
Abstract
Background:
Mobile phone messaging software robots allow clinicians and healthcare systems to communicate with patients without the need for human intervention. The purpose of this study was to (1) describe a method for communicating with patients postoperatively outside of the traditional healthcare setting by utilizing an automated software and mobile phone messaging platform and to (2) evaluate the first week of postoperative pain and opioid use after common ambulatory hand surgery procedures.
Materials and Methods:
The investigation was a prospective, multicenter investigation of patient-reported pain and opioid usage after ambulatory hand surgery. Inclusion criteria included any adult with a mobile phone capable of text messaging, who was undergoing a common ambulatory hand surgical procedure at one of three tertiary care institutions. Participants received daily, automated text messages inquiring about their pain level and how many tablets of prescription pain medication they had taken in the past 24 h. Initial 1-week response rate was assessed and compared between different patient demographics. Patient-reported pain and opioid use were also quantified for the first postoperative week. Statistical significance was set as p < 0.05.
Results:
Forty-seven (n = 47) patients were enrolled in this investigation. Total response rate of both pain and opioid medication questions through 7 days was 88.3%. Pain trended down on a daily basis for the first postoperative week, with the highest levels of pain being reported in the first 48 h after surgery. Patients reported an average use of 15.9 ± 14.8 tablets of prescription opioid pain medication.
Conclusions:
We find that a mobile phone messaging software robot allows for effective data collection of postoperative pain and pain medication use. Patients undergoing common ambulatory hand procedures utilized an average of 16 tablets of opioid medication in the first postoperative week.
Introduction
There is an increasing pressure in the healthcare landscape to care for patients in the most efficient and cost-effective manner. Traditionally, communicating with patients during the postoperative period has involved multiple clinic visits, which represent a time and monetary cost to patients and providers. Authors have also considered utilization of traditional “telehealth” programs 1 –3 that largely consist of patients and providers interacting through a telephone conversation, video feed, or e-mail exchange. Although these solutions allow a patient to be cared for outside of the traditional healthcare setting, they are still resource intensive with need for appropriate medical staffing and potentially expensive technology setups for both patients and providers. We also recognize a growing shortage of research funding 4 and associated pressures to obtain important patient data in effective ways at the lowest possible costs to researchers and healthcare systems. Automated mobile phone messaging robots present the opportunity to communicate with patients using a widely accepted means of communication on devices that patients already own. 5 –11 Software messaging robots allow for the automated delivery of predefined questions, reminders, and instructions to patients through mobile phone messaging interfaces 6 –9 without the need for human intervention.
Opioid use has reached epidemic levels 12,13 and is of concern to orthopedic surgeons. 14 Increased opioid use has previously been found to lead to worse clinical outcomes and increased subsequent opioid use in various orthopedic patient populations. 15 –17 In addition, previous authors have reported that 30–40% of patients will experience an acute 24–48 h history of elevated pain that interferes with sleep and daily activities after outpatient surgical procedures. 18 The current medical literature does not accurately describe the typical postoperative pain course and use of opioid medication after ambulatory orthopedic hand surgery. In our experience with ambulatory hand procedures, opioid medication is, at times, overprescribed, likely because of the lack of data on pain and pain medication requirements after these procedures.
Further inquiry into how healthcare systems can communicate with patients postoperatively outside of the hospital setting may allow for effective communication while decreasing cost and utilization of healthcare resources. In addition, understanding the postoperative course of pain and opioid demand after common hand surgery procedures would be valuable in counseling patients 19 and in providing appropriate amounts of prescription pain medication. This investigation aimed to (1) describe a method for communicating with patients postoperatively outside of the traditional healthcare setting by utilizing an automated software and mobile phone messaging platform and to (2) evaluate the first week of postoperative pain and opioid use after common ambulatory hand procedures.
