
Abstract
Purpose:
Heart failure (HF) is common in older adults. With increases in technology use among older adults, mobile applications may provide a solution for older adults to self-manage symptoms of HF. This article discusses the development and acceptability of a HF symptom-tracking mobile application (HF app).
Methodology:
The HF app was developed to allow patients to track their symptoms of HF. Thirty (N = 30) older adults completed an acceptability survey after using the mobile app. The survey used Likert items and open-ended feedback questions.
Results:
Overall, the acceptability feedback from users was positive with participants indicating that the HF app was both easy to use and understand. Participants identified recommendations for improvement including additional symptoms to track and the inclusion of instructions and reminders.
Conclusion:
HF is common in older adults, and acceptability of mobile apps is of key importance. The HF app is an acceptable tool for older patients with HF to self-manage their symptoms, identify patterns, and changes in symptoms, and ultimately prevent HF readmission.
Introduction
Approximately 915,000 individuals are newly diagnosed with heart failure (HF) each year, with incident rates highest among older adults, particularly males and people of color. 1 With a booming aging population, it is estimated that nearly 8 million people will have HF by 2030. 2 HF is the leading discharge diagnosis and the number one reason for hospital readmission among Medicare beneficiaries, and is a main driver of cost. 3 –6 With HF, patients often experience multiple symptoms simultaneously, and a change in symptoms can indicate impending HF decompensation. 7,8 HF self-management can be critical for many patients to control the disease and avoid decompensation. 9 –11 This requires self-monitoring of daily weight for fluid accumulation and symptom recognition. Early identification of weight gain and potentially problematic symptoms allows a patient and their caregivers to intervene before hospitalization is needed.
