
Abstract
Purpose:
Veterans with dementia and their caregivers in remote areas may not have access to specialists to provide diagnosis, treatment, and education. The purpose of this clinical demonstration project was to examine the feasibility, acceptability, and impact of a video consultations clinic for veterans with dementia or memory complaints and their caregivers.
Methods:
The dementia clinical video telehealth (CVT) consultation clinic was established to identify, diagnose, and treat dementia in veterans at sites distant from the main medical center. A geriatrician at the main facility provided video consultation to patients and caregivers at seven satellite facilities. Diagnoses made and services provided were recorded after the initial consultation. Patient and caregiver satisfaction with the CVT clinic were assessed.
Findings:
Ninety-four patients were evaluated in the CVT dementia clinic (average age = 74.7; average Mini-Mental State Exam = 24.4). Forty patients had a prior dementia diagnosis, 15 received a new dementia diagnosis, and 20 a new mild cognitive impairment diagnosis. Of the remaining patients evaluated for memory complaints, seven were found to have depression, three had hearing loss, and three had traumatic brain injury. After CVT consultation, common referrals included social work (n = 43), neuropsychology (n = 36), and brain imaging (n = 26). Patients and caregivers expressed high satisfaction with the video consultation and 90% of caregivers indicated they would rather use CVT than travel to see the specialist in person.
Conclusions:
Video consultation was well accepted by both dementia patients and caregivers. CVT may facilitate timely diagnosis and management and provide support for rural dementia patients and caregivers.
Introduction
Dementia is often under-recognized in primary care settings. 1,2 Early diagnosis, treatment, and follow-up of dementia patients are especially important given the consequences of delayed or missed diagnoses. 3 These include potentially missed opportunities to manage symptoms, discontinue undesirable medications, manage coexisting medical conditions, provide caregiver support, and plan for future care. 4 Timely diagnosis and intervention may reduce healthcare costs, increase the quality of life for patients, delay institutionalization, and reduce caregiver burden. 5,6
In urban areas, major medical centers commonly have interdisciplinary or specialty clinics that provide comprehensive diagnostics, treatment, and education to patients and their caregivers. Workup and management of dementia are more difficult for rural patients and their caregivers with significantly more barriers. 6,7 Rural medical facilities often do not have specialty dementia clinics or providers trained in dementia care. Persons with dementia may have difficulty making trips to a major medical center because of mobility, transportation, and behavioral issues. These patients can become anxious or agitated in unfamiliar locations. As their travel is dependent on caregivers, it can increase caregiver burden.
Rural caregivers already face more challenges than those in urban areas as access to formal support services such as home health, transportation, or caregiver support groups is limited. 7,8 These caregivers would benefit from greater access to additional services that may reduce caregiver burden.
Similar challenges are faced by veterans and their families who receive care by the Veterans Health Administration (VHA). Many veterans reside far from the main medical facility and receive primary care in its satellite facilities. They often do not have access to specialists in these remote clinics.
One potential solution to increase access for rural patients with memory problems and their families is to use video telehealth. There are a few published reports of memory clinics targeting rural residents that evaluate video technology using an interdisciplinary team approach to deliver services for assessment, management, and follow-up of dementia patients and supporting the dementia family caregivers. 9 –11 Most of these initial reports are mainly based on small samples and have examined a focused aspect of a comprehensive memory disorders clinic, such as the validity of the Mini-Mental State Exam (MMSE) or neuropsychological assessment through telehealth. 12,13 Although these preliminary studies have shown feasibility of the video telehealth approach and stakeholder acceptance and satisfaction, 10,14 more work needs to be done to make this approach mainstream. None of the previous reports have used a single geriatrics provider to provide dementia consultation for both initial and follow-up visits and for both patients and caregivers. Our work evaluated a single-provider model that may be easier to implement in clinical practice, compared with an interdisciplinary program. We established a dementia clinical video telehealth (dementia CVT) consultation clinic within the Miami VA Healthcare System (VAHS) as a clinical demonstration project. The primary goal of this study was to examine the feasibility and acceptability of this clinic to veterans and their caregivers. The secondary goal was to assess referrals made and support provided.