Materials and Methods
The investigation was a prospective, multicenter investigation of pain and opioid usage after ambulatory hand surgery. In this investigation, we sought to evaluate the feasibility of monitoring pain and opioid usage with an automated mobile phone messaging platform. Patients presenting to one of three (Iowa, Minnesota, University of Pennsylvania) hand and upper extremity clinics were approached for this study. Inclusion criteria included any adult (≥18 years old) with a mobile phone capable of text messaging, who was undergoing a single common ambulatory hand surgical procedure at a participating institution (carpal tunnel release, ulnar nerve decompression or subcutaneous transposition, trigger finger release, ganglion cyst excision, or open reduction internal fixation for distal radius fracture). Exclusion criteria included chronic opioid use. Patients signed informed consent after thorough explanation of the software and communication protocol involved in the study. Patients were not compensated for this study. Patients participating in the study were required to fill out a demographic questionnaire that assessed sex, age, level of educational attainment, work status, mobile phone type/carrier, smoking status, and presence of diabetes. No demonstration of the software was performed during the consent process; patients were simply told they would start receiving mobile phone messages inquiring about their level of pain and opioid use after surgery.
Data collection began on the day of surgery, termed postoperative day (POD) 0. The participants received an initial text message on the evening of POD 0 inquiring about pain level (0–10) and a subsequent text message asking how many tablets of prescription pain medication had been taken in the past 24 h (Fig. 1). On POD 1–POD 3, individuals received three pain inquiries throughout the course of their day (morning, noon, and evening) and a once daily prescription pain medication inquiry (evening). On POD 4–POD 6, individuals received a daily pain and prescription pain medication inquiry (evening).
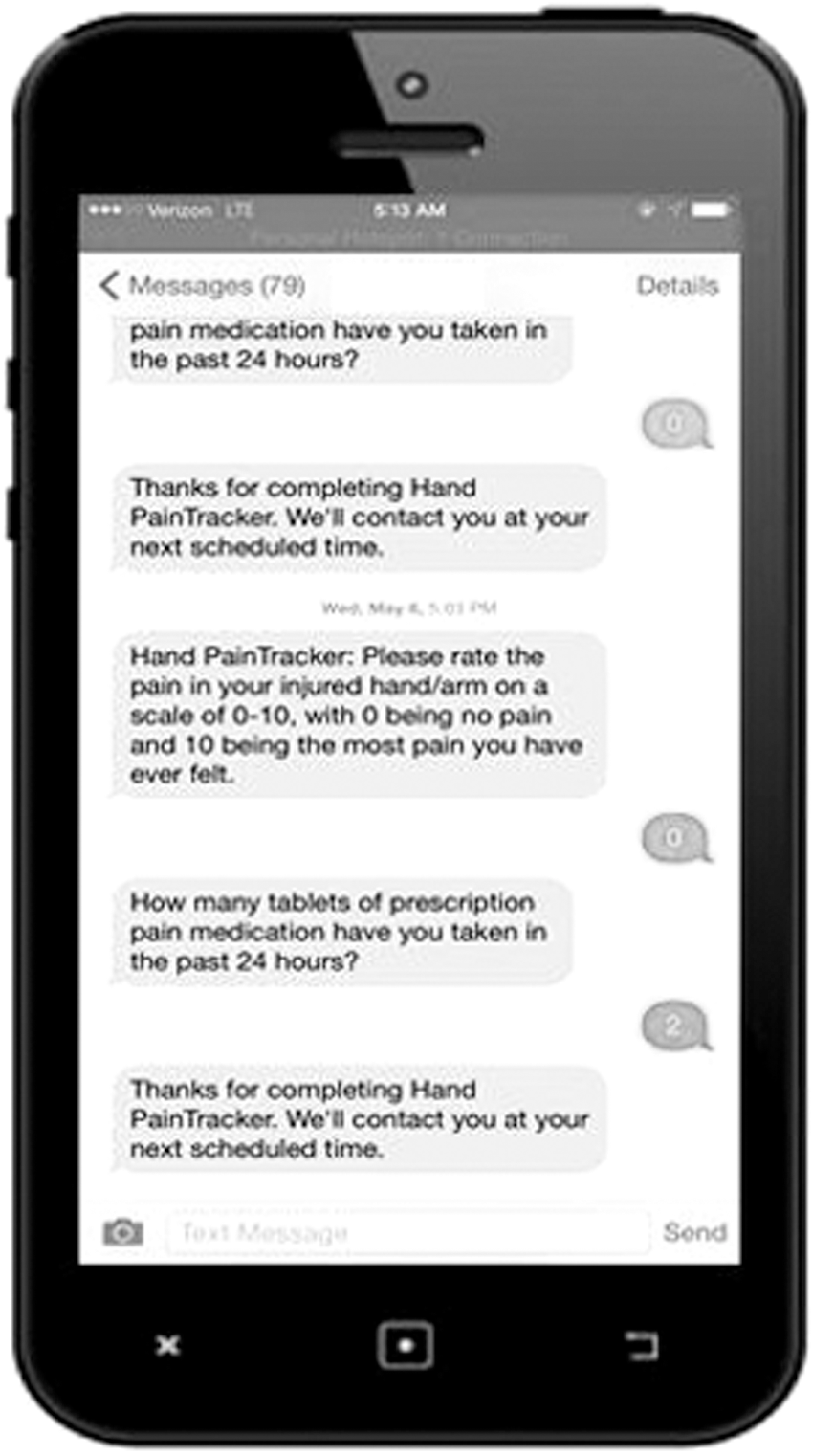
Example of mobile phone interface and questions/responses in this study.
