
Abstract
Background:
Health information technology (HIT) interventions developed to support patients' self-care for chronic diseases have become popular, but people may not always accept and sustain their use.
Introduction:
This study examined factors that affected patients' acceptance of a computer-based, chronic disease self-monitoring system over a 4-week period.
Materials and Methods:
A research model was developed to test the relationships between the perceived usefulness, perceived ease of use, attitude, and subjective norm and the patients' behavioral intention to use the system (i.e., acceptance). Data were collected with surveys of 42 patients with type 2 diabetes mellitus and/or hypertension at baseline, 2 weeks after implementation, and 4 weeks after implementation. Path analysis was used for model testing.
Results:
Perceived usefulness affected behavioral intention indirectly at 2 weeks and directly at 4 weeks; perceived ease of use affected behavioral intention indirectly at 2 and 4 weeks; attitude directly affected behavioral intention at 2 weeks; and subjective norm affected behavioral intention indirectly at 2 weeks and directly at baseline and at 4 weeks.
Conclusions:
Patients' acceptance of HIT is affected by the factors proposed in our research model. It is suggested that healthcare stakeholders consider and address the effects of these factors and their variations over time before implementing HIT.
Introduction
Health information technology (HIT) interventions, herein referred to as patient-focused, computer-based health applications, 1 have become popular for chronically ill patients because the technology can provide patients with easy access to resources that can augment their ability to engage in self-care activities, which in turn may lead to better patient health outcomes, well-being, and quality of life. 2 –5 However, patients do not always accept and sustain the use of this technology, 6 –8 which can be of significant concern because nonacceptance or nonuse of the technology may prevent them from realizing its full benefits and can lead to failure to implement the technology. To promote patients' acceptance and sustained use of HIT, it is essential to understand the factors that may influence acceptance of the technologies.
Many studies of such factors have been qualitative. For instance, Zhang et al. 6 interviewed patients about their use of an e-appointment scheduling system and found that acceptance was associated with the system's functionality and the patient's characteristics. Hoaas et al. 8 conducted semistructured focus groups and found that patients' perceived improvement in health benefits, self-efficacy, and emotional safety were the factors that affected their use of a telerehabilitation system to manage their chronic obstructive pulmonary disease. In Radhakrishnan et al., 9 patients who used a telehealth system to monitor heart failure were interviewed, and the results indicated that patients' use of the system was affected by their own health conditions and by the perceived usefulness of the system.
Quantitative studies of factors that affect patients' acceptance of HIT have also been performed; however, only a few were conducted in longitudinal contexts, and the research contained limitations. For example, Kelley et al. 10 studied patients' use of a Web-based e-Health system over a 12-month period. Acceptance surveys were conducted when the patients entered the study and every 3 months thereafter. However, their research hypotheses were tested using data that were pooled across all time points, which overlooked the potential changes in patients' responses over time. In Klein, 11 patients' use of an Internet-based patient–physician communication application was examined for a 12-month period. However, their hypotheses were tested based on patients' responses collected at only one time point, which may not have been representative of the whole study period.
In this study, we set out to examine factors that may have affected patients' acceptance of a computer-based, chronic disease self-monitoring system over a 4-week period. A research model concerning patients' acceptance of HIT was developed and tested using data collected at three different time points during the study period.
Theoretical Background and Research Hypotheses
We developed our research model using Davis's technology acceptance model (TAM) 12 as a theoretical basis to specify which factors to study and the relationships among them because it provides a reliable foundation for examining individuals' HIT acceptance. 13,14 In this study, acceptance was measured as patients' behavioral intention to use the disease self-monitoring system. Based on TAM, two key factors were posited to predict acceptance: perceived usefulness, which refers to the degree to which patients believe that using the system will enhance their performance in managing chronic conditions, and perceived ease of use, which refers to the degree to which patients believe that using the system will require little effort. The effects of these two factors on acceptance were believed to be mediated by attitude, which refers to patients' positive feelings about using the system. Subjective norm, which refers to the degree to which patients perceive that people who are important to them think that they should use the system, was also included in our research model because the opinions of important others can influence patients' health-related behaviors. 15,16 Previous studies outside healthcare have shown the significant effects of subjective norm on perceived usefulness, perceived ease of use, attitude, and behavioral intention 17 ; however, the pertinent evidence within the health informatics discipline is lacking. Further studies on how subjective norm influences patients' HIT acceptance and how the effects may change over time are needed. Based on theoretical considerations, the following hypotheses were posited in our research model (Figure 1):

Research model and hypotheses.
