
Abstract
Background:
Despite a recognized need for improved communications and logistics in high acuity situations, the integration of telemedicine services into the mainstream health services has been difficult. This study reports on the opinions of Romanian professional responders to mass casualty incidents and disasters regarding the use and requirements of specific electronic medical documentation solutions.
Materials and Methods:
Doctors, nurses, paramedics, and fire department officers participated in a customized online structured questionnaire. To assess factors associated with the current use of information technology and the willingness to adopt an exclusive optimized electronic system, a multivariate analysis was performed. Logistic regression was used for free input key elements regarding the most useful technical and operative improvements and medical documentation solutions for large-scale events.
Results:
A total of 536 respondents provided answers between the second half of the year 2014 and the first half of the year 2015. Doctors and nurses were the most frequent users of documentation techniques, especially if they were employed at a high-level emergency care center. Professionals' duties were perceived as increasingly impaired by the use of current electronic systems as those duties became more complex. All respondents favored an optimized large-scale event electronic solution, emphasizing the need for enhanced communications, technical equipment, cooperation, and workflow mainly by integrating mobile devices, dedicated software, remote databases, and interlink capabilities.
Conclusions:
Professionals support the implementation of an integrated electronic system for large-scale events if outlined requirements are met to maximize user acceptance.
Introduction
Telemedicine has proven to be not only a valid alternative within the classical healthcare process, but also a supplementary tool, providing features and benefits that would otherwise be unavailable locally. This makes it useful not only for underserved geographical areas, but also for critical cases where time is of the essence.
Acting as a force multiplier, telemedicine can address complex issues independent of location by interlinking medicine, public health authorities, civil services, as well as remote expertise, to assist overwhelmed local resources. Its application has been demonstrated to be appropriate for real and simulated mass casualty incidents and disaster (MCI-Ds) scenarios. 1 –3 Improvements in patient triage, monitoring, medical management, remote medical assistance, and disaster recovery support are undeniable benefits in stressful situations, contributing to a structured approach in event management. 4 –6
In large-scale events, the visual representation of unfolding processes by using object-oriented modeling tools may optimize medical and operational workflows. Using a field electronic medical record system makes conventional paper methods obsolete provided the case that there are no significant technological challenges. 7 Victim tracking and status evaluation are significantly improved, while documentation standards are enhanced. 4,7,8
Despite the potential benefit, telemedicine has not met expectations in terms of in-the-field application. 9 Although there is an acute need to establish telemedicine programs in high-risk areas, 10 acceptance has been slow within the mainstream health services. This is true despite the fact that its perceived usefulness ought to impact the behavioral intention to use it. 11 Cited reasons for unsuccessful deployment of telemedicine refer mainly to technology, regulations, and licensing and costs, but there are also concerns regarding physician buy-in and patient acceptance. This brings up controversies since patients, medical staff, hospital executives, and cultural issues are also cited not to interfere with its implementation. 12,13
Given the diversity of telemedicine solutions that may be applied in MCI-Ds settings, as well as the multitude of factors hindering their application, it is reasonable to investigate factors impacting variations in clinical acceptance, expansion, and sustainability. 13,14 Before implementing such systems, it is worth investing in studies attempting to identify predictors of success or failure to modify their influence. 15 Stakeholder participation, particularly clinicians, early in the design process is a key element for success, while pilot projects should be designed with a maximum degree of integration into the existing care system. 9,16 –18
Over the last 10 years, the Romanian Ministry of Health has implemented various telemedicine initiatives designed to improve specialist care in distant emergency medical centers as well as in prehospital settings for individual selected cases. The current study reports on the topic of emergency personnel familiarity and acceptance of electronic documentation methods and their opinions regarding a prospective telemedicine solution proposed for the MCI-D setting in Romania. These results can be extrapolated and integrated across the region and Europe as well as other locations worldwide.
Materials and Methods
This study is a part of a larger research project that aims to develop a customized telemedicine solution for MCI-Ds rescue efforts as an extension of current emergency management operations. The first phase of the project consists of inquiring upon current procedures followed by inviting study participants to point out specific requirements and features of a future system that they would regard as beneficial to their work and agree to utilize. The study methodology utilized in this study is based on similar work. 19
Selection Criteria
The current study recruited all participants to a nationwide comprehensive MCI-D training course, which took part for the second half of the year 2013. Each week-long training session included doctors, nurses, paramedics, and fire department officers. Participation was not mandatory but based on an informed opt-in process before the beginning of the program. Experienced specialists from the largest emergency situations nonprofit organization in Romania provided participation instructions. All participants were informed of their right to opt out of the study at any time of their choosing. We obtained approval for the overall project, including the current study, from the Institutional Review Board of the host institution, the Tîrgu Mureş Emergency Clinical County Hospital.
Inquiry Process
Program enrollment was based upon personal credentials, including the participants' name, e-mail address, agency, geographical origin, and other specific information requested by the organizers. The e-mail address was used as a username for all online instructional support. Participants also gave their consent for using the registration credentials for the purposes of the program, including the current study.
A master questionnaire was developed addressing specific aspects of large-scale events, interventions, as well as targeted questions regarding the use of information technology in these settings. The current study refers exclusively to the latter.
