
Abstract
Background:
Rapid growth of three-dimensional (3D) printing in recent years has led to new applications of this technology across all medical fields. This review article presents a broad range of examples on how 3D printing is facilitating liver surgery, including models for preoperative planning, education, and simulation.
Materials and Methods:
We have performed an extensive search of the medical databases Ovid/MEDLINE and PubMed/EMBASE and screened articles fitting the scope of review, following previously established exclusion criteria. Articles deemed suitable were analyzed and data on the 3D-printed models—including both technical properties and desirable application—and their impact on clinical proceedings were extracted.
Results:
Fourteen articles, presenting unique utilizations of 3D models, were found suitable for data analysis. A great majority of articles (93%) discussed models used for preoperative planning and intraoperative guidance. PolyJet was the most common (43%) and, at the same time, most expensive 3D printing technology used in the development process. Many authors of reviewed articles reported that models were accurate (71%) and allowed them to understand patient's complex anatomy and its spatial relationships.
Conclusions:
Although the technology is still in its early stages, presented models are considered useful in preoperative planning and patient and student education. There are multiple factors limiting the use of 3D printing in everyday healthcare, the most important being high costs and the time-consuming process of development. Promising early results need to be verified in larger randomized trials, which will provide more statistically significant results.
Introduction
Ever since three-dimensional (3D) printing has become available to a broader audience with the growth of commercially available 3D printers and growing experience in this technology, multiple medical research centers have been discovering its potential. Surgery is an area especially focused on advancements in additive manufacturing, since 3D printing allows for the creation of precise anatomical models in a relatively simple manner.
Although 3D printing in the surgical field has thus far been dominated by maxillofacial and orthopedic surgery, 1 more subspecialties are discovering its benefits and present early promising developments in fields such as neurosurgery, 2 transplantation surgery, 3 pediatric cardiac surgery, 4 and anesthesia. 5 3D-printed models are being actively considered as a feasible tool in state-of-the-art surgical planning, 6 being an unique adjunct for complex procedures.
It is of note that the spectrum of 3D fabrication techniques is very broad. With each technique's strengths and weaknesses, it is difficult to find the optimal approach for each unique case. Thus, most articles describing applications of additive manufacturing in medicine focus on the technology itself, rather than on quantitative results and clinical outcomes.
Facing these barriers, liver surgery emerges as a suitable candidate for creating 3D-printed models. Complex surgeries such as living donor liver transplantations, minimally invasive procedures, and hepatic resections in oncological patients require exquisite knowledge of each patient's unique anatomy. 3D printing, as a potential alternative or adjunct to the standard medical imaging techniques of computed tomography (CT), magnetic resonance imaging (MRI), and 3D rendered visualizations, can provide a good representation of patient anatomy and tactile feedback.
Materials and Methods
We performed a literature search following the PRISMA guidelines 7 for pertinent articles using the scientific databases Ovid/EMBASE and PubMed/MEDLINE. Broad search terms were used to capture all potentially relevant articles. We included full-text articles and conference abstracts available in English. The search terms used were “3d printing,” “three-dimensional printing,” “additive manufacturing,” and “rapid prototyping” in combination with “liver” and “hepatic.” Our last search was conducted on February 1, 2017.
The results of our initial search were screened by two reviewers to identify relevant studies. Bioengineering and veterinary publications, nonbiomedical articles, duplicate publications, follow-up studies, and publications not pertaining to liver surgery or clinical practice were excluded from our review.
Extracted information included the following: type of implementation, image source, 3D printing technique, printing time, costs, reported accuracy of the model, and type of surgery performed, if applicable.
Results
Our initial search, following the search strategy described above, yielded a total of 297 articles (Fig. 1). After excluding 283 articles not fitting the criteria of our review, 14 articles were found suitable for data extraction (Table 1). Of the analyzed articles, the first was published in 2013. The number of publications in the area increased to two in 2014 and 2015 and increased to seven in 2016. The most common application for 3D printed models was the preoperative planning of complex procedures, such as living donor liver transplantation and liver resection (Table 2). One article described the development of models specifically for education purposes 14 —multiple models were created for teaching hepatic anatomy, including hepatic segments, to medical students. All liver models were created based on structures segmented from CT scans. In addition, some articles report MRI as feasible image source as well. 8,10,20

Flowchart of the search and screening process.
Short Descriptions of Three-Dimensional Printing Applications in Liver Surgery, Sorted by Ascending Year of Publication First and by First Author's Last Name Second
3D, three dimensional.
Grouped Parameters of Three-Dimensional Printing Applications in Reviewed Studies
Results are n (%).
CT, computed tomography; FDM, fused deposition modeling; MRI, magnetic resonance imaging; SLS, selective laser sintering.
