
Abstract
Purpose:
Pediatric transport teams rely on communication to report patient data to medical command officers, who create care plans and determine disposition. Common destinations are the emergency department (ED), pediatric intensive care unit (PICU), or regular inpatient care area (RIPCA). Telephone report does not result in complete understanding of the patient's condition. Further workup in the ED is often required. Telemedicine allows the patient to be directly seen; parents to be interviewed; and laboratory studies, radiographs, and vital signs to be reviewed. We hypothesized that telemedicine would improve understanding of the patient and result in more accurate disposition.
Design:
Patients within our hospital from 2012 to 2013 were compared with patients transported using our telemedicine program from April 2014 to April 2015.
Results:
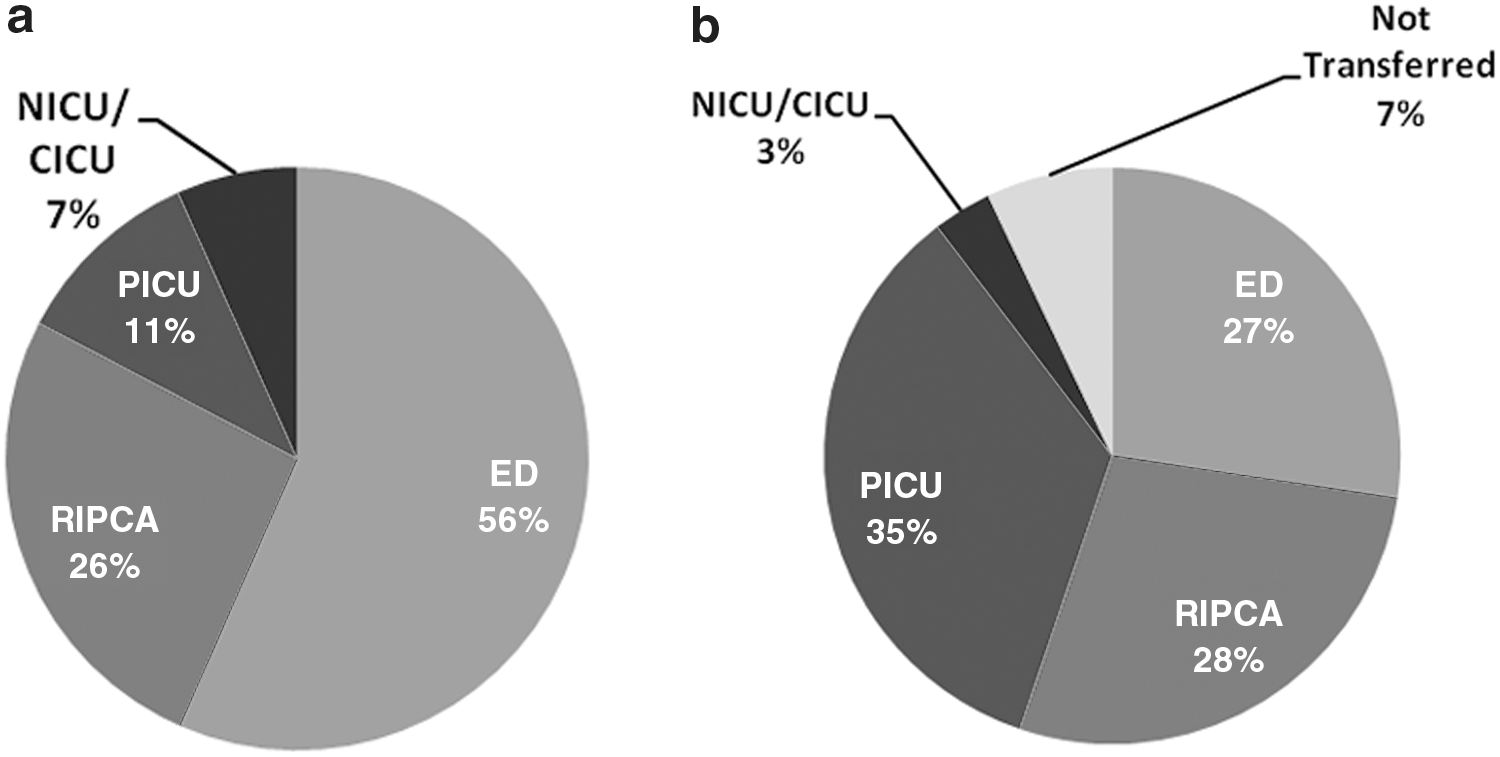
From 2012 to 2013, a total of 4,662 transports were performed. Of these, 4,067 were inbound transports, 2,302 of these patients were sent to ED (56.6%), 1,062 were sent to RIPCA (26%), and 431 were sent to PICU (10.6%). Over a year-long period of telemedicine implementation, 212 patients used telemedicine and were analyzed. ED utilization decreased to 27% (p < 0.0001), PICU increased to 34.4% (p < 0.0001), and RIPCA rates remained the same at 28% (p = 0.203). Of ED dispositions, 58.6% were admitted to RIPCA for further care, 13.7% to PICU for escalation of care, and 24.1% were discharged. Of RIPCA dispositions, 10% had rapid responses; 0 had code blues. Of PICU dispositions, 90.4% had care escalation; 9.6% were observed in the PICU without escalation.