H1: Perceived ease of use will have a significant positive effect on perceived usefulness.
H2: Perceived usefulness will have a significant positive effect on attitude.
H3: Perceived ease of use will have a significant positive effect on attitude.
H4: Attitude will have a significant positive effect on behavioral intention.
H5: Perceived usefulness will have a significant positive effect on behavioral intention.
H6: Subjective norm will have a significant positive effect on behavioral intention.
H7: Subjective norm will have a significant positive effect on attitude.
H8: Subjective norm will have a significant positive effect on perceived usefulness.
H9: Subjective norm will have a significant positive effect on perceived ease of use.
Materials and Methods
Study intervention
The HIT involved in this study was a computer-based, chronic disease self-monitoring system that was based on a user-centered design process. The system comprised a two-in-one blood glucose and blood pressure monitor connected to a 10-inch touchscreen tablet computer that enabled patients to measure and track their blood glucose, blood pressure, and pulse. The system automatically stored the measurement records and indicated whether they were within a normal range. All measurement records were presented in structured tables and graphs in which normal values were displayed in black and abnormal values were displayed in orange or red based on the specific situation. The system also provided video-based educational materials that allowed the patients to learn proper self-management of their chronic conditions, such as how to measure blood glucose and blood pressure, collocate diet, and exercise.
Participants
We recruited participants from three community health centers of a nonprofit health service network. The participant inclusion criteria were as follows: (1) age of 18 years or above with a diagnosis of type 2 diabetes mellitus and/or hypertension for at least 3 months, (2) a prescription for oral hypoglycemic and/or antihypertensive medications, (3) normal (or corrected-to-normal) vision, (4) no cognitive or physical impairment, (5) the ability to learn and perform computer-based disease self-monitoring, and (6) the ability to understand written and spoken Chinese. Patients with unstable or life-threatening conditions were excluded.
Outcome measures
An HIT acceptance questionnaire that comprised measurement items adapted from previously validated scales 18 –20 was developed to measure the factors in the model. Interviews with 10 senior citizens (5 males and 5 females) were conducted to modify the measurement items to ensure that they could be comprehended as intended by the target population. We used 7-point Likert-type scales ranging from 1 (very strongly disagree) to 7 (very strongly agree) to assess the measurement items. Table 1 shows the factors and measurement items used in this study.
Factors and Measurement Items Used in This Study
ATT, attitude; BI, behavioral intention; PEOU, perceived ease of use; PU, perceived usefulness; SN, subjective norm.
Procedures
This study examined the acceptance of HIT for a 4-week period, during which the participants were provided with the disease self-monitoring system, blood glucose test strips, and lancets at no cost. The participants were trained and encouraged to use the system to monitor their chronic conditions at home while continuing with the usual care recommended by their healthcare providers. The acceptance questionnaire was administrated to participants during home visits conducted at baseline and 2 weeks and 4 weeks after implementation. The participants' demographic information, including age, sex, education level, and self-rated computer experience, was collected.