We utilized a simple software algorithm for this study (Fig. 1). Server side, time-based automated software scripts were utilized to access hypertext preprocessing (PHP) scripts at appropriate time intervals. The associated PHP scripts would subsequently send the appropriate text communication to patients. If a patient responded to the initial evening pain question, a subsequent follow-up opioid usage inquiry would be immediately sent by the software (Fig. 1). All patient responses were stripped and parsed by the software and inserted into a secure database. If patients attempted to communicate with the software at an inappropriate time, the software would alert the patients that it would contact them at their next scheduled time. If a patient who was not enrolled in the study attempted to communicate with the software, the software would communicate with the patient that he or she was not currently enrolled to receive communication and provide study coordinator contact information for further communication needs.
Initial 1-week response rate was assessed and compared between different cohort demographics. Characteristics of participants were compared using Student's t test for continuous variables and chi-square or exact tests for categorical variables. Statistical significance was set as p < 0.05. To detect a 10% increase or decrease in overall response rate to all questions with 80% power, 10 patients were required per group (p < 0.05). Statistical analyses were performed using Microsoft Excel (Microsoft Corp., Redmond, WA). This investigation was approved by the Institutional Review Board at the University of Iowa, University of Pennsylvania, and HealthPartners/Regions Hospital, and was deemed compliant with the Health Insurance Portability and Accountability Act.
Results
Forty-seven patients (n = 47) were enrolled in this study with 45 being considered in the final analysis; 2 patients who were enrolled at their preoperative visit subsequently decided on their day of surgery that they did not want to participate. Average patient age was 49.6 ± 13.7 years (range 20–70)—69% were female, 40% had completed college, and 64% were working.
Total response rate of both pain and opioid medication questions through 7 days was 88.3%. Completion rate for pain questions was 90.1% and completion rate for prescription pain medication questions was 85.1%. Female participants responded at a higher rate (92%) than males (79%, p = 0.01). There were no differences in completion rate between those who had completed college and those with less than a college degree ( = 0.44) or between those who were working and those who were not (p = 0.73). There were no differences in completion rate by age group between those >40 years and those of age ≤40 years (p = 0.10) (Table 1).
Completion Rate of Both Pain and Opioid Medication Questions by Patient Age for the First Postoperative Week After Ambulatory Hand Surgery in 45 Patients
Pain trended down on a daily basis for the first postoperative week for all procedure groups (Fig. 2). Average pain on POD 0 (4.59 ± 2.9) was different from average reported pain on POD 6 (2.35 ± 2.62; p < 0.005). Patients undergoing carpal tunnel release, trigger finger release, and ganglion cyst removal had the lowest reported pain after 48 h from surgical intervention (Fig. 3). During the 1-week study period, patients reported an average use of 15.9 ± 14.8 tablets of prescription pain medication. Average reported use of prescribed pain medication for the first postoperative week was 36% of patient's prescribed amount for that week (Table 2).