The survey was implemented by using a dedicated Web-based application, connected to a secured database, which sent e-mail invitations to all trained participants, and collected individual responses. An alphanumeric unique identifier was assigned to each subject and included in the survey URL. The researchers were blinded to personal credentials, exposing only the profession of the subject (doctor, nurse, paramedic, or officer). This was done for response tracking purposes to maximize response rate by reissuing e-mail invitations in case no response was obtained for a certain period of time. This timeframe was set to a week. In total, a particular subject would receive three e-mail invitations at most should no response be received.
The first invitations were sent in early 2014 and the initial assumption was that by the end of that year the data collection process would be concluded due to the absence of new input. However, survey responses continued to arrive through early 2015 when the process was terminated.
Survey
The questionnaire included nine questions regarding participants' demographics, their past participation in a real MCI-D setting, the general utilization of information technology at their specific workplace, and particularly in an MCI-D setting. Assessment of a subjects' opinion regarding a certain topic included the use of a 5-point Likert scale with the exception of a single three options staged question regarding the exclusive use of an electronic data documentation solution. We inquired on each participant's opinion on the implementation of new technical or operative solutions as well as their opinion on the best practice for patient data documentation in an MCI-D setting by allowing free text inputs. The questionnaire is shown in Table 1.
Study Questionnaire Used
Statistical Analysis
We first performed the descriptive analysis of the demographic data to describe the population characteristics. The chi-squared test for independence was used when examining differences between response behaviors among subject groups. We used the Mann–Whitney U or the Kruskal–Wallis test of variance to compare differences between groups for the questions where the subject's opinion was assessed, the ANOVA test to compare differences in age groups, and Pearson's chi-squared test or Fisher's exact test for categorical variables as appropriate. Free text responses were parsed to establish key words and concepts provided by responders, which were later on made subject to logistic regression to identify possible differences between groups. Statistical significance threshold was set to a p-value of 0.05. All statistical computations were performed using STATA/MP 14.1 by StataCorp LLC (College Station, TX).
Results
