
Abstract
Background:
Preliminary studies suggest the need of a global vision in academic reform, leading to education re-invention. This would include problem-based education using transversal topics, developing of thinking skills, social interaction, and information-processing skills. We aimed to develop a new educational model in health with modular components to be broadcast and applied as a tele-education course.
Materials and Methods:
We developed a systematic model based on a “Skills and Goals Matrix” to adapt scientific contents on fictional screenplays, three-dimensional (3D) computer graphics of the human body, and interactive documentaries. We selected 13 topics based on youth vulnerabilities in Brazil to be disseminated through a television show with 15 episodes. We developed scientific content for each theme, naturally inserting it into screenplays, together with 3D sequences and interactive documentaries. The modular structure was then adapted to a distance-learning course.
Results:
The television show was broadcast on national television for two consecutive years to an estimated audience of 30 million homes, and ever since on an Internet Protocol Television (IPTV) channel. It was also reorganized as a tele-education course for 2 years, reaching 1,180 subscriptions from all 27 Brazilian states, resulting in 240 graduates.
Conclusion:
Positive results indicate the feasibility, acceptability, and effectiveness of a model of modular entertainment audio-visual productions using health and education integrated concepts. This structure also allowed the model to be interconnected with other sources and applied as tele-education course, educating, informing, and stimulating the behavior change. Future works should reinforce this joint structure of telehealth, communication, and education.
Introduction
Teenagers of the 21st century have already been born and grown with interactive technologies, but are also usually exposed to many sensitive situations because of the difficult access to proper orientation. In Brazil, this is a common fact. Huge geographic distances, distinguished communities, and the difficulties met by schoolteachers to talk about sensitive themes increase ignorance and reduce interaction. According to public policies and official data from the Brazilian Ministries of Health and Education, this happens primarily with teenagers in priority topics related to sexuality, nutrition problems, and oral health. Therefore, we must rethink the traditional educational model to reach this public and encourage them to take effective actions.
According to Araújo, 1 education has been going through many transformations with the developments in science and technology in the past century. Therefore, the ongoing educational model became obsolete facing the modern world. Students are now able to learn through/and supported by technology, and teachers are no long the only source of knowledge for them.
Endrizzi 2 refers to Douglas Kellner about the need of a global vision in academic reform, with more space to communication, creativity, and applied skills. By these means, defining the student as an active and committed individual, overcoming the separatist vision of the students' cyber culture and the authoritarian model of teaching, was supported only by printed bibliographies. The Finnish educational system, which has been regarded as one of the best in the world, points toward this direction for at least 16 years. According to Symeonidis and Schwarz, 3 this happens because the world is changing around the school and, since the 2000s, the impact of globalization and the challenges for a sustainable future are increasing. Mattila and Silander 4 also argue that technology and internationalization pose new challenges to education. For developing focused on the future, thinking skills, social interaction, information processing skills, and skills in producing information play an important role.
Although the expression distance learning is well spread and consolidate, the Discipline of Telemedicine of the Pathology Department of the University of Sao Paulo—Medical School (FMUSP) have been developing new models for education supported by technology to raise the learning efficiency in conventional or distance learning. This research line is named Interactive Educational Technologies. 5 One highlighted area among educational technologies is the possibility to build interactive components to support teachers in the educational process, and the students' learning (e.g., the Virtual Human Project, a dynamic and direct communication method). It consists in a graphical portrayal of a huge amount of specialized information in a pleasant, interactive, dynamic, and objective way.
Morin 6 said that teaching an isolated subject weakens the mind's natural skill to process the knowledge. This quote comes straight toward the Virtual Human Project concept, a multidisciplinary joint work to develop new educational models in health. Moreover, according to Perrotti and Pieruccini, 7 we must break the traditional fragmentation in separated subjects that barely communicate to each other. The understanding of the teacher as the exclusively source of knowledge is vanishing and we must deal with this new reality. The new teacher must now be able to interact with the environment and understand the social and cultural background of the students. By these means, guide them to build their own understanding about different matters.
Many studies over new pedagogical architectures point toward a new educational model based on interactive educational technologies. Araújo 1 says that education professionals must understand and assume an academic and scientific position leading to education reinvention. According to him, the educational model set in the XIX century no longer supports the demands and needs of the modern society. He named it the fourth Educational Revolution, a model based on the problem-based education using transversal topics, and technics of the Human Centered Design Thinking.