Conclusion:
Telemedicine use in transported pediatric patients can positively alter disposition patterns.
Introduction
Telemedicine can be defined as the exchange of medical information from one site to another through telecommunications or other electronic technology. This can provide access to health assessment, diagnosis, intervention, consultation, supervision, and information across distances. 1,2 It may encompass an array of technologies, including videoconferencing, Internet, streaming media, images, or wireless communications. The earliest telemedicine application was in radiology—analyzing and interpreting stored then forwarded digital images. 3 Support strengthened with expansion into the dermatology and pathology fields. 1 Improved cost and technological advances now allow for live streaming of digital video, allowing telemedicine to be applied in many new clinical specialties. The ultimate goals remain the same as outlined in the American Academy of Pediatrics telemedicine recommendation regarding pediatric healthcare: to improve access to care, to provide more patient family centered care, and to increase efficiency. 4
Pediatric transport teams have long relied on telephone communication to report patient examination findings, laboratory, and radiographic data to medical command officers (MCOs) responsible for children's care during transport. Strong communication is an integral part of safe and efficient transports. The MCO (a pediatric intensive care attending physician or a supervised pediatric intensive care fellow) uses this information to initiate care plans during transport and to determine the appropriate patient disposition within the receiving hospital. The most common destinations for disposition are the emergency department (ED), the pediatric intensive care unit (PICU), the regular inpatient care area (RIPCA), neonatal intensive care unit (NICU), or cardiac intensive care unit (CICU).
At times, report by telephone alone does not fully communicate the patient condition or disease process, and often the patient may require transport to the receiving ED for further workup and evaluation. This burdens the ED team leading to unnecessary or repeated testing, and can be associated with morbidities and additional charges to the patient. The purpose of this retrospective analysis is to demonstrate that the use of telemedicine to observe the patient rather than receive a verbal description by phone will lead to a better understanding of the disease process and patient acuity resulting in a more accurate disposition within the receiving hospital when compared with phone communication.
Materials and Methods
A retrospective cohort study was conducted using data obtained from Epic (Verona, WI), an electronic medical record system. Patients transported by the Nemours Kids Transport Team (NKTT) were studied, comparing those transported without telemedicine consultation with those who were transported and received a telemedicine consult before departure from the referring hospital. The study's inclusion criteria were patients aged ≤18 years old who presented to an outside hospital ED for medical care and subsequently required NKTT transportation to a higher level of medical care. Those excluded from the study were patients transported by a non-NKTT, patients who were >18 years of age, as well as those who were seen at our affiliate hospital in a different state. This study was institutional review board approved, and data collection was compliant with the Health Insurance Portability and Accountability Act (HIPAA).
Patients were grouped as either presenting through NKTT transport before telemedicine program inception (January 2012–December 2013) or after telemedicine inception (April 2014–April 2015). Instituted in April 2014, Nemours “CareConnect” is a telemedicine “smart cart” consisting of an iPad (Apple, Cupertino, CA) mobile cart connected to a secure WiFi network in five partner EDs initially. The iPads, using the HIPAA compliant secure Vidyo™ videoconferencing application, were used to visually inspect the patient, review studies, interview parents, and formulate plans in conjunction with ED staff. No peripheral devices such as stethoscopes or otoscopes were used to keep the system easy to use. The program then rapidly expanded to 21 additional partner sites over the subsequent months. Nemours CareConnect allowed physicians to immediately access the MCO for questions regarding the evaluation and care of critically ill patients at the time the decision for transport was made rather than having to wait until the NKTT arrived to further assess the patient. Before telemedicine inception, EDs had access to MCOs for difficult cases solely by telephone.