The training program enlisted 1,380 professionals by the end of all sessions, consisting of 305 doctors, 383 nurses, 562 paramedics, and 130 fire department officers.
Response Aquisition
During the e-mail invitation process, 122 invalid e-mails (8.8%) were identified. As a result, only 1,258 professionals were successfully notified of their invitation to the study. The study links were accessed by 722 subjects and valid responses were obtained from 536 of them, averaging a 42.6% response rate.
Demographic Analysis
The responders were generally young, with a median age of 35 years (30–39 years old interquartile range). Male and female ratios differ significantly (p < 0.001) between doctors and nurses on one side, which are formed roughly of 2/5 males and 3/5 females, as opposed to paramedics and officers, where males make up more than 90% of these groups (Table 2).
Demographics of Study Respondents
IQR, interquartile range.
We observed a significant difference regarding the origin of professionals by the presence of a medical university and/or a county aeromedical service and/or dedicated disaster resources in the subject's county—hereinafter referring to such origins as High-Level Emergency Care Centers (HLECCs). Doctors (81.2%) and nurses (78.1%) came more frequently from such centers than paramedics (68.5%) and officers (45.1%) (p < 0.001).
Response Analysis
Given the differences in their training, when appropriate we will refer to doctors and nurses as an advanced medical care (AMC) group and to paramedics and fire department officers as a restricted medical care (RMC) group.
All professional groups reported on an electronic patient data documentation system already in use for their daily activities; however, AMC group subjects had a statistically significant higher ratio of its use compared with the RMC group subjects (p < 0.001). Age and gender were not identified as independent factors for either groups. However, HLECCs account for a significant difference between AMC and RMC groups (p < 0.001)—as shown in Figure 1.
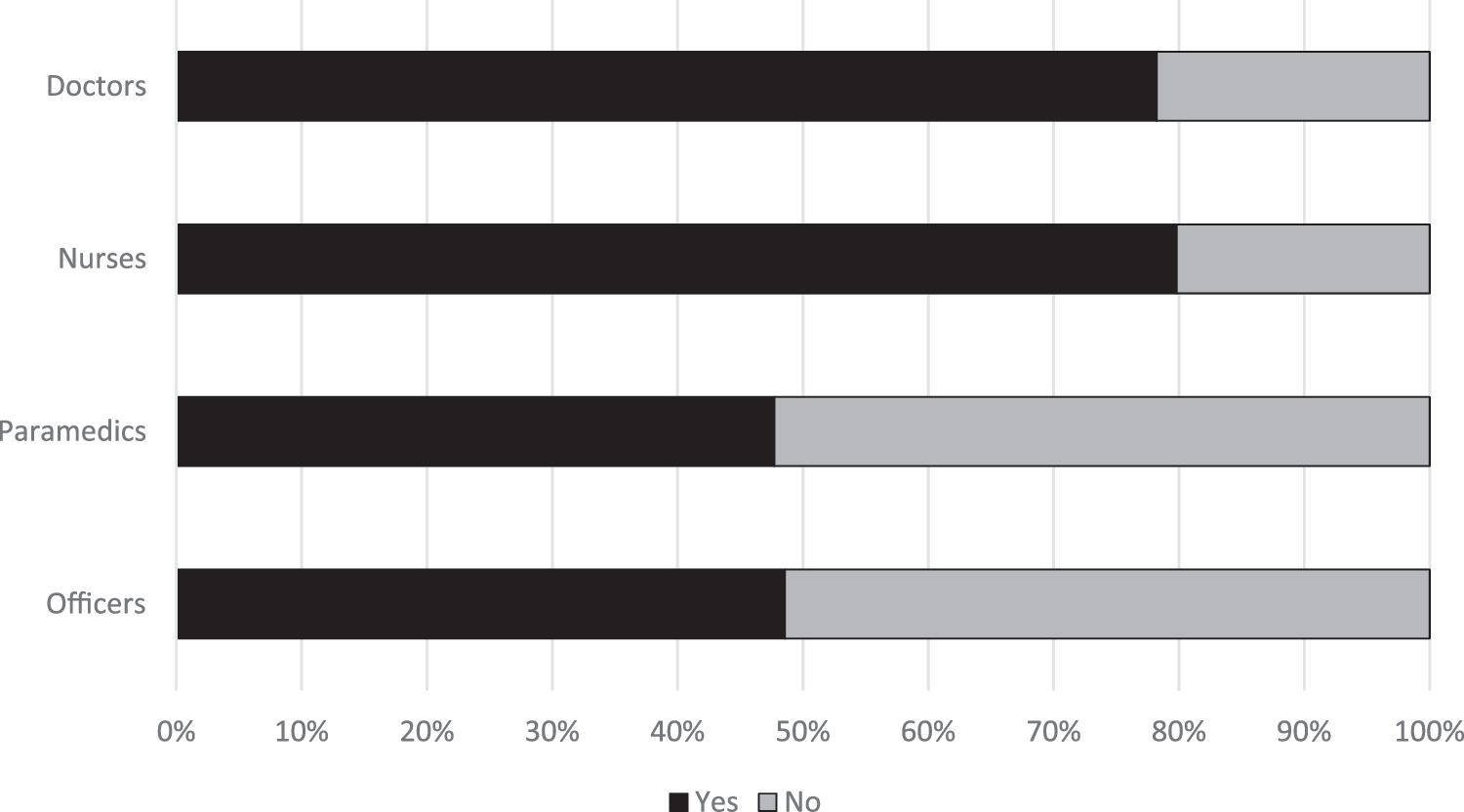
Current usage of an electronic data documentation system by survey groups.
Figure 2 illustrates the Likert item response distribution for the question regarding the hindering effect of responders' duties when required to use an electronic data documentation system. For the Likert item point range from 1 (no hindering) to 5 (extreme hindering), doctors scored a mean of 2.7 (95% confidence interval [CI] 2.5–3.0), nurses scored a mean of 2.3 (95% CI 2.1–2.6), paramedics had a mean of 1.8 (95% CI 1.6–2.0), and officers had a mean of 2.0 (95% CI 1.7–2.4), the differences being statistically significant (p < 0.001).
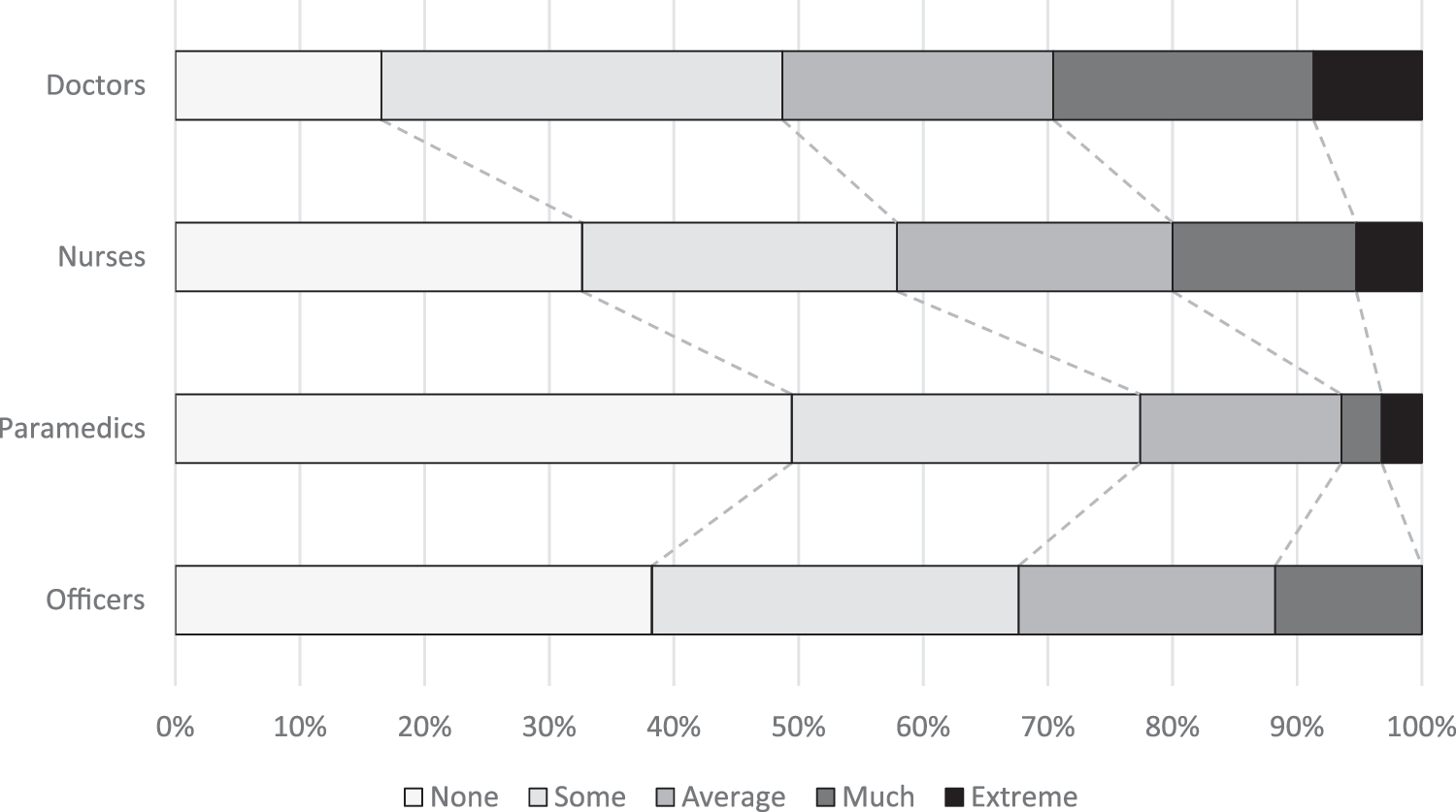
Hindering effect of current electronic solutions when required to use an electronic data documentation system by survey groups.