Seeking to understand the nonformal education, Falk and Dierking 8 developed the free-choice learning concept. This is a voluntary process, nonsequential, respecting each person's pace, and through free choice, similar to what happens in museums, Internet, books, radio, and others. Therefore, the development of good educational programs in health must not be seen only through its scientific aspects. It must always seek the approach to practical experiences and encourage aspects that facilitate the learning. Then, we may say that all communication supports—audio visual, cognitive, interactive, and any other new development that stimulates the human senses—allow many uses to promote the experimental learning process in new educational models. All these combined with new technologies may create knowledge units to spread, propagate, and retain knowledge in many ways. That is why we developed audio-visual knowledge units in health as a resource to improve the understanding of complex topics, reinforcing the competence learning and measuring health education outcomes.
According to Grierson, 9 film producer who was an enthusiast of the pedagogical use of the films and the first to use the word documentary, the conventional educational process was no longer capable to teach by itself alone. For him, education should have overtaken the classrooms to meet the immediate needs of the society, therefore shaping new citizens with social responsibilities and more knowledge. Over 40 years later, we can see this applied in modern educational systems. Symeonidis and Schwarz 3 understand that competence is a key theme underpinning the mission and national goals of education in Finland. According to them, education is seen as “a precondition for personal growth, studying, work, and civic activity now and in the future.” The focus is particularly on transversal competences that cross the boundaries of individual subjects and aim to link different fields of knowledge and skills. They are entities consisting of knowledge, skills, values, attitudes, and will that can be applied in a given situation.
Based on these references, this study developed a system for a new educational model in health with modular components using scientific information to adapt fictional screenplays for educational broadcasts, and for interactive tele-education courses.
Materials and Methods
The use of multimedia resources to engage the target audience is a way to propose nonformal new educational models in health. Therefore, the development of a modular educational audio-visual TV show in health followed the following steps:
Development of Scientific Screenplays as the Central Core of the TV Show
The goal is to set the contents and main characters with an equivalent approach, also allowing consistent time intervals for each health condition.
• Each episode has a macrotopic that must appear as a microtopic in previous episodes;
• A macrotopic must appear at least twice or thrice before its main episode. In the same way, it must be mentioned once or twice after it (e.g., consequences and outcomes);
• Each episode has three to four microtopics.
We invited professors and clinical staff from the Medical School of the University of Sao Paulo, as well as Clinical Hospital, Odontology School, and Public Health School of the university to develop the scientific content.
Audio-Visual Adaptation
Working with the specialists the turning points in each topic were identified and these topics were highlighted in the screenplays. In other words, the key points in each condition and the moment to act were determined and the most relevant information was noted.
A “Skills and Goals Matrix” (Fig. 1) was developed to help this distribution and the development of support materials to the virtual environment. It is the evaluation of each topic using two criteria exposed on horizontal and vertical vertices. The vertical evaluation (1 to 9) is a weighting of each aspect's importance compared to another in the same topic (relative relevance). The horizontal evaluation is its weighting over the main topic. Therefore, we are able to identify the most relevant aspects in each topic and develop it in the fiction screenplays. It gave us the turning points and how to adapt the scientific content.