Data analysis
A power analysis was performed using G*Power to determine the number of participants for model testing. The internal consistency reliability was assessed for each factor in the model by examining Cronbach's alpha, of which a value higher than 0.7 was considered acceptable. 21 Curve estimations were performed to test the assumption of linearity. Multicollinearity was tested by computing the variance inflation factor (VIF) of the independent variables in each subpart of the model. A VIF of less than 10 indicated an absence of multicollinearity. 22,23 Path analysis was used to examine the relationships among the factors at each time point. Maximum likelihood estimation was used for model fitting and parameter estimation. The path coefficients indicated by standardized regression weights and squared multiple correlations (R 2 ) for dependent variables in the model were calculated using SPSS Amos for Windows. Four commonly used goodness-of-fit indices were used to assess the overall fit of the model; a good model fit was indicated by the ratio of χ2 to degrees of freedom (χ2/df <3), 22 the comparative fit index (CFI ≥0.95), 24,25 the Tucker–Lewis index (TLI ≥0.95), 24,26 and the root mean square error of approximation (RMSEA <0.06; although RMSEA values as high as 0.08 are considered acceptable). 24,27
Ethics
This study received ethical approval from the institutional review board of the University of Hong Kong/Hospital Authority Hong Kong West Cluster and informed consent was obtained from all participants.
Results
Sample size and participant characteristics
Our power analysis indicated that 36 observations were needed to detect an effect size f 2 of 0.35 with 80% statistical power at the 0.05 significance level. In this study, 42 participants completed the questionnaire at baseline. Because of withdrawal and loss to follow-up, the data of four participants (two males and two females) were not collected at 2 weeks and those of another four participants (three males and one female) were not collected at 4 weeks. Therefore, the data from 42, 38, and 38 participants were used in the analyses for baseline, 2 weeks, and 4 weeks, respectively. Table 2 presents the participants' demographic characteristics.
Demographic Characteristics of the Study Sample
Internal consistency reliability
Table 3 shows the means, standard deviations, and Cronbach's alphas for the factors at baseline, 2 weeks, and 4 weeks. The measurement scales showed good internal consistency reliability, except that Cronbach's alpha for subjective norm at baseline was slightly lower than 0.7.
Means, Standard Deviations, and Cronbach's Alphas for the Factors at Baseline, 2 Weeks, and 4 Weeks
Testing of linearity and multicollinearity
The linearity assumption for path analysis model testing was fulfilled as all paths in our model indicated linear relationships at the significance level of 0.01 (see Table 4). Table 5 shows that all VIF values were below 10, indicating the absence of multicollinearity in the model.
Curve Estimations for Linearity Assumption Test
Results of Multicollinearity Tests
VIF, variance inflation factor.
Model testing
The fit indices showed an adequate fit between the model and the data for 2 weeks and 4 weeks, but less of a fit for baseline (χ2/df = 5.719, CFI = 0.963, TLI = 0.628, and RMSEA = 0.339 for baseline; χ2/df = 1.360, CFI = 0.997, TLI = 0.973, and RMSEA = 0.099 for 2 weeks; and χ2/df = 1.046, CFI = 1.000, TLI = 0.997, and RMSEA = 0.035 for 4 weeks).
As shown in Figures 2 –4, H1, H6, H7, H8, and H9 were supported at baseline; H1, H2, H3, H4, H7, H8, and H9 were supported at 2 weeks; and H1, H2, H3, H5, H6, and H9 were supported at 4 weeks. Overall, our model was able to account for 51%, 46%, and 76% of the variance in patients' behavioral intention to use the disease self-monitoring system at baseline, 2 weeks, and 4 weeks, respectively.