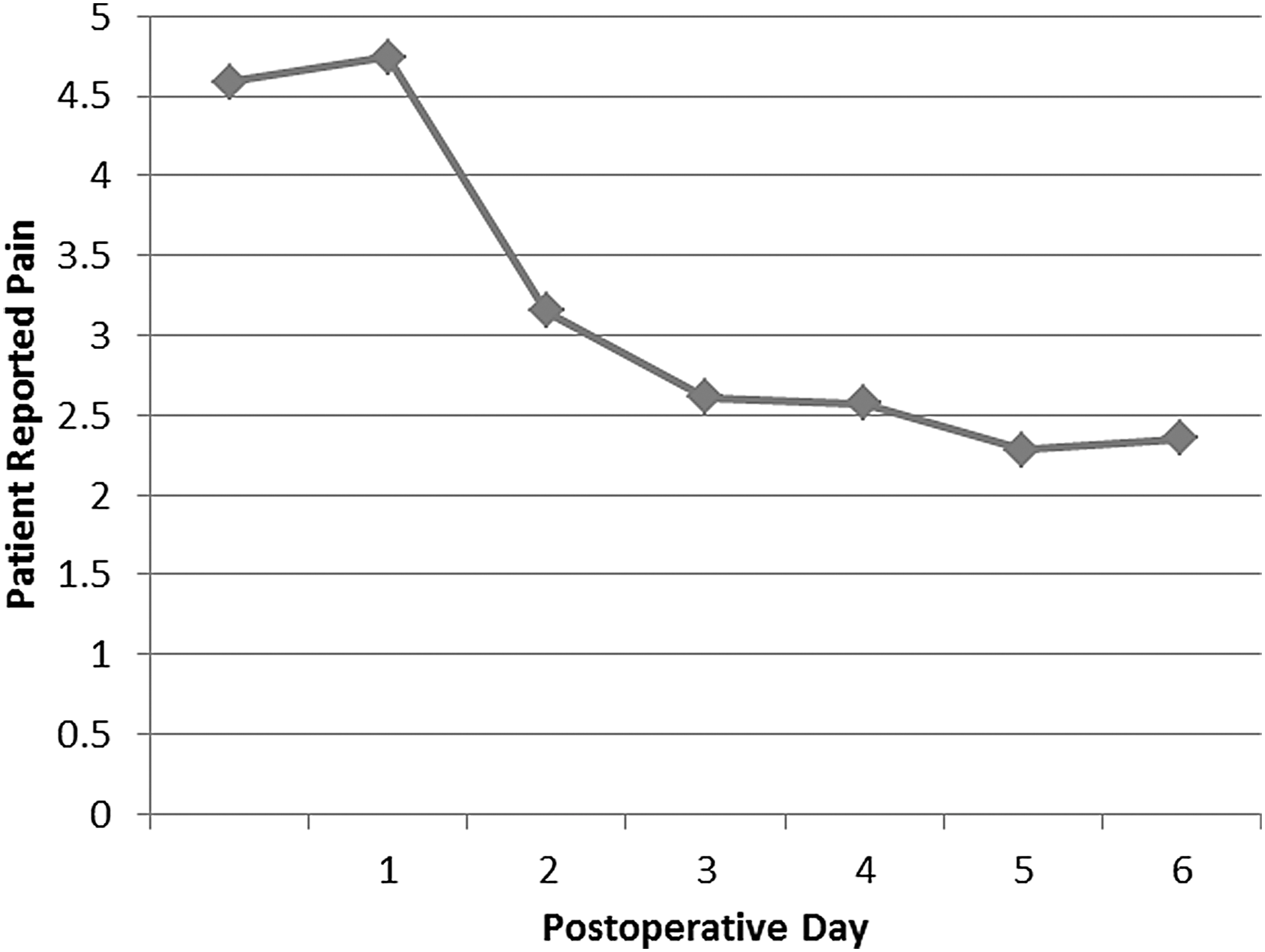
Average pain by day for the first postoperative week for 45 patients undergoing ambulatory hand surgery.