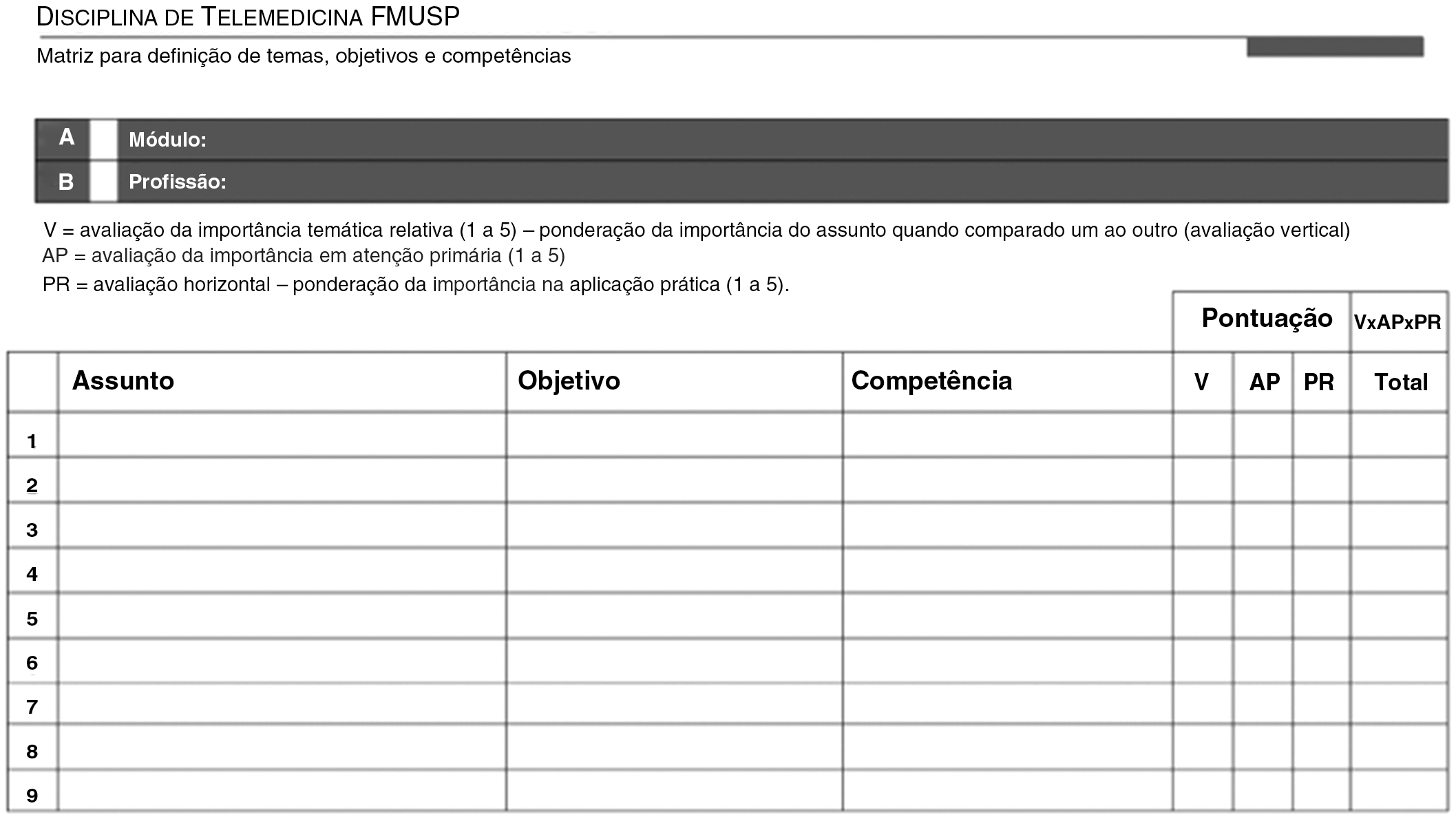
Skills and goals matrix.
Interactive Documentary
The proposed educational model intended to use fiction episodes together with debates and specialists' statements in each topic to stimulate the behavior change. The model should keep the youth atmosphere of the fiction episodes to avoid a hard break in style, what might generate noises in the learning process. The traditional interview model with Q&A was then substituted for a directed debate with actors, real-life characters, and specialists in health and education. The researcher wrote and directed the questions according to the topic and selected characters. It is important to guarantee that all the important information that resulted from the Skills and Goals Matrix was covered.
Specialist Statement
The specialist is shown in a nonformal style with the following script: • Analyze the scientific content of the episode; • Highlight the turning points and key aspects of each character; • Make a link with the real life and his personal experience.
Virtual Human Project
The development of three-dimensional (3D) sequences in computer graphics (CG) based on the “Virtual Human Project” is the result of an integrated work between scientific specialists, telemedicine specialists, and digital designers. Unlike traditional CG productions, the “Virtual Human Project” specifies and details each scientific aspect to produce an easier communication using dynamic 3D resources. We developed sequences for each of the themes focused and detailed in different scientific levels. Once again using the Skills and Goals Matrix, we had to guarantee that all the scientific information is covered by the sequences. The validation process with the responsible specialist must be done twice: first to set the animated sequences and second to validate the complementary subtitles. Moreover, all the scientific and physiological information must be covered.