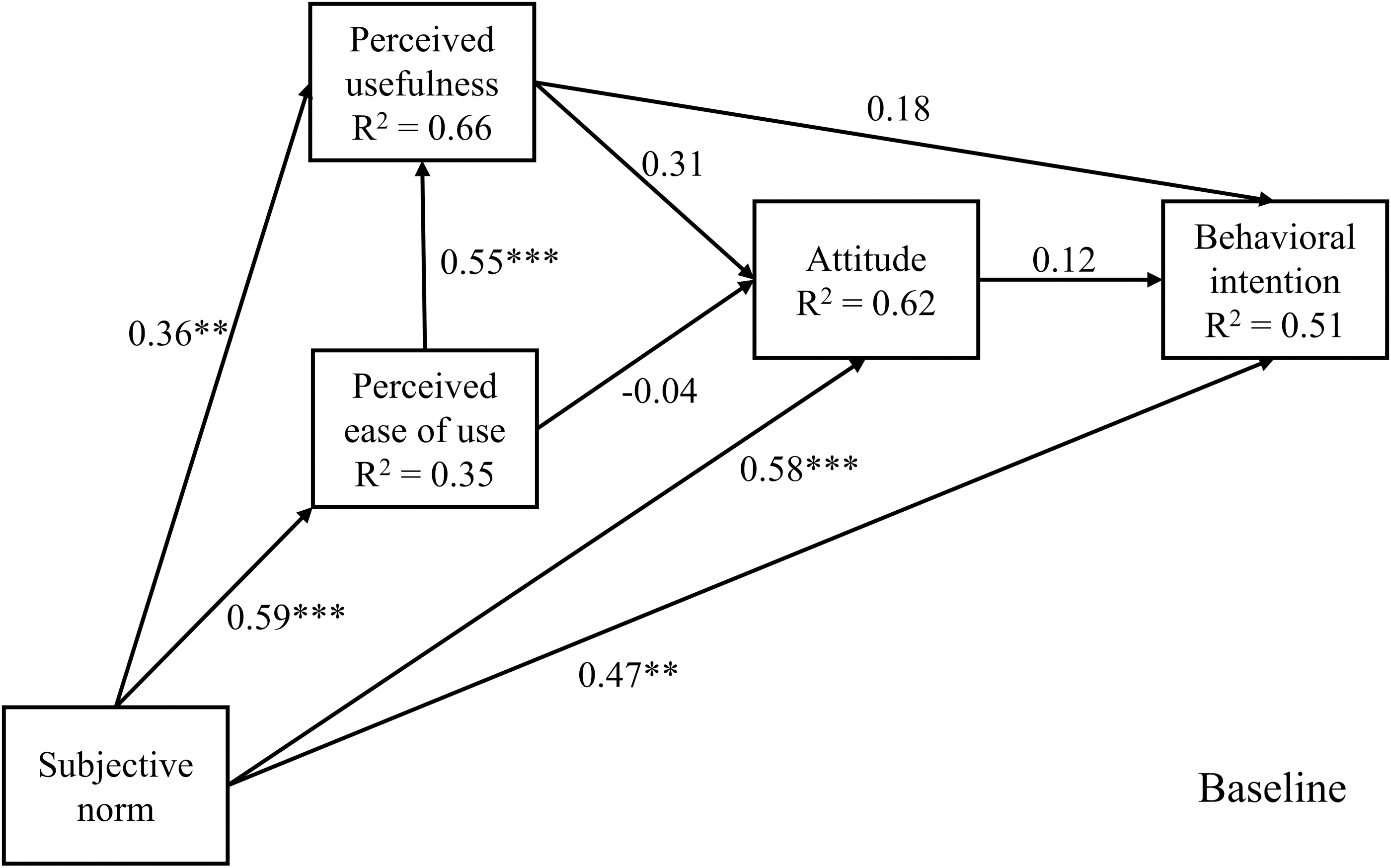
Path diagram for baseline (**p < 0.01; ***p < 0.001).