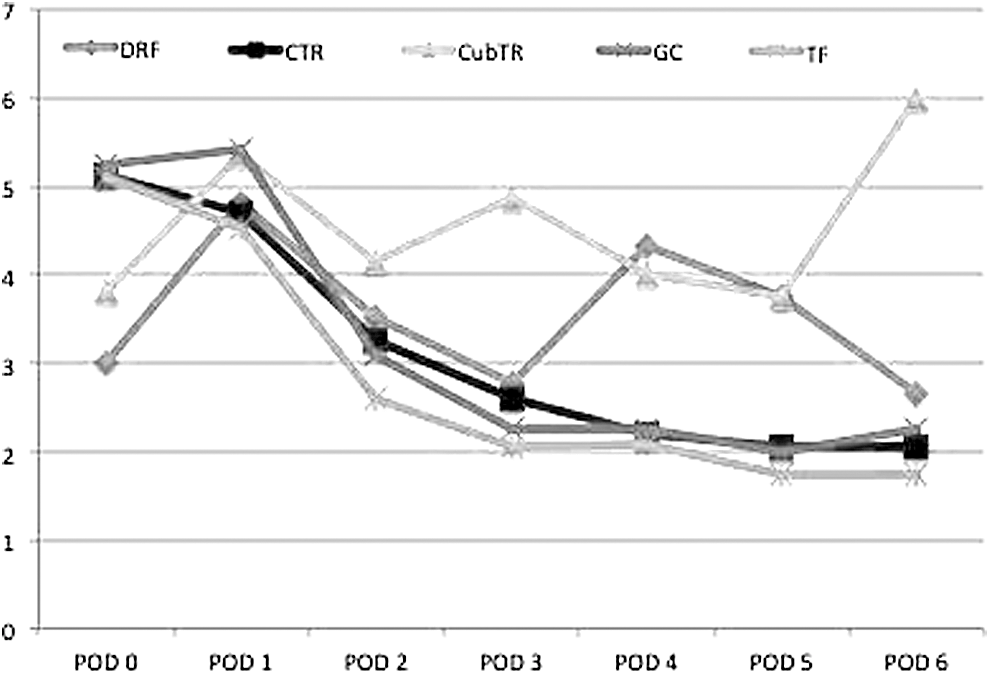
Average pain by surgical procedure for the first postoperative week after ambulatory hand surgery in 45 patients. DRF, distal radius fracture fixation; CTR, carpal tunnel release; CubTR, cubital tunnel release; GC, ganglion cyst removal; TF, trigger finger release.
Breakdown of Patient-Reported Opioid Use by Surgical Procedure During the First Postoperative Week After Ambulatory Hand Surgery in 45 Patients
Discussion
Postoperative communication between patients and providers typically occurs in person in a clinic or over the phone. This type of communication can be time consuming for patients and provider organizations, and is an intensive use of human resources. Use of automated software to communicate with patients outside of the healthcare setting may have advantages compared with traditional communication models. We report our experience and describe our method of software-driven mobile phone communication through an automated messaging robot during the acute postoperative period. We also report data on pain and opioid usage from adult patients undergoing common ambulatory hand procedures at the participating institutions. We find that patients had a high response rate of questions delivered by the automated software messaging to their mobile phones. We also report that patients utilized only a small percentage of the prescribed opioid medication during the first week after surgery, suggesting an opportunity to curtail opioid overprescription.
Communication with automated software messaging robots presents the opportunity for healthcare providers to communicate with patients in an ongoing and continuous manner without the need for extensive use of healthcare resources. 7,8 This form of human–computer interaction has become prevalent in cultures around the world and takes the form of text messages, 5 instant messaging (e.g., Facebook Messenger), 10 and “apps” with messaging interfaces (e.g., WhatsApp). 11 We report an average response rate of nearly 90% by utilizing our described automated messaging platform. Other than a difference between genders, we find no differences in response rate by various patient demographics, including patient age and educational attainment. Our findings suggest that the automated software communication utilizing mobile phone messaging robots is an effective way to communicate with a broad range of patients in the postoperative period. We recommend that mobile phone messaging robots are a cross-platform/device communication interface that have a high likelihood of success when attempting to communicate with patients. The communication algorithm utilized in our study was relatively simple, and we call for further investigation in software communication with patients by utilizing more extensive “conversational” algorithms.