Interactive Virtual Environment
We have developed a virtual educational platform based on the scientific contents of the show for evaluation and statistic study. The episodes and multimedia resources were disassembled and reorganized to fit an interactive tele-education course based on Moodle, an open source application for distance learning. Since each episode is made of 4 different multimedia segments, its modularity allowed different appliances. The structured course was developed to have 3 h of in-site activities, 27 h of distance learning, 13 h of distance activities, and 15 h of study. The total length of the course was 58 h in 2 months.
The contents were released after pretests of each topic and were made of educational videos, Web conferences, theoretical material, and common doubts vote, besides the final test. Each topic was released in 5 weekly modules with three topics each and the students were obligated to access the system in determined times for synchronized interactions (doubts voting and weekly Web confer). A team of six undergraduate medical students acted as group leaders to follow the students during the course. A specialist crew of professors, researchers, and clinical staff of the university tutored them.
Results
We developed a television show with 15 episodes made of fiction segments, interactive documentaries, specialists' statements, and learning objects about health in 3D CG. The target audience were teenagers from 15 to 20 years, and the topics were those of interest to the Brazilian Ministries of Health and Education.
Macrotopics Selection
Priority subjects to the Brazilians Ministries of Health and Education were based on young people vulnerabilities and related issues (e.g., high levels of early birth deaths were identified mainly in communities in need). However, this topic is not an isolated issue. It is first related to teenage pregnancy, what leads to contraceptive methods, sexually transmitted diseases (STD) prevention, and up to high levels of human immunodeficiency virus (HIV) infection. All topics covered by the study.
Criteria Selection of the Scientific Content
The creative team developed the story line, and the Educational Communication Design team adapted the fiction story according to the scientific content. The list is made of 13 topics because the first and the last episodes were used for opening and closure of the show, covering all subjects in a wide range. Therefore, the “Skills and Goals Matrix” indicated the following topics for each episode: (1) puberty, (2) obesity, (3) STD prevention, (4) bad breath, (5) anorexia, (6) food quality, (7) living with HIV, (8) teenage pregnancy, (9) oral health, (10) mouth cancer, (11) contraceptives, (12) STD early symptoms, and (13) human papilloma virus (HPV).
Screenplay Development
We set 12 workshops to write and develop the fiction screenplays. The length of these workshops was from 1 to 7 days according to the complexity of the topic. Each single issue was debated and validated by a specialist. When it was not possible to achieve an agreement in a workshop, the related topic had to be restared once again in a following meeting after several argues with the scientific team. This systematic approach was repeated until the final version of each screenplay.
Interactive Documentaries Development
The directed debate consisted in putting together real-life characters—people who faced the same problem of the episode—health specialists, actors who performed the main characters, and a mediator. The time length of the edited fragment varied from 3 to 4 min. We followed the recording for six consecutive days to guarantee that all the important topics were covered. Before each debate, the pre-edited fiction episode was screened to the participants. After that, the debate was guided to tease their emotions, invoking them to talk about personal experiences.
Specialist Statement
A 2 min statement was needed to validate the scientific content of the episode. The full-length interview was made available at the interactive virtual environment. We guided and directed each specialist during the interviews. Since some of the specialists were not involved in the previous scientific research, this was a first proof of the systematic model. Each specialist received a briefing of the project, watched the preedited fiction, debate segments and the suggested questions before the recording was made. They were allowed to suggest and/or adapt the questions, bringing their personal expertise to the topic.
Virtual Human Project
We have developed 13 animated sequences in 3D CG of the human body with 2-min each. The first episode has a compilation to introduce the project, and the last has no sequence. After the final cut, new meetings were made with the specialists to adapt to the scientific comments. These narratives were once again validated by the specialists, and then recorded and added to the 2-min sequences.
A Television Show Structure
Each episode has 26 min, allowing two 2-min breaks for a final length of 30 min. The episodes were then separated in three segments to fulfil the educational demands and achieve the experimental learning process according to Table 1.
Final Structure of the Episodes
3D, three dimensional; CG, computer graphics; DOC, documentary.