Older adults are increasingly using smart phones and mobile applications (apps). 12 As such, providing self-management mobile apps to help older adults with HF monitor their symptoms may improve HF health outcomes and decrease healthcare utilization. 13 –15 However, there may be biases against using such tools given misperceptions about capacity and desire for use among the elderly. To overcome these biases, it is critical to overcome likely barriers to the use of mobile apps among older adults, 16,17 through assessment of the acceptability of proposed tools to improve design and user engagement. The purpose of this project was to develop a HF symptom-tracking mobile application (the HF app) and to test the acceptability of the app among potential older users.
Materials and Methods
Prototype Development
The HF symptom-tracker application (HF app) was initially developed with the overall goal to monitor the effect of research interventions. The HF app was designed to allow older adults with HF to record their weight, log their symptoms, and symptom severity (Fig. 1). Areas monitored included weight, fatigue, edema, shortness of breath, cough, stomach bloat, feeling sad, and feeling anxious (Fig. 2). Each item was dichotomous and only in cases of an affirmative response would a slider appear to indicate the symptom severity.
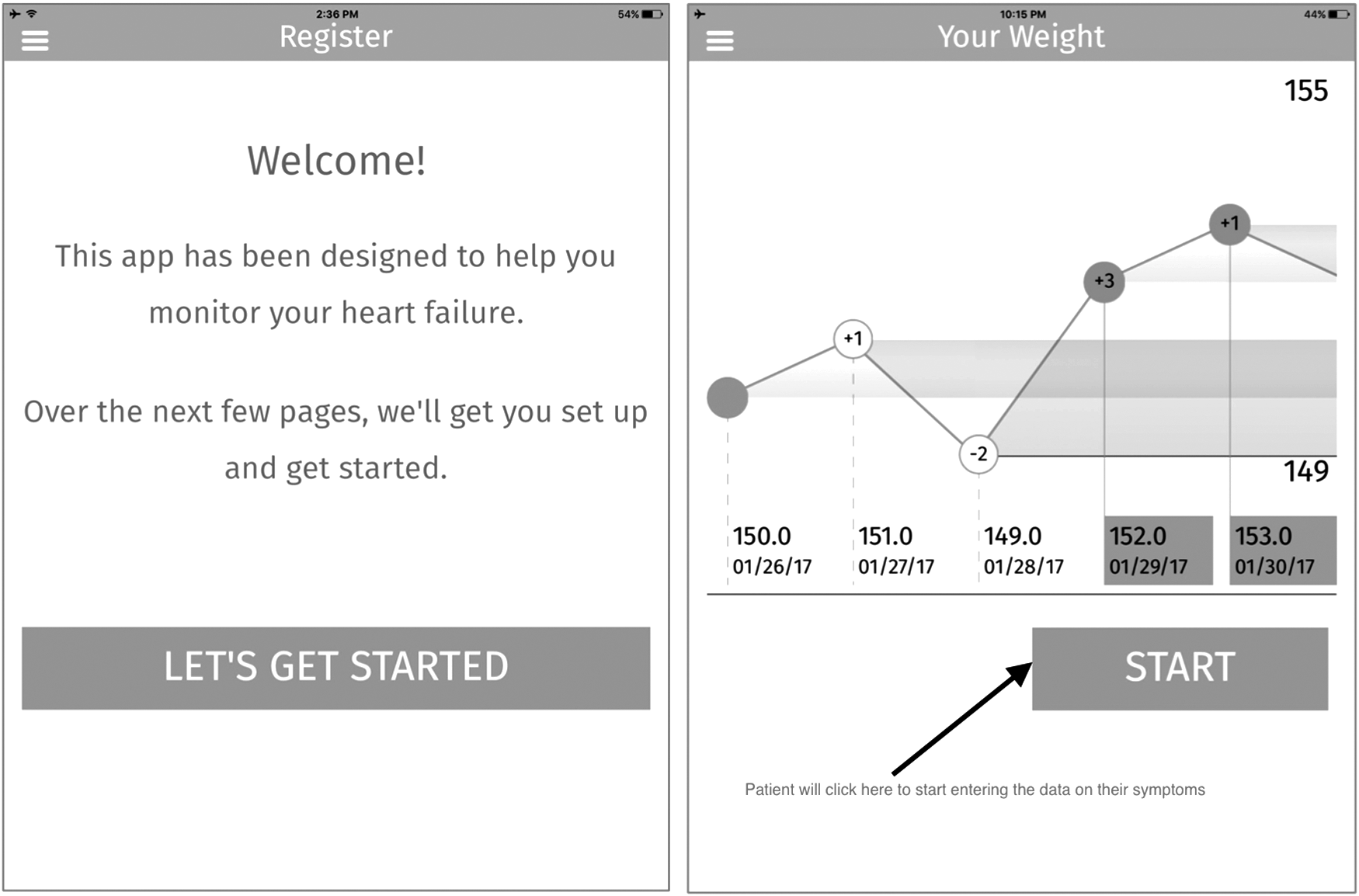
Heart Failure Application Start Screen and Weight Tracking Report.
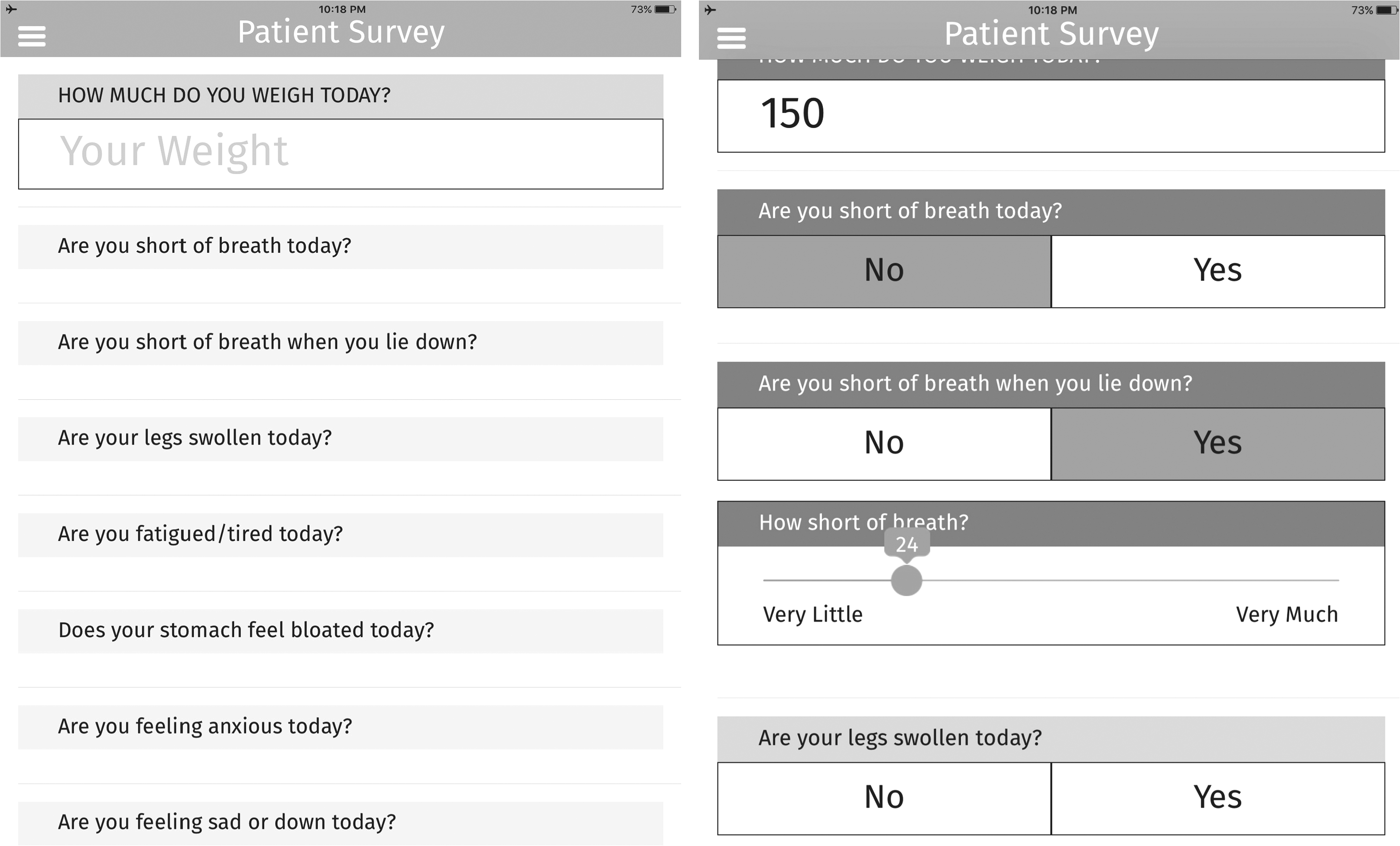
Heart Failure Application Symptom Tracking Screens.