Methods
The dementia CVT clinic was set up by a geriatrician at the main facility to provide consultation to seven satellite facilities. A consultation request for this clinic was created in the VA's Computerized Patient Record System (CPRS). Consult documentation templates were also created for both the preclinic and clinic visits to guide the assessment and ensure consistency in reporting.
Staff Training
All telehealth programs within the VA are supported by telehealth clinical technicians (TCTs), who are allied healthcare professionals (e.g., Licensed Practical Nurses). They help manage telehealth clinical encounters from the patient and provider location, including checking in patients, explaining the CVT procedure, and setting up the patients for CVT visits.
The TCTs at the seven satellite facilities were trained by a psychologist and the project coordinator on how to perform the MMSE, and their competence in administering this examination was certified by the psychologist. This training was done using a standardized protocol and competency checklist that is used to train medical students and residents. 15
Technology for the CVT Clinic
A Cisco TelePresence HD USB camera and the Cisco Jabber Video for TelePresence software were added to the provider's desktop computer to allow direct video communication to each satellite facility. For communication from the patient at the satellite clinic to the provider at the main hospital, we used a Cisco TelePresence Precision 60 camera connected to a high-definition television.
Intervention
Primary care providers at the satellite clinics submitted the consultation request template through CPRS in order for patients to be seen in the dementia CVT clinic. The TCTs at the satellite clinic sites then scheduled the appointment.
Preclinic Assessment
Before each CVT visit, the project coordinator at the main site performed a patient assessment over the phone using validated questionnaires available through CPRS. Each assessment consisted of the Geriatric Depression Scale (GDS) short form, 16 SF-36 Health Survey, 17 Katz Activities of Daily Living (ADLs) scale, 18 Lawton–Brody Instrumental Activities of Daily Living (IADLs) scale, 19 and the Functional Assessment Staging (FAST) survey. 20 If patients were unable to answer, the caregivers responded if available. Caregivers were also assessed for social support, depression using the PHQ-9, 21 and caregiver burden using the 12-item Zarit burden interview. 22 All responses were entered into CPRS.
Clinic Visit
Patients were asked to come to the consultation with their caregivers if they had one, and to bring their medications. They were asked to arrive 30 min before the CVT appointment time. Upon arrival, they were checked in by the TCT who explained the telemedicine process, administered the MMSE, 23 measured vital signs, and set up the patient and caregiver comfortably in a private room with a large television screen on which they would see the geriatrician at the main site. The TCT also entered a short note into CPRS with the patient's MMSE score. This allowed the TCT to code the visit and capture their workload.
The TCT then contacted the geriatrician at the central location through the Jabber Video software. When a connection was established, the visit continued similar to a face-to-face visit. The provider conducted an interview with the patient and caregiver and performed a comprehensive geriatric assessment focusing on the cognitive, functional, and social domains. The caregiver evaluation addressed patient problem behaviors, living situation, home safety, social support, awareness of resources available, and needs assessment, and reviewed data gathered in the preclinic visit. The clinician then made referrals to social work and other services depending on the needs identified. Figure 1 shows the workflow of the CVT dementia clinic.