There is currently an opioid use epidemic in the United States. 12,13 We find no previous work that attempts to quantify the acute postoperative course of pain and opioid medication use in patients undergoing common hand procedures. We provide patient-reported pain and opioid use data from the first postoperative week in a cohort of patients who underwent common outpatient hand procedures. We report a precipitous drop in patient-reported pain after the first 24–48 h, which is consistent with previous reports (Fig. 2). Our initial findings suggest that patients undergoing common hand procedures may require a relatively small amount of opioid medication (Table 2). Surgeons should be advised that pain medication requirements during the first week after common outpatient hand procedures likely do not exceed 20 tablets of opioid medication. Patients in this study utilized just more than one-third of their prescribed opioid medication during the first postoperative week, suggesting an opportunity to decrease prescription quantities and reduce opioid diversion. Further inquiry in a larger patient cohort with longer follow-up is warranted to understand postoperative pain patterns and opioid usage after ambulatory hand surgery. We aim to investigate a larger patient cohort for an extended period of time to this end.
Automated software communication platforms are not free; there are multiple factors that comprise the overall cost of these modern communication tools. The software design and build process, ongoing software maintenance, computer servers, and appropriate security comprise the total cost picture when considering software platforms that communicate with patients. Although a detailed analysis of these factors is outside the scope of this work, we do recognize that the costs to produce and maintain software as well as store data continue to experience a precipitous decrease in price. In this study, the actual delivery of messages through our software application was of minimal cost at $0.01 for every message sent and received. 20 Our approach also eliminated the need for human intervention in the data gathering process as well as common associated costs. The cost of employing staff members to obtain postoperative data is immense at our institution and we feel that this study serves as an example of how mobile phone messaging platforms can be built that may alleviate this cost. We recommend a detailed cost analysis/modeling of automated mobile phone messaging platforms.
This study should be considered in light of several limitations. Follow-up was limited in this study to 1 week. Certainly, longer follow-up is warranted. We also acknowledge that generalization of our relatively small study cohort to a larger and more diverse patient population may not be appropriate. We suggest a larger patient cohort is necessary to draw more definitive conclusions on both the presented technology platform and postoperative pain and medication use after common hand procedures. In addition, our pain question did not ask patients to differentiate between pain they were having currently versus average pain for the past 24 h (Fig. 1). We acknowledge this could potentially have been a point of confusion for patients. We also recognize that the technology platform presented in this study may not be preferred or optimal for all patients. In addition, we did not assess the type of messaging/data plan each patient had and we acknowledge that interaction with our platform may have been influenced by this factor. Further inquiry into appropriate patient populations and use case scenarios will be critical if automated software communication with various patient populations and demographics is to be successful. Hand dominance was also not assessed and may provide a useful data point in further related work. Finally, we acknowledge that pain and opioid use may have, in part, been influenced by different postoperative provider-specific recovery and rehabilitation protocols. Our lack of standardization of the postoperative course in this multiinstitutional study may potentially skew our reported pain and opioid profiles. We also recognize the opportunity to perform interventional automated software messaging in appropriate circumstances that might help to reduce patient opioid use among other problems.
Conclusions
Automated software mobile phone messaging robots allow surgeons and healthcare systems to obtain data during the postoperative period with limited human intervention and nominal expense. We recommend further inquiry in this area with more extensive development and validation of software messaging robots in orthopedic and general healthcare-related contexts. In patients undergoing common ambulatory hand procedures, an average of 16 tablets of opioid pain medication were utilized in the first postoperative week, which represents 36% of the prescribed pain medication for the first postoperative week. We recommend further inquiry regarding postoperative opioid use in patients undergoing hand procedures to reduce overprescription of opioids and diversion. We also recommend that surgeons and healthcare systems consider our initial data when determining patient-specific postoperative opioid requirements.
Footnotes
Acknowledgments
Each author certifies that he or she, or a member of his or her immediate family, has no funding or commercial associations (e.g., consultancies, stock ownership, equity interest, and patent/licensing arrangements) that might pose a conflict of interest in connection with the submitted article. Each author certifies that his or her institution approved or waived approval for the human protocol for this investigation and that all investigations were conducted in conformity with ethical principles of research.
Disclosure Statement
No competing financial interests exist.