Pretelemedicine transports included data collected from 75 medical sites represented by EDs and community hospital pediatric inpatient floors. The post-telemedicine analysis was limited to 26 sites, EDs, and inpatient pediatric floors, with Nemours CareConnect partnerships. Disease process was not used as an exclusion criterion. The study was restricted to patients transported by the NKTT, which is composed of a pair of critical care nurses or a critical care nurse and respiratory therapist. The disposition of these patients upon arrival to our facility was then analyzed: ED, PICU, RIPCA, NICU, or CICU. Post-telemedicine patients were identified by using Epic to search for a customized telemedicine note and then crossreferencing these patients with a secure electronic list that captured CareConnect network patients as part of a quality improvement and compliance analysis.
The post-telemedicine charts were reviewed for demographics, history, physical examination, disposition, and management information. Transport records, hospital course, rapid response activations, code blue activations, and hospital discharge summaries were also reviewed. Data collected are presented in Table 1.
Telemedicine Chart Review Categories
MCO, medical command officer.
The NKTT pediatric acuity scoring system is given in Table 2. The internally derived scoring system runs from acuity level 1, which includes critical or active cardiopulmonary resuscitation, to acuity level 5, which is defined as basic life support level of care. 5 A rapid response activation system (Fig. 1) is used for patients with unexpected clinical deterioration after admission to the RIPCA and is based on a Pediatric Early Warning Score system. 6 To differentiate progression of disease versus a failure of telemedicine consultation for patients transported to the RIPCA, a 6-h time limit for inclusion was set. Rapid response or code blue activation called ≤6 h after arrival through transport was considered a failure of telemedicine in determining accurate disposition. Events occurring >6 h after transport were considered natural disease progression.
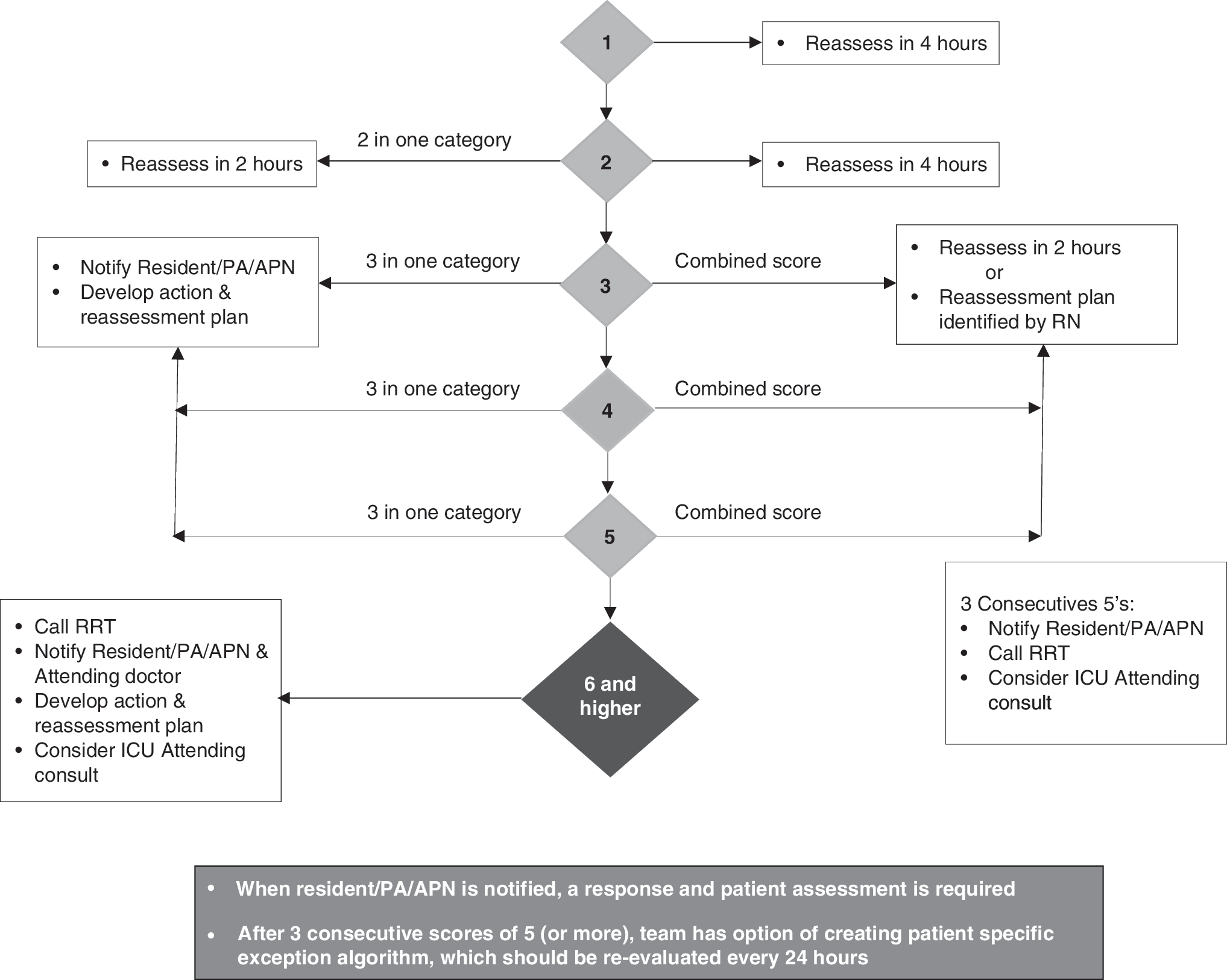
Pediatric Early Warning Score algorithm. APN, advance practice nurse; PA, physician's assistant; ICU, intensive care unit; RRT, rapid response team.