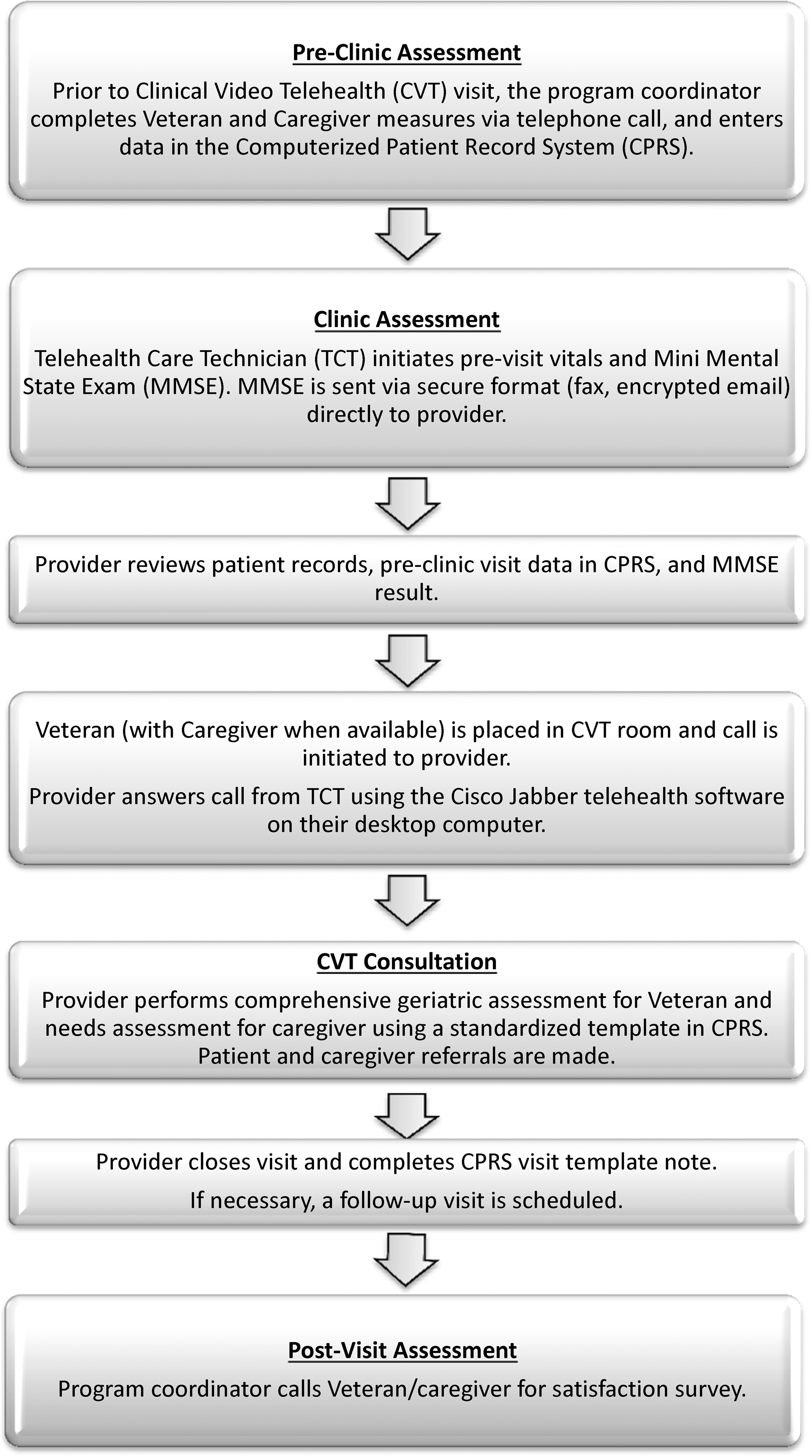
Workflow of the clinical video telehealth dementia clinic.
Postclinic Assessment
Within 2 weeks after the CVT consultation, patients and their caregivers received a telephone call to complete a telehealth satisfaction questionnaire. Respondents rated 10 aspects of the video visit experience (e.g., convenience, comfort, hearing or visual issues, and privacy concerns) and 7 items regarding the overall experience (e.g., ease of the visit, comparison with a face-to-face visit). Patients and caregivers rated their agreement with statements on a 5-point Likert scale ranging from 1 to 5, with higher scores indicating greater agreement.
We also tracked the number and characteristics of veterans receiving consultations and support services they were referred to.
Analysis
The data were entered into an Excel spread sheet (Microsoft Excel 2010) for analysis. Descriptive statistics (means, standard deviation, range, etc.) were calculated for all variables.