All respondents, independent of their professional roles, were found to be in favor of using an electronic solution for MCI-Ds should its employment be convenient, averaging a 94.1% agreement (95% CI 92.1–96.1%)—Figure 3. There is a significant shift toward less positive answers regarding its adoption as respondents report being hindered from their duties by current electronic solutions, with a drop from 100% to just over 60% (p < 0.001)—illustrated in Figure 4. Age and HLECCs did not account for any other significance; however, males are slightly more motivated than females (mean 96.3% vs. 89.9%, p = 0.003). Simulation versus real events experience had no impact upon any of the examined topics.

Willingness of using a convenient electronic data documentation system for MCI-Ds by survey groups. MCI-Ds, mass casualty incidents and disaster.
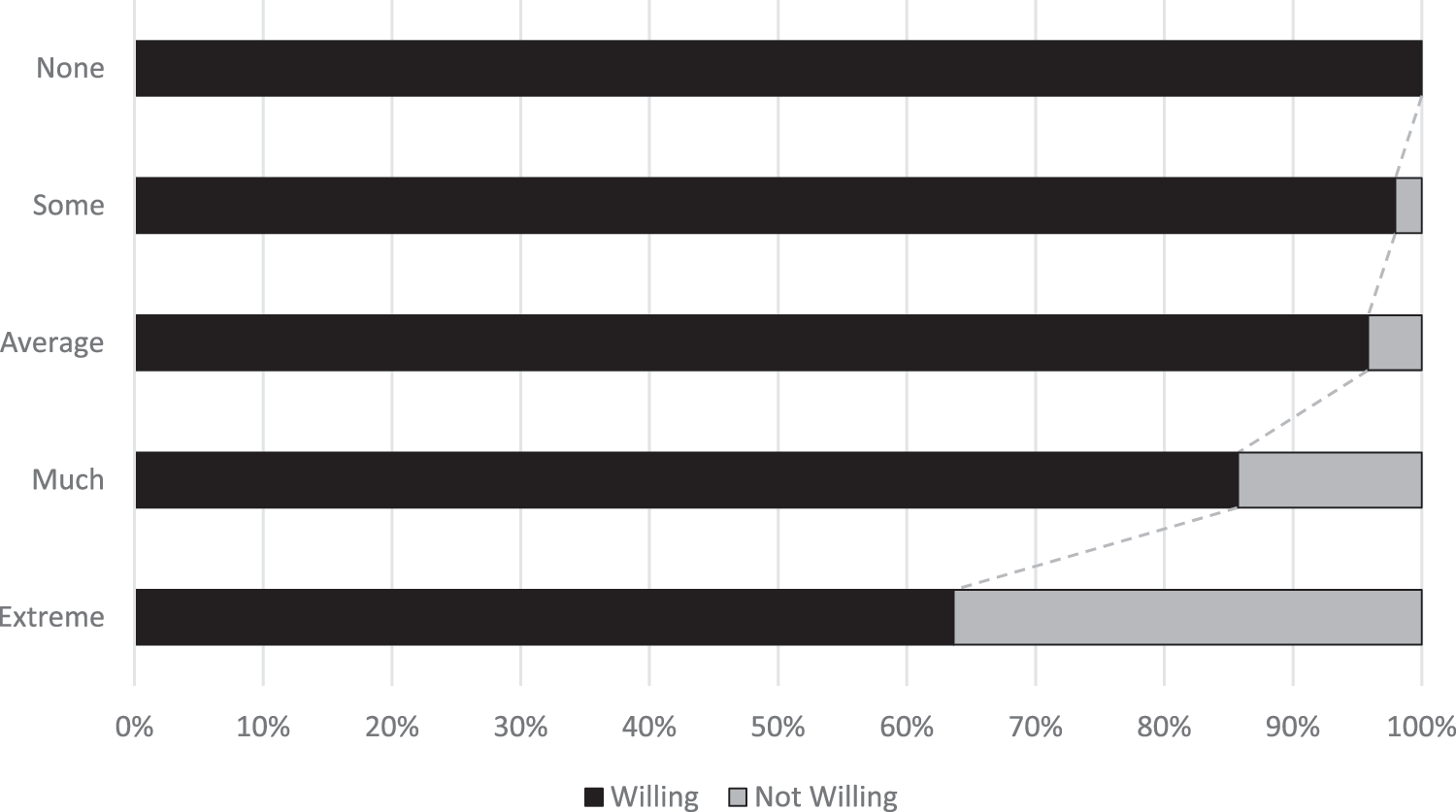
Hindering effect of current electronic solutions over willingness of using a convenient electronic data documentation system for MCI-Ds.