Acuity Scoring System
BLS, basic life support; BP, blood pressure; IV, intravenous.
Data were analyzed using SPSS 22.0 (SPSS, Chicago, IL). Distributions were described as mean percentage values. p Values ≤0.05 were considered statistically significant. Comparisons were made between dispositions of transported patients pretelemedicine and posttelemedicine.
Results
From 2012 to 2013 in the pretelemedicine group, there were 4,662 total NKTT transports. Of those, 4,067 were inbound transports to our facility for additional medical management, averaging 2033.5 patients per year. Over this 2-year time period, 2,302 patient transports were sent to the ED (56.6%), 1,062 patients were sent to the RIPCA (26.1%), and 431 patients were sent to the PICU (10.6%). The remaining 6.7% were divided between the NICU (219 patients, 5.4%) and CICU (53 patients, 1.3%). Of the 2,302 patients who were transported from an outside hospital to the ED, 1,556 patients (67.6%) were admitted and 746 (32.4%) were discharged home.
Over the 1-year period since the induction of telemedicine, 310 patients used the “CareConnect” telemedicine services; 212 of these patients met inclusion criteria and were analyzed. Referrals came from 26 outside hospital EDs, 6 inpatient pediatric units, and 1 PICU. Ninety-eight patients were excluded from the analysis for reasons that included but were not limited to pronouncement of death at the outside hospital, medical management that was deemed safe to continue at the outside hospital after physician-to-physician consultation, burn patients who were diverted to the regional burn center, or referrals to our affiliate children's hospital in another state (Fig. 2).

The post-telemedicine group included 93 (43.9%) females and 119 (56.1%) males. The average age was 52.4 months (4.4 years; range 7 days–17 years). Mean distance transported was 60 miles (range 4.2–91.1 miles; mode 89.6 miles). Acuity ranged from level 1 to 4. Three patients (1.3%) were assigned acuity level 1, which included two cardiac arrests and one respiratory failure. Twenty-six patients (12.3%) were designated acuity level 2. Most patients (149; 70.3%) who were transported post-telemedicine were designated acuity level 3. Twenty-two patients (10.4%) were designated acuity level 4. There were no acuity level 5 patients transported using telemedicine. Twelve patients (5.7%) did not have a documented acuity level and ultimately were not transported; care was either continued at the outside hospital or the patient was discharged from the outside ED. The average duration of a telemedicine call between the MCO and the outside provider was 5.2 min, median was 4 min. Range of duration of telemedicine calls varied from 1 min to the longest, a total of 57 min.
A variety of diagnoses were supported by telemedicine consultation and can be reviewed in Table 3. As one would expect in a pediatric population, respiratory distress was the dominant diagnosis.
Transport Diagnoses
In the post-telemedicine group, ED utilization decreased significantly to 27% (p < 0.0001) and PICU utilization increased to 34% (p < 0.0001). The RIPCA utilization rates remained the same at 28% (p = 0.203). The analysis did not focus on the minimal usage of telemedicine in the NICU and CICU as they have just recently adopted the technology. Finally, 15 patients (7.1%) had a telemedicine consult but were able to remain at the referring hospital (Fig. 3a, b).