The approach to creating 3D-printed models varied significantly in several aspects: the most popular fabrication method was the PolyJet/MultiJet technique, which was used to create models in 6 (43%) articles. Selective laser sintering (SLS) and fused deposition modeling (FDM) were utilized in four and two cases, respectively. Choice of technique had a major impact on the final model along with time and cost of printing. However, few authors described these details sufficiently for costs and printing times to be objectively compared. Costs began at $30 for low-quality models of hepatic vessels 18 to $4,000 for very complex, multimaterial liver models. 6 This was dependent on the following: type of fabrication, whether the labor costs were neglected, and cost of the 3D printer itself. Having said that, PolyJet is without a doubt the most expensive fabrication method (Fig. 2). Similarly, time of model creation is impossible to average and could be as long as 5 days for significant model finishing 9 or silicone casting. 21

Chart presenting prices of 3D models in reviewed articles by fabrication method. 3D, three dimensional; FDM, fused deposition modeling; SLS, selective laser sintering.
Quantitative analysis of the models' accuracy was performed in only one study, 14 which was deemed satisfactory. Ten other articles reported positive opinions and three did not discuss this issue at all. In addition, a study by Soon et al. showed that low-quality models are not accurate enough to plan surgery, but might be useful for educational purposes. 18
Discussion
Among the studies included in this review, only nine contained information regarding the approximate cost of developing 3D models. It should be noted that these costs are highly dependent on the type of printer (with PolyJet being the most expensive approach), material costs, complexity of the project, and the accuracy of the desired model and its assignment—medical education or preoperative training. Some authors suggested that despite the high costs of development, 3D printing incurs savings when the advantages are considered. We would like to highlight that scaling down 3D models 9,15 might reduce costs and is a valid option in some cases. However, its limitation is that the anatomy of a patient will not truly be reflected. Neglecting labor costs may be another problem in cost estimates. In contrast, it is usually difficult to estimate these expenditures, since several models are created in their entirety by physicians on personal 3D printers or by external companies as a promotional material. We suggest the standardization of future publications to detail time spent on specific parts of model development. Articles published in the future should distinguish costs of materials, labor, and the 3D printer used.
As was shown in the results of our study, fabrication methods vary widely (Fig. 3). Although PolyJet and SLS technologies allow relatively easy and quick print times, their availability is limited, and the costs of creating models on those machines can be several times higher than when using FDM. PolyJet undoubtedly provides great material property control and allows printing with multiple materials in a straightforward manner, but there have been some attempts to avoid its high costs with FDM. Those studies use materials such as jelly wax 14 or silicone to mimic PolyJet's transparent resins.
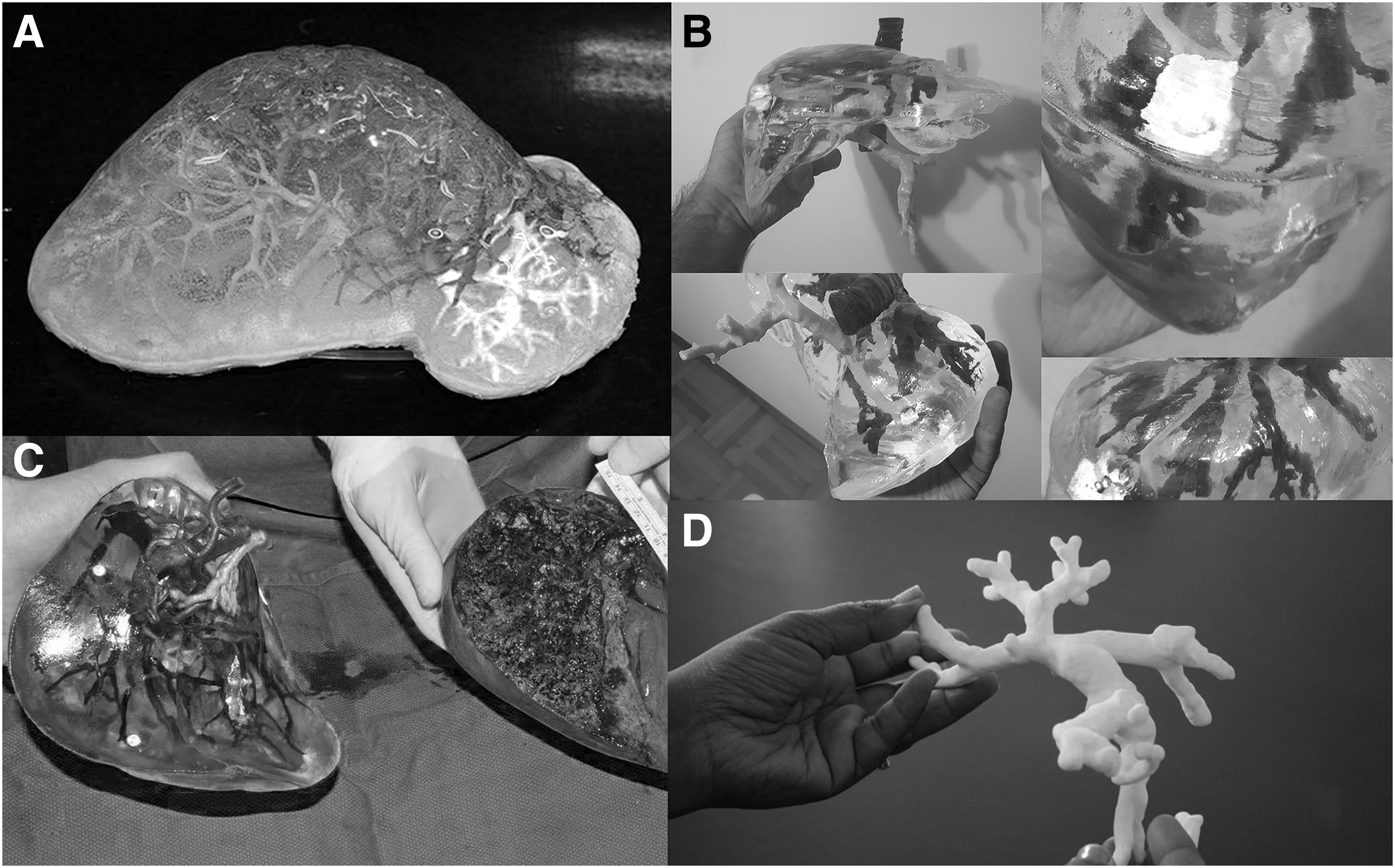
Liver models created with various fabrication techniques.
When using silicone to create 3D liver models, costs can be reduced significantly to $150, although this process requires more manual work in the finishing phase and is more time consuming due to long silicone curing times. 21
