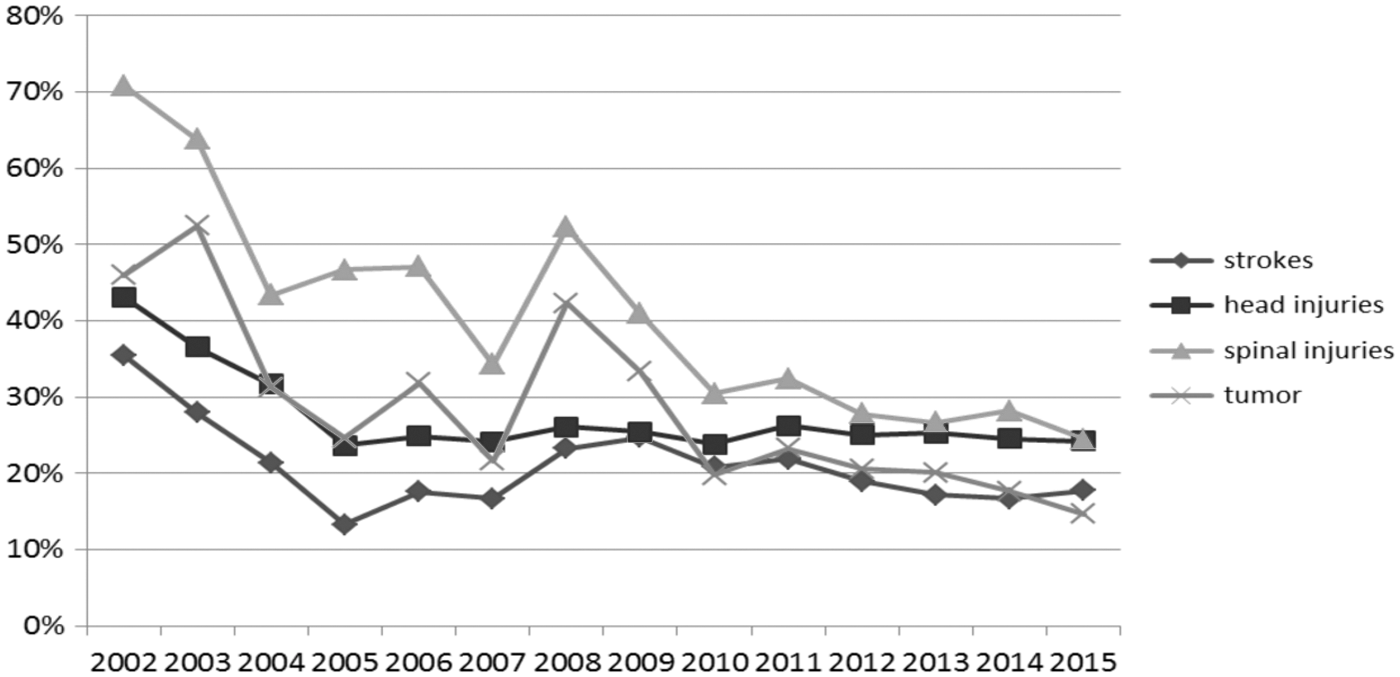
Transfers evolution.
Discussion
The increased use of our telemedicine system illustrates the need of neurological expertise in our rural region. The need is due to the high frequency of neurological emergencies up to 14% in Moulin's work and also the global lack of physicians in rural areas. 7,8,11 –18 The high use of the system for stroke patients can be explained by the high prevalence of stroke. Recent estimations indicated that the global prevalence rate was 5 per 1,000 person‐years, corresponding to 33 million people living after a stroke. 19 –21 Functional outcome of stroke patients can be enhanced by the thrombolysis if given within 4H30. 22 But this first curative treatment must be delivered by physicians specialized in stroke. Indeed, European and French approval of alteplase in acute stroke restricts application of treatment to physicians who are experimented and trained in neurological care. 23 This neurovascular expertise can be given by telemedicine with the same clinical reliability and also the same efficiency and security. 8 At the beginning of our network, thrombolytic therapy was provided only in 0.6% of patients. In 2015, 9.9% of the patients admitted for stroke underwent thrombolysis. This enhancement was also found in previous studies but the rate of alteplase administration could probably be improved as shown in the Houston paramedic and emergency stroke treatment (HoPSTO) experimentation. 8,9,24 The main findings of our 14-year experience of telestroke are the improvement in thrombolysis service and the large assessment to neurovascular expertise offering state-of-the-art acute stroke care.
Head injuries were the second most frequent reason to call in our experience. It can be explained by the frequency and the potential severity of this pathology. In fact, injuries are a leading public health problem worldwide; accounting for an estimated 10% of global mortality rate and in remote regions, the lack of equipment, insufficient personnel, or technical resources contributes to a less than optimal environment for acute injury management. 25,26 In our work, ∼30% of patients admitted for head injury required a neurosurgeon expertise. This expertise based on clinical findings and neuroradiological information facilitated immediate decision-making. The consequence was a dramatic decrease of transfers since the deployment of the system. These observations were the same in other experimentations and no significant changes in mortality rate in the nontransferred patients were noted. 25 The decrease of transfers noticed in our work induced obviously a cost reduction. This was also demonstrated in other drip and ship model networks. 26 –29
This study has a few limitations. Our single network represents prospectively collected registry data. Therefore, selection and coding biases as well as data collected errors cannot be excluded. The analysis of secondary transfers is based on the recommendations of the physicians providing telemedicine consultations. These recommendations may not have been applied and some patients may have been transferred to other hospitals. Nevertheless, the lack of hospital in the region reduces this risk. The outcome of nontransferred patients is not known. Patients' and users' satisfaction were not taken into account.
Conclusion
The teleneurological emergency network RUN-FC is a model of mutualized regional network implemented for 14 years. This study illustrates the use and the effects of that kind of network. It may be informative for future experimentations since stroke management nowadays might require neurological, neurosurgical, and neuroradiological expertise.
Footnotes
Acknowledgment
The telemedicine system was funded by the healthcare system. There is no other specific funding for this study.
Disclosure Statement
No competing financial interests exist.