Results
Ninety-four patients were evaluated for a 19-month period. They completed a total of 116 visits; 18 patients were seen twice and 2 patients were seen three times. The average age of the patients was 74.7 years (range 36–95). Table 1 displays the results from the preclinic assessment. The average scores are representative of a mild level of impairment: MMSE = 24.4/30, FAST = 2.9/6, GDS = 4.6/15, Katz ADLs = 16.9/18, and Lawton's IADLs = 1.8/8. Table 2 displays the caregiver demographics. We were able to reach 41 of the caregivers either in the preclinic call or during the visit, of whom 33 were family caregivers and 8 were paid caregivers. Most of the caregivers were female (95%), married (81%), and white (71%). Table 3 displays the data from the preclinical caregiver assessments. Sixteen caregivers completed the detailed surveys. The mean PHQ-9 score was 4.1 ± 4.2, and the mean Zarit burden interview score was 11.4 ± 7.8. Data from CPRS documentation revealed that 40/94 (43%) veterans seen had a prior diagnosis of dementia, 15/94 (16%) received a new diagnosis of dementia (Alzheimer's, Vascular, or Lewy Body), and 20 (21%) received a new diagnosis of mild cognitive impairment (MCI). Seven patients referred for memory problems were identified as being depressed, three as having hearing loss, and three with a traumatic brain injury. Additional tests and referrals made by the dementia CVT clinic are shown in Table 4. The most common referrals were to social work (n = 43), for advance directives, caregiver education and support, and respite care.
Veterans Preclinic Assessment (n = 94)
Single question scored out of 5
FAST, Functional Assessment Staging survey; MMSE, Mini-Mental State Exam.
Caregiver Demographics (n = 41)
SD, standard deviation.
Caregivers Preclinic Assessment (n = 16)
Single question scored out of 5
Tests and Referrals Ordered
Patient and Caregiver Satisfaction
Results from the postvisit satisfaction surveys with veterans (n = 27) and family caregivers (n = 11) are displayed in Table 5. Ninety-six percent of the veterans and 91% of the caregivers surveyed found the video visit experience convenient. Twenty-six percent of the veterans were not fully satisfied with the quality of the sound during the video visit; however, none of the caregivers expressed concerns with the sound quality. In general, there was a high level of satisfaction with the overall clinic experience with 88% of the patients and 91% of the caregivers responding positively. Of note, 65% of the patients and 91% of the caregivers felt that they preferred to see the specialist through CVT rather than in person. Twelve percent of the patients did not express a preference.
Satisfaction Survey Results
CVT, clinical video telehealth.
Discussion
This project evaluated the feasibility and acceptability of a dementia CVT clinic for veterans with memory problems and their caregivers. This is one of the first published reports on a geriatrician-provided video consultation for memory complaints to patients and caregivers that provided follow-up and tracked referrals for support services.
By providing evaluation and management of patients with dementia through CVT, they did not need to travel to the main medical facility to receive specialty care, and were able to receive the consultation at the clinic in their local community. This project achieved its goal to improve access to care, timely diagnosis and management of dementia, and referrals to appropriate support services.
The most frequent reasons for the CVT consultation by the primary care providers were assessment of cognitive decline and management of previously diagnosed dementia patients. A number of new cases of dementia and MCI were diagnosed. Most patients were referred early (average MMSE 24.4 and 62% with MMSE 25–30), and several patients were still living and driving independently. This suggests that although primary care providers were recognizing potential early warning signs of memory impairment, they may not have been comfortable making a dementia or MCI diagnosis. In addition to diagnosing new cases of dementia, we identified patients referred for memory complaints who turned out to have other geriatric syndromes such as depression and hearing loss. These cases might have been overlooked or misdiagnosed had they not been referred to a geriatrician-led clinic. Primary care providers were also referring previously diagnosed dementia patients, perhaps recognizing their own limitations in managing these complex cases.