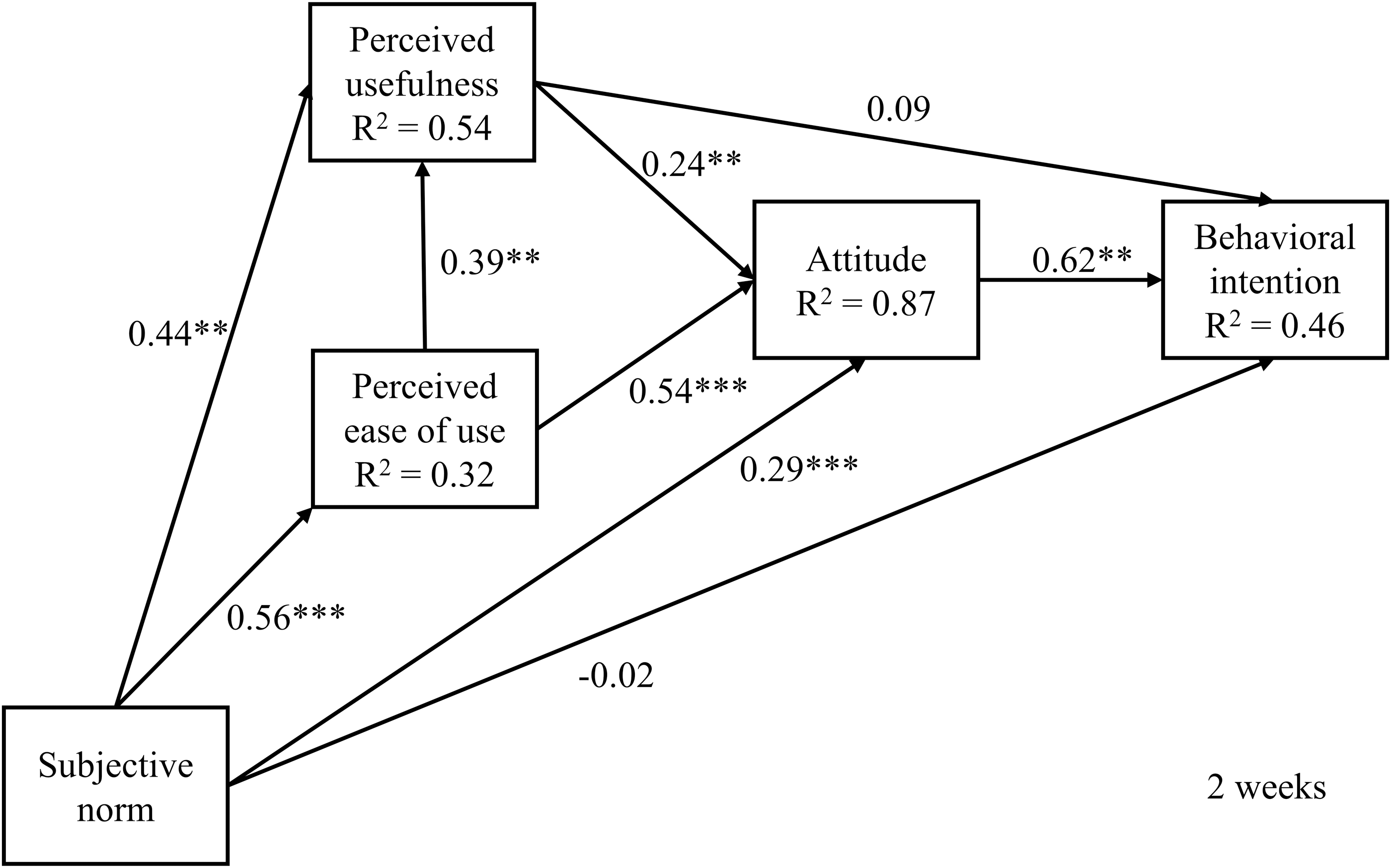
Path diagram for 2 weeks (**p < 0.01; ***p < 0.001).