When questioned on the prospect of an exclusive electronic data documentation MCI-D solution, a large majority of respondents considered this would have a beneficial effect, with significant differences between AMC and RMC groups (p = 0.046) as depicted in Figure 5. Factors having a positive impact on respondents' opinion of an electronic data documentation MCI-D solution were the current use of electronic data documentation by doctors (p = 0.011), nurses (p = 0.042), officers (p = 0.028), but not paramedics (p = 0.476), and by males (p = 0.035), but not females (p = 0.074). It was also noted that the perception of being hindered by current electronic solutions inhibits the positive effect of an exclusive electronic solution for all professional categories (p < 0.001), except officers, as does withholding to use an electronic input system (p < 0.001).
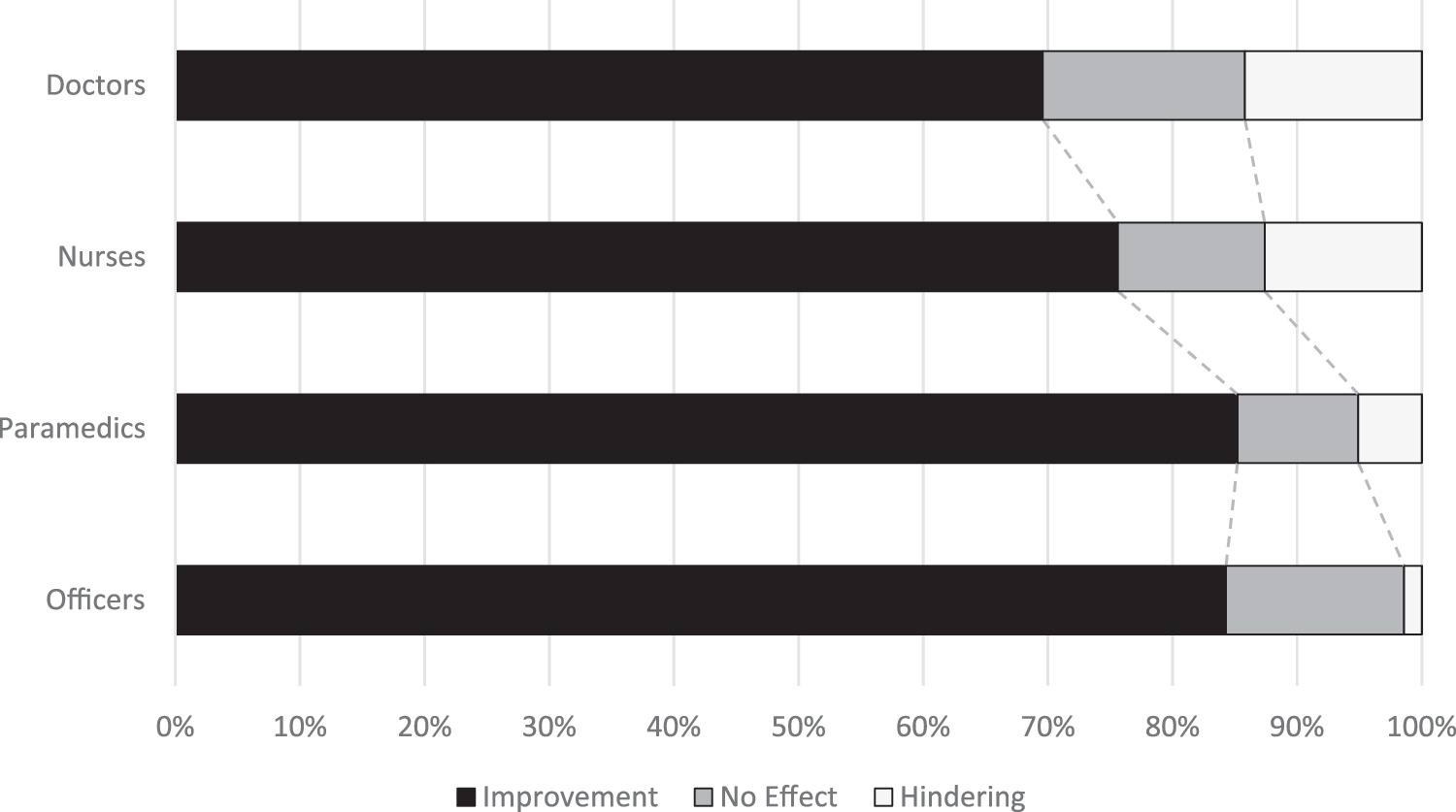
Perceived effect of using an exclusive data input solution for MCI-Ds over professional duties by survey groups.