The widespread use of 3D modeling in surgery is also limited because many centers lack technicians with specialist knowledge in interpreting medical imaging. Medical 3D printing requires basic knowledge and skills in the following: anatomical structure segmentation (automatic, semiautomatic, or manual), virtual modeling, preparation for 3D printing, the printing process itself, and postprocessing. Thus, many surgical centers require help from not only radiologists but also specialist technicians in the early phases of their 3D printing research.
The authors of reviewed articles were in accordance that 3D modeling requires time, which limits the technique's usefulness in elective procedures. This period of model preparation will hopefully be shortened by the constant advancements in this field. Progressively shorter development times and better printing technologies are also likely to expand the use of 3D printing into other medical applications.
Undoubtedly, the lack of studies validating the accuracy of printed models to real anatomy is an issue for 3D printing in preoperative planning. Despite the lack of quantitative statistical validation, the authors of reviewed articles perceived the accuracy to be satisfactory. However, we concede that such analysis is difficult to undertake, since it can only be performed in select procedures, such as in living donor liver transplantation. 8
It is also worth noting that there have been no studies comparing the usefulness of virtually rendered models to 3D-printed ones. This is an issue with modeling in all surgical subspecialties, and although early reports suggest an edge for physical models, 22 even in comparison to immersive virtual reality, 23 further investigation is warranted.
Presented applications have focused primarily on surgical planning and intraoperative guidance. Other emerging and exciting applications include patient and trainee education. A study by Kong et al. 14 has proven that 3D-printed models are a feasible teaching aid for teaching complex anatomical concepts to medical students, such as hepatic segments. Other reports also suggest using these models to teach surgical trainees 18 anatomy or for surgical simulation. 19
Conclusions
Early publications exploring of 3D printing in liver surgery suggest that further study into this technology is warranted. It has yet to be established if 3D printing offers any improvement to clinical outcomes; in order for further growth in this field to occur, case reports need to give way to large-scale randomized controlled trials. Recent reports showing low-cost methods for creating liver models 21 should accelerate the adoption of 3D printing by smaller surgical centers, and with ongoing advancements in technology, major costs and time reductions are forthcoming.
The utility of 3D printed models for patient and student education has yet to receive much attention in the field of liver surgery, but could prove beneficial to the therapeutic relationship when counseling patients. 23
We suggest evaluating the utility of 3D models in all facets of surgical practice; from educating patients before the procedure, as a preoperative and intraoperative tool, and using those same models for medical education. It is our hope that this holistic approach of integrating 3D models into patient care will result in this promising new technology becoming adopted by more surgeons in their everyday practice.
Footnotes
Disclosure Statement
No competing financial interests exist.