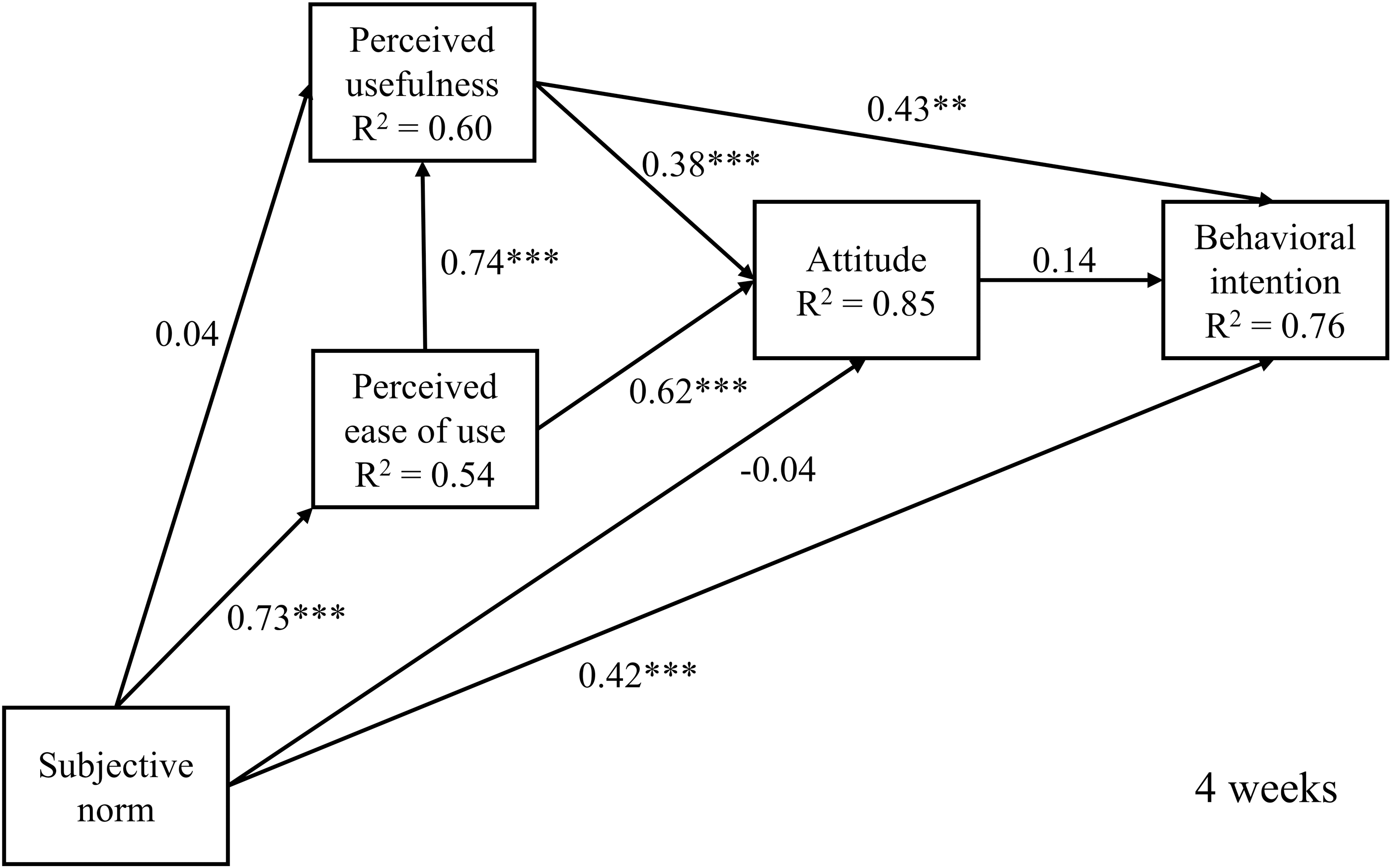
Path diagram for 4 weeks (**p < 0.01; ***p < 0.001).
Discussion
E-health initiatives focusing on the integration of HITs into patients' chronic disease self-care have been developed because they can improve patients' access to care resources and enable remote monitoring. However, some studies have shown a decline in patients' use of HIT, especially during the first few weeks. 28,29 This finding underscores the importance of studying patients' acceptance of HIT in the preliminary implementation stages. Our study examined patients' acceptance of a computer-based, chronic disease self-monitoring system at baseline, 2 weeks, and 4 weeks to identify the relationships between the perceived usefulness, perceived ease of use, attitude, and subjective norm and behavioral intention and to test how the relationships changed over a 4-week period. Overall, as indicated by the model fit indices, our research model fit the data well at 2 and 4 weeks, but less well at baseline. This suggests that this HIT acceptance model may apply better during the postimplementation stages, which could be attributed to variations in the concerns that patients may have regarding acceptance over time. 30,31
Our study found that perceived usefulness had no significant effect on behavioral intention at baseline, an indirect effect mediated by attitude on behavioral intention at 2 weeks, and a direct effect on behavioral intention at 4 weeks. The changes may be due to the process whereby patients familiarize themselves with the use of the system. Patients may have limited ideas about the usefulness of the system at the initial stage, but they may experience benefits with increased use over time. Therefore, the effect of perceived usefulness on behavioral intention emerged over the study period. Proper training delivered before implementation to familiarize patients with the use of the technology could be one of the principal methods to help patients shorten the process of recognizing the usefulness of HIT and realizing its benefits. 32,33 In addition, it is suggested that the intended target users be actively involved in the process of technology design and development to study their requirements and preferences to provide them with the desired functions and features.