Free Input Analysis
Free text input to express potentially useful technical and operative improvements of an MCI-D intervention was provided by 266 responders (71 doctors, 53 nurses, 101 paramedics, and 41 officers), averaging a 49.63% input rate while collecting 434 input elements.
The majority of collected elements were of operative nature, demonstrating strategies and indirect technical necessities, doubled later on by specific technical elements. Communication optimization under all of its aspects—employed technical devices as well as their applied operation—was the dominant topic (36.18% input rate) outlined by all groups, paramedics having a statistically significant lead on the subject relative to other responders (p = 0.007).
Detailed aspects of communication improvements were identified (in descending order of their average input rates): increased interagency communication flow (11.52%), optimized coordination within the same agency and improved dynamic command structure (7.14%), extended information regarding the event scene (13.23%), increased information/time density and real-time traffic (2.07%), role-centered filtered communication (1.84%), standardized communication procedures (1.38%), and enhanced knowledge of assigned resources whereabouts (0.69%). The remaining operative elements refer to the need of more frequent unannounced MCI-D simulations with realistic scenarios (5.76%), improved customization with MCI-D intervention procedures (5.76%), and the need to implement an objective debriefing solution (0.69%).
The most cited technical topic is the need for individually assigned communication devices—paramedics advocating the most once again (p = 0.013). The technical elements include (1) improved communication quality and decreased error rates (3.92%), (2) increased wireless carrier coverage (4.15%), (3) increased use of radio devices (2.3%), (4) individually assigned hands-free devices (2.07%), (5) the need for a dedicated radio frequency or data channel for the unfolding event (1.84%), (6) the deployment of an MCI-D integrated electronic system (0.69%), deployment of mobile devices (0.69%), (7) use of data and video broadcast features (1.38%), (8) use of interactive maps and GPS localization features (0.92%), (9) on site and in-traffic Internet access (0.23%), and (10) devices interoperability (0.23%). All input rates are homogeneous among responder groups, without statistically significant differences apart from the specified exceptions. All technical and operative input rates are illustrated in Figure 6.
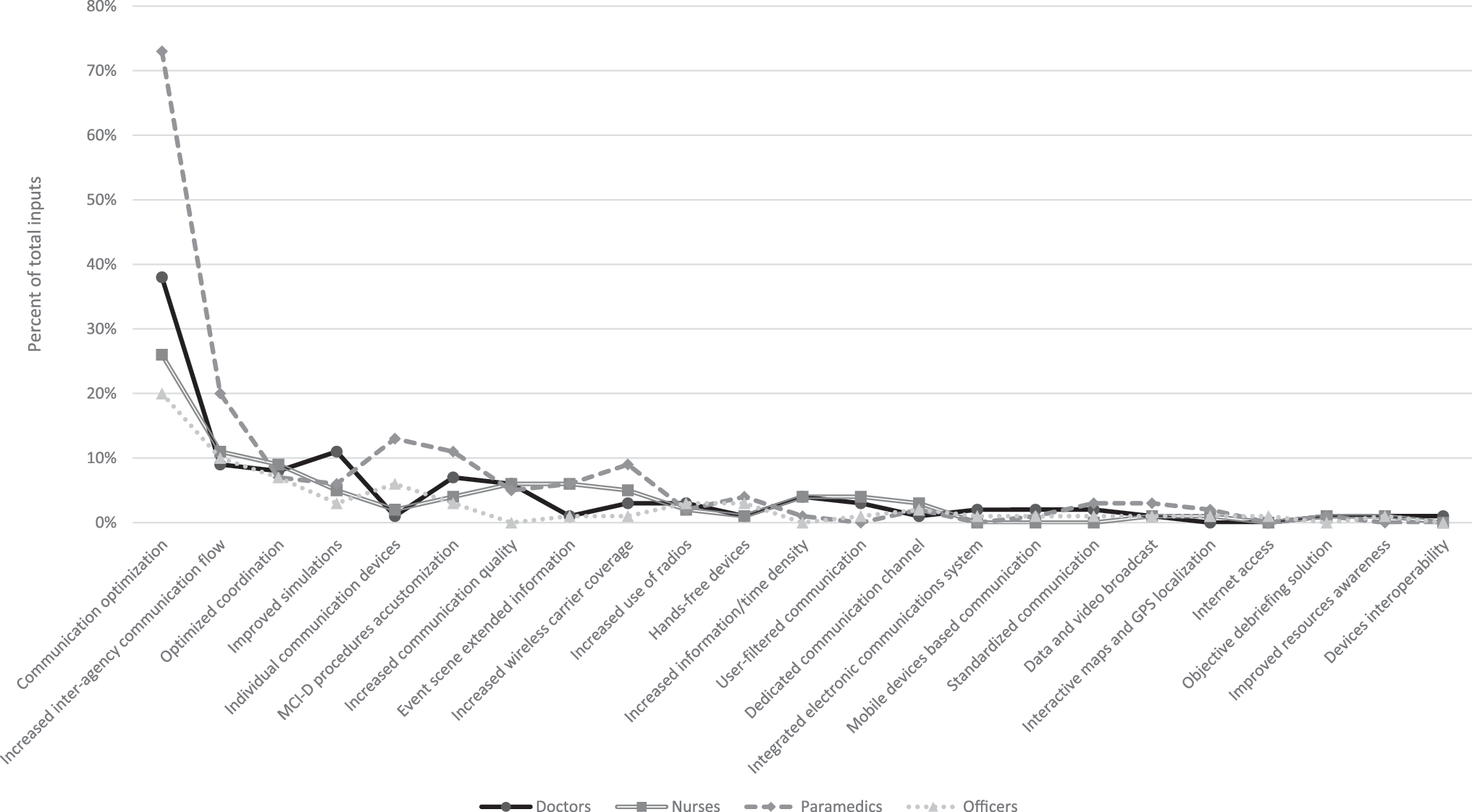
Input rates for the most useful technical and operative MCI-D improvements.