The HF app was available on the iPad and downloaded from the Apple app store. There was no identifying information used in HF app; a six-digit username and four-digit pin were used to connect patient information to a separate database. The backend used to collect data from the application and export it for use in external reporting tools ran on an Amazon commercial, HIPPA-compliant Web Services EC2 t2.Micro instance with 128 bit SSL encryption.
Acceptability Testing
The HF app was evaluated for acceptability by patients more than the age of 60 with a pen and paper survey. The survey comprised two sections. The first section included 18 items measured on a 5-point Likert scale from strongly agree to strongly disagree. Questions inquired about their understanding of the app, ability to use the app, and ability to report symptoms through the app. The second section included open-ended questions for specific changes or additions and potential caregivers' use of the app. We examined the differences in responses by participant characteristics (age, race/ethnicity, and gender) using chi-square and correlation as appropriate. The open-ended responses were analyzed using magnitude coding, a process that quantifies participants' answers, highlighting the most frequent comments.
Results
Participants
To evaluate the prototype, 30 patients were recruited from HF clinics in Denver at the University of Colorado Hospital and at the University Hospital Cleveland Medical Center in Cleveland, Ohio. Participants were mostly female (60%), black (63%), and a mean of 66 ± 18 years of age (Table 1).
Participant Characteristics (N = 30)
Denver site only.
HF, heart failure; SD, standard deviation.
Acceptability
Overall, the acceptability feedback from users was positive with participants indicating that the HF app was easy to use, understand, and navigate (Table 2). Participants liked the general design, but sought the addition of specific symptoms, improvement of navigation features, and enhanced instructions. There were no differences in responses by race, ethnicity, or gender. Older age was significantly associated with a self-identified need for help in ongoing use of the HF app (r = 0.462, p = 0.010).
Acceptability Summary
There were several potential improvements identified by participants. First, some participants suggested tracking additional items, including heart palpitations, blood pressure, exercise, and water intake. Two participants also noted that they did not understand the word “fatigued.” Participants recommended adding specific features, such as reminders, instructions for using the HF app, patient-specific symptoms, and HF information to support symptom management.
Discussion
Currently there are few high-quality, commercially available mobile apps for the management of HF. 18 Also, there is little peer-reviewed literature assessing the acceptability, functionality, and efficacy of such apps. 18,19 We developed a HF symptom-tracking app and, as a critical first step, assessed the acceptability of the app with older adults. Because HF results in high healthcare utilization, specifically hospital readmissions, mobile apps such as the HF app may help patients, caregivers, and providers better manage HF symptoms, care utilization, and costs. 20 The HF app is a usable program for tracking symptoms of HF, which is central to HF management. The feasibility of the HF app should be examined to determine whether older adults will use the program and enter symptom data over time.
Several improvements to the app should be incorporated for future use, and instructions for use should be provided to future users. Because age was associated with a need for assistance to use the app, instructions and support from caregivers will be important to engage older patients with the HF app. Final changes to the HF app should also include improvements in mobile platform capability (in addition to iPad) and specific HF information important to the patient.
HF is common in older adults, and acceptability of mobile apps is of key importance. Current barriers to mobile apps among older adults should not deter the development of digital programs that can be used to improve HF care. The HF app is a useful tool to help older patients with HF self-manage their symptoms, identify patterns and changes in symptoms, and ultimately prevent HF readmission. Next steps in this process will require updates to the HF app, followed by usability testing to observe and document standard usability metrics, 21 followed by a randomized trial of the app efficacy for improving HF self-management and reduced hospital admissions and readmissions.
Footnotes
Acknowledgments
The authors thank DXY, Inc. for its assistance with the development of the HF symptom-tracker mobile application. This research was funded by the McGregor Foundation and the National Institute on Aging (T32AG044296-02).
Disclosure Statement
No competing financial interests exist.