Like previous studies, 11,34 –37 our study showed a significant effect of perceived ease of use on perceived usefulness. Perceived ease of use was also deemed to be important in acceptance because it showed indirect effects mediated by perceived usefulness and/or attitude on behavioral intention at 2 and 4 weeks. This indicates that patients who perceive that HIT is easy to use would be more likely to perceive the technology as useful, which would in turn generate positive feelings toward acceptance. Therefore, HITs should be designed to be user-friendly for the end users. Achieving this may require iterative usability evaluations, followed by careful attention to human factors and principles, both before and after implementation. One should also consider designs that are tailored for older adults, such as avoiding the use of small font sizes in the system interface, because they may be more likely to suffer from chronic conditions and functional decline or disability than younger populations. 38 –42
Patients' attitude was found to influence their behavioral intention to use the disease self-monitoring system only at 2 weeks. Thus, the effects of perceived usefulness, perceived ease of use, and subjective norm on behavioral intention were mediated by attitude at 2 weeks, but not at baseline and 4 weeks. This seems to agree with the argument of some studies that attitude may not be an appropriate mediator between the perceived beliefs and behavioral intention. 18,19,30,43 Moreover, it could be noted that the direct effects of perceived usefulness on behavioral intention appeared to grow over the mediation effects of attitude over time, implying that the determinant role of attitude on behavioral intention might become less important when other factors such as usefulness are independently taken into account (p. 166). 19 More research is needed to further examine the role of attitude on patients' acceptance of HIT over a longer period.
In this study, subjective norm was found to influence behavioral intention either directly (at baseline and 4 weeks) or indirectly (at 2 weeks). Although subjective norm exerted a consistent influence on perceived ease of use over the study period, its effects on attitude and perceived usefulness appeared to diminish over time. This implies that patients' initial attitudes toward acceptance and perceptions about the usefulness of the technology may rely substantially on other referents' opinions, which may, along with increased use over time, become less important to patients as they gain hands-on experience with the technology. Therefore, it is suggested that patients' important others (e.g., family members, close friends, and caregivers) consider means to cultivate a positive social environment that helps to develop the patients' initial acceptance of HIT, such as by emphasizing to patients the usefulness of the technology in managing chronic conditions and providing prompt help when needed.
This study had several limitations. First, the small sample size restricted us from including more factors in the research model. A larger sample would have allowed the examination of more factors that may be relevant to HIT acceptance. Second, although our study provides important information about factors that affect patients' acceptance of HIT in the preliminary 4-week period, it would be meaningful to study acceptance over a longer period, particularly when dealing with chronic diseases that require long-term care. Third, we used behavioral intention to measure acceptance because it is a common indicator of the variable. 44 However, actual usage of the technology can also be considered for the measurement as it represents an objective approach to understand acceptance. The relationship between patients' behavioral intention to use the HIT and their actual usage behavior awaits further examination.
Conclusions
This study shows that patients' acceptance of HIT was affected by the factors proposed in our research model. These effects varied over the 4-week period. The effect of perceived usefulness on behavioral intention tended to increase over time. Perceived ease of use affected behavioral intention indirectly at 2 and 4 weeks. Attitude affected behavioral intention only at 2 weeks. Subjective norm was shown to be a prominent factor in behavioral intention and other perceived beliefs both before and after implementation. It is hoped that the likelihood of patients' acceptance of HIT can be increased by applying the findings of this study.
Footnotes
Acknowledgment
The study was conducted with the support of the General Research Fund of the University Grants Council of Hong Kong (PI: Calvin Or; project #: 716211).
Disclosure Statement
No competing financial interests exist.