Broadcast
The television show Generation Health 2 was broadcast through TV Escola, the official channel of the Brazilian Ministry of Education. It was developed to be a national educational resource to support the basic education in public schools as part of the health in schools program. According to its official Web site, the channels are broadcast through satellite in open signal to about 15 to 20 million homes. It is also broadcast through cable TV, reaching a potential audience of another 18 million. Through a digital signal, it can be watched in smartphones and tablets with iOS and Android systems, besides being simultaneously broadcast in the channel Web site. In Brazil, about 50,000 public schools are able to receive the TV Escola programing.
The show was first broadcast from August to November 2010, for 15 consecutive weeks, on Mondays at 10 am Brazilian time (BRT) with a second broadcast at 2 pm BRT. After the broadcast, the episodes were available to download at the TV Escola Web site. The first broadcast reached third place on the audience score, and was the most requested TV show among teachers from public schools in 2010. It was rebroadcast at two other channels in 2011 and 2012. From 2013 on, it became part of the programing of the Health Channel—Internet Protocol Television of the University of Sao Paulo (IPTV USP). It is part of a health content programing based on prevention concepts, and is available in an online video server attached to a social network in health.
Young Doctor Project: Education and Health Promotion Trough Interactive Tele-Education 2014/2015
The show was then converted in an interactive tele-education course for two consecutive years as part of the Young Doctor Project in 2014 and 2015. Both editions had a huge demand among teachers and students from elementary and high school (75% of the 1,180 subscriptions). In addition, there were subscriptions from all 27 Brazilian states. In the end, at least one teacher or student was approved in the course in 20 different states, representing 73% of the graduations. The major periods of access to the system were at night and afternoon, with the peak time between 10 and 11 pm.
The courses also promoted training and education for medical undergraduate students who acted as group leaders. During the 2 months of the course, they created an instant message group that exchanged 560 messages, with 39% (217) of them during weekends. The peak times for the interactions were 1, 5, and 9 pm. On groups' management impact, the 31% of the subscribers who interacted with the group leaders represent 60% of the approvals.
Discussion
Positive results indicate the feasibility, acceptability, and effectiveness of a model of modular entertainment audio-visual productions using health and education integrated concepts. The use of 3D CG and interactive documentaries creates a reflection moment about each theme, immediately after the audience's emotional awareness of the anguish experienced by the characters. This is what we named experimental learning process.
Our aim was to deliver quality information, developing the learning process through daily life aspects to stimulate a behavior change. The division of each episode in 3 segments follows a logic model based on content versus time length (Table 2). We have seen that this planning increases the retaining process.
Logic Model Result
The developed model helps the student to overcome the virtual environment and apply the knowledge in his life and community. It builds audio-visual productions about health that are easy to understand. The modular structure creates many linking possibilities and increases the learning through complementary reinforcement.
The time length of each episode suits the television timetable and, simultaneously, fits the schools' classes' time length of 50 min. Therefore, the teacher may use the episodes to introduce a topic and carry out a debate in around 50% of extra time. In both cases, the model reaches sustainability and social education needs.
The study showed its acceptance and effectiveness on the audience scores of the first broadcast followed by continuous transmission in partners networks and IPTV channels. The modular structure also allowed the model to be interconnected with other sources and applied as a tele-education course, educating, informing, and stimulating the behavior change. According to previous studies' outcomes, the students were encouraged to share the acquired knowledge in their community, acting like leaders on the learning process about health issues. The peak times of access during the night period shows how the model also turns flexible the education and learning processes. The medical students' participation provided them a remarkable experience in peer learning, expanded learning, and understanding of medical and health issues. The amount of messages exchanged among them, especially in weekends and out of the school time, also reinforces the flexible learning aspect. Finally, their interaction with the groups proved to be determinant in the students' outcome, reinforcing the Pareto principle (aka 80/20 rule).
New technologies' resources help the independent learning, motivate education, and reinforce the peer learning. We focused on learning instead of teaching. We built knowledge through interaction. Future works should reinforce this joint structure of telehealth, communication, and education.
Footnotes
Acknowledgments
This study was partially supported by CAPES—Coordenação de Aperfeiçoamento de Pessoal de Nível Superior, and the TV show was sponsored and produced by the Brazilian Ministry of Education.
Disclosure Statement
No competing financial interests exist.