Caring for loved ones with dementia extracts a huge physical, emotional, and financial toll from the family caregivers. 24,25 Individuals with Alzheimer's require increasing levels of supervision and personal care as the disease progresses. High levels of burden and depression are reported in caregivers, 26,27 and the survival and quality of life of the dementia patient have been shown to be related to the welfare of the caregiver. 28 –31 In our study, 25% of the caregivers reported severe burden. The dementia CVT clinic allowed us to provide patients and caregivers referrals to much needed support services, particularly social work. The geriatrician identified needs for advance directive discussion, caregiver education/support, and respite and home health aide services based on the previsit and visit interview with the patient and caregiver. Maximizing opportunities to provide timely and needed support may reduce caregiver burnout.
A common factor among effective dementia caregiver interventions such as in the Partners in Dementia Care program 32 is improved access to needed services that can be helpful in reducing caregiver depression, burden, and anger. Although we were not able to evaluate the impact of our intervention and referrals on caregiver burden, these caregivers may benefit from frequent caregiver reassessment. 4 The CVT modality may facilitate such reassessment.
Results from this project show that CVT dementia consultation is feasible and acceptable to both patients and caregivers. Contrary to concerns that the advanced age of the patients (and caregivers) could pose challenges to using CVT technology because of sensory impairment and limited familiarity with this type of technology, the patients and caregivers had little trouble with the CVT modality and embraced it well. A quarter of the patients were not fully satisfied with the sound quality during the CVT visit. However, since none of the caregivers voiced similar concerns, it is likely that these patients had pre-existing hearing loss that may have also evidenced itself during a face-to-face encounter. One patient even commented that he “liked being on television and felt like a star” (he could see himself on one corner of the monitor). Except for three instances, there were no technical issues such as connection difficulty or images freezing, disconnecting and reconnecting resolved these issues. In general, there was a high level of satisfaction with the overall clinic experience, and most patients and caregivers preferred to see the specialist through CVT rather than travel to the distant main facility.
This study had a number of limitations. As the geriatric consultation was provided by only one geriatrician, it limited the availability of appointment slots. Scheduling an appointment time that worked for the veteran, caregiver, clinic provider, and TCT proved challenging on occasion. Having additional specialty providers would provide greater scheduling flexibility. Another limitation is relative lack of caregiver data. Some patients did not have caregivers, several caregivers were either not reachable or amenable to completing the detailed assessments, and paid caregivers were not included in the assessment. As this was a clinical demonstration project, we chose to make the surveys optional so patients and caregivers would not be discouraged from attending the clinic.
This report incorporated clinical data for 94 patients, which is one of the larger sample sizes in the reports on memory CVT clinics to date. In this era of rapidly advancing CVT technology, similar clinics can be established by other VA and non-VA Health Systems.
Some previous studies have demonstrated reliability of the neurological examination 33,34 and cognitive testing 35 through CVT, and reliability and validity of CVT in diagnosing dementia. 14,36,37 Others have reported on the effectiveness of a multidisciplinary team in diagnosing and managing dementia patients through CVT. 33,34 Our dementia CVT model incorporated both initial diagnosis and follow-up, using a single specialty provider, thereby making it easier to replicate. With appropriate staff training, this model could also be used for diagnosis and management of other geriatric syndromes such as incontinence, frailty, polypharmacy, and falls.
This project affirms the role for CVT technology in the evaluation and management of dementia. Access to a geriatric specialist at remote locations through CVT may help address the geriatrician workforce shortage that is particularly prevalent in rural areas. Future studies should examine the longer term impact of such CVT models on patient and caregiver outcomes, as well as cost and sustainability for the healthcare system.
Footnotes
Acknowledgments
Funding for this project was provided by the VHA Office of Rural Health. The project was also supported by the Miami VA Geriatric Research, Education, and Clinical Center. Findings in this article were presented, in part, at the Gerontological Society of America's 68th Annual Scientific Meeting (November 18, 2015) and the Geriatrics & Extended Care Leads Virtual Conference (April 26, 2016).
Disclosure Statement
No competing financial interests exist.