In the matter of medical data documentation, 522 input elements were obtained from 295 responders (86 doctors, 61 nurses, 108 paramedics, and 40 officers), averaging a 55.04% response rate.
The largest proportion of inputs pointed to an electronic medical data documentation solution with a highly significant 36.78% leading average input rate as opposed to an exclusive paper-based solution (2.3%) or to a dual electronic and paper-based solution (3.45%)—p < 0.001. For this last option, all but two elements were in favor of digitizing a previously handwritten medical chart versus a simultaneous paper and electronic documentation effort. The responder groups did not show any statistically significant differences among input rates (p = 0.176).
In functional terms, responders requested (in descending order of their average input rates): remote access to the patient medical history (12.45%) and dedicated staff for the documentation effort (4.21%)—where the AMC group had a significant higher demand than the RMC group (p < 0.001). In anticipation of future use of a dedicated electronic solution, responders asked for an easy-to-use application interface (4.79%), interagency software interfacing (4.6%), location-independent access to collected data (4.21%), real-time data visualization among all users (4.02%), MCI-D chart data fields essentialization (2.11%), standardized medical forms (1.92%), hospital prearrival medical data receival (1.53%), patient data and user access security (1.34%), documentation redundancies removal (1.15%), addition of visual, audio, and location data meta elements (0.77%), role-centered application interface (0.77%), and real-time event statistics (0.38%). The most requested technical element was the use of mobile devices (8.81%), doctors and paramedics having a significant higher demand than officers and nurses (p = 0.044). The remaining two technical elements included dedicated MCI-D software (3.07%) and patient bracelets with wireless (radio-frequency identification [RFID], near field communication [NFC]) and/or optical (barcode or quick response [QR] code) tags (1.34%). All input rates are also homogeneous among responder groups, without statistically significant differences apart from the specified exceptions. All medical data documentation solution input rates are illustrated in Figure 7. Controlling for age, gender, and HLECCs did not expose any independent factors for any free input topic.
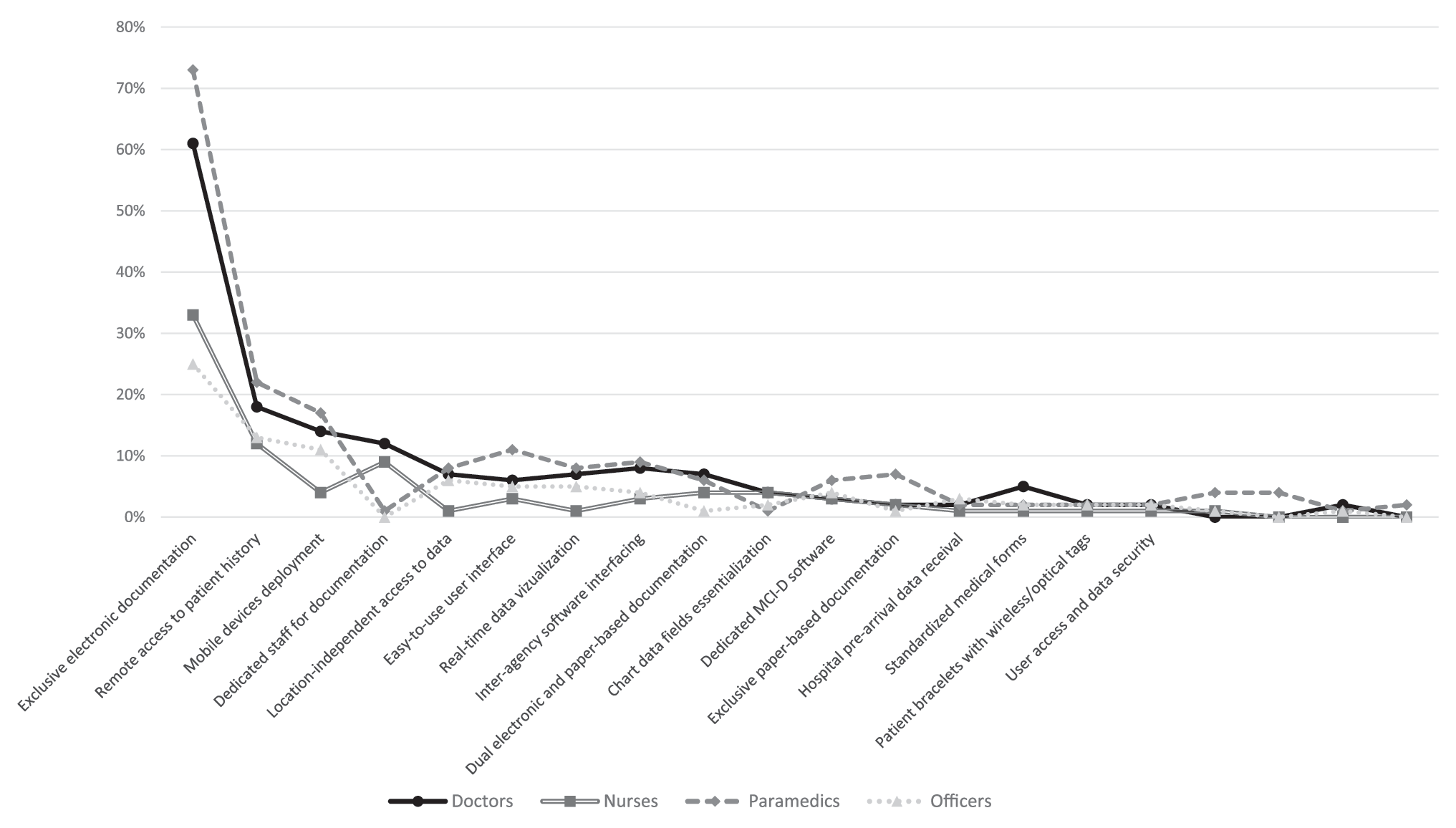
Input rates for MCI-D medical data documentation solutions.
Conclusions
The deployment of telemedicine during a mass casualty incident or disaster is a challenge, not only because of infrastructure constraints but also because the available solutions are still immature. 14,20
Even if rescue personnel are cited as not being an obstacle to implementation of telemedicine projects, 13 omitting user design input and user acceptance studies in favor of technical concerns can be pitfalls destined to negatively impact a project. To conceive a successful and sustainable MCI-D telemedicine project, 15 we started by querying professionals on their perception of current technology in use and then asked for specific improvements to establish a general model for the proposed future project.
Among limitations of the current study, we presumed that age is proportional to professional experience without specifically requesting this information. This may not always be the case, but we assumed those cases to be rare particularly considering that the study population is young and that changing professions is infrequent in Romania. We also chose not to suggest a list of elements to choose from as an alternative to free text input in an effort to encourage spontaneous input and to avoid social desirability bias. Evening out respondent proportions with larger professional population groups would ideally be preferable, especially given the relatively low input rates we obtained and which we attribute to sociocultural factors.
We observed that doctors and nurses are required to use some form of electronic medical data documentation more often than paramedics and officers, particularly if they originate from a HLECC. Higher medical expertise generally relates to a perceived increased negative effect of current electronic documentation solutions on professional duties. The magnitude of this effect is not negligible, demonstrating that the current setup does not act as a natural extension to the staff's medical duties. Not surprisingly, this leads to a significant drop in enthusiasm for the implementation of a proposed improved system.
It was generally conceded that enhanced communication and an exclusive electronic system for MCI-D data documentation could streamline staff's duties. Responders focused mostly on functionalities that may be supported by technology, sometimes exclusively, rather than pointing to detailed technical solutions, which may exceed their competence.
The ideal model centered on responders' feedback is an updated communication system based on modern devices, designed to facilitate rescue effort interactions, and teamwork while streamlining workflow, supporting a dynamic command hierarchy, delivering a larger amount of exact, reliable data taking advantage of available advanced technical features. In this regard, it must compensate for technical shortages like the absence of a wireless carrier signal. It must also be enabled for simulation and educational purposes. All of these requirements need to be available in an ergonomic user-friendly package. 21 The user interface has to be adapted to role requirements and demonstrate filtered data. To allow doctors and nurses to perform complex and urgent medical maneuvers, where possible, specially designated operators should provide data input into the system rather than the healthcare provider.
In setting up a project with the stated specifications it is vital to ensure organizational and technical integration into existing services. While pilot projects are critical, switching to mainstream operations is known to be far from straightforward. 9,22 This requires that, in addition to technical aspects and user-centered design, the implementers of the project have to plan and budget for user training, protocol development, technical support, a business model, and supporting policy and legislation. 14 While ensuring system resilience—as an exclusive state prerogative—is critical for MCI-Ds, the aforementioned complex requirements may set the need to externalize some of the above services to private contractors. Failure to ensure an overall coherent working system may lead to rescue intervention collapse, potentially aggravating an unfolding event. We thus consider there will always be a need for contingency plans.
Finally, we advocate for the development of a user-centered and user/task-customized telemedicine system for MCI-Ds. Although this may be difficult in some settings due to previously initiated projects, model design, and technical changes incurred later may not only increase expenditures, but also decrease user perceived usefulness and acceptance, posing a substantial risk to the overall success of the project.
Footnotes
Acknowledgments
This study was supported by SC Avant Maris Medical SRL and the University of Medicine and Pharmacy of Tîrgu Mureş—Research Grant No. 15897/10.11.2014.
Disclosure Statement
No competing financial interests exist.