Transport disposition
Fifty-eight patients were transported to the ED after telemedicine consultation. Thirty-four patients (58.6%) were then admitted to the RIPCA for further management, and eight patients (13.8%) were subsequently admitted to the PICU for escalation of care. A single patient was admitted from the ED after transfer to the operating room for surgical management and extraction of foreign body and then subsequently to the RIPCA for further observation. Another was admitted to the NICU after post-transport evaluation in the ED. Fourteen patients (24.1%) were discharged home after being transferred.
Of the patients admitted after transport directly to the RIPCA, there were no reported code blue events. Six of the 59 patients (10.1%), who were transported to the RIPCA, had a rapid response within 6 h of transport. Four of these were then transported to PICU for escalation of care, including increased high-flow nasal cannula (HFNC), bilevel positive airway pressure, or intubation. A single patient was transported to the PICU as the RIPCA nursing was uncomfortable with managing the patient; respiratory settings on HFNC were not increased, but closer nursing observation was maintained in the PICU. The other rapid response initiated within 6 h of transportation had malfunctioning equipment; once corrected, the patient continued care in the RIPCA. Of the 59 RIPCA transport patients who received telemedicine consultation, 24 (40.6%) were discharged from the hospital in < 24 h.
Seventy-three of 212 patients (34.4%) were admitted to the PICU after telemedicine consultation, and 90.4% of those had a level of care that could only be provided in the ICU setting at this hospital. This included new or escalating noninvasive mechanical ventilation, ingestion requiring continuous cardiac monitoring and hourly neurological checks, central line insertion with pressor therapy, and endotracheal intubation with invasive mechanical ventilation. One patient, resuscitated at an outside hospital ED, was pronounced brain dead after PICU admission. Seven patients admitted to the PICU did not require escalation of care upon arrival to the facility (9.6%).
Discussion
Telemedicine is being used in many new and exciting ways. Studies exploring pediatric telemedicine have been limited but are becoming more prevalent as use rapidly grows. A recent study by Yang et al. 7 explored the economic cost of pediatric telemedicine consultations in rural EDs, finding that telemedicine consultations are cost-effective and can reduce patient transfers compared with telephone consultations. Another recent study by Dayal et al. 8 used retrospective data from >500 children transferred from 15 EDs over a 4-year period and discovered that, after establishment of a telemedicine program, children arrived to the PICU with lower Pediatric Risk of Mortality (PRISM) III scores than before the implementation of telemedicine. Whether telemedicine ultimately impacted patient outcome, however, was not determined. 8 The study presented here is the first to analyze the effect of telemedicine on disposition and then explores hospital course after admission to a tertiary care, free-standing children's hospital.
Before its use at this institution, many NKTT transports were being re-evaluated in the ED. Through the use of telemedicine, there has been a decrease in ED utilization rate from 56.6% to 27.3%. Theoretical benefits in ED resource utilization include more available physical space and staff for other waiting patients, decrease in existing wait times, increase in ED throughput, avoidance of duplication of laboratories and studies, and a decrease in patient and insurance costs.
Specialty evaluation is slightly more complex. Fifty-eight patients were transported to the ED after telemedicine consultation and 14 patients (24.1%) were then discharged home shortly after ED evaluation. Of these 14, 7 patients required a pediatric specialty consultation, which the referral hospitals were unable to provide. This suggests that there is room for further improvement in telemedicine utilization. Using telemedicine in a way that links the MCO, pediatric specialist, and referral ED to discuss continuing care in the referral hospital setting could make many of these transports unnecessary, further decreasing excess healthcare waste. This has led the organization to begin transitioning from a one-to-one video connection to a platform that allows multipoint videoconference patient evaluation.
Current hospital policy also led to repeat evaluation in the ED. Trauma patients require initial evaluation in the ED before disposition elsewhere in the hospital. This policy derives from state trauma regulations, but it also offers rapid evaluation and flexibility if additional studies, such as computed tomography scanning or emergent operative management, are needed. Telemedicine can still help rule out isolated injuries that are advertised as trauma but do not require transport. It also gives the receiving team the most up-to-date condition of the patient with observation in real time, allowing lead time to prepare personnel and equipment for impending trauma arrivals.
Direct admission transport has been the subject of studies for many years, and various scoring systems, such as PRISM, transport Pediatric Early Warning Score, and Transport Risk Assessment in Pediatrics, have attempted to predict which patients would need higher levels of care. 9 –11 The ability to see the patient in real time makes these attempts at predictive scoring unnecessary. Telemedicine was useful in predicting those who needed definitive PICU-level care, particularly during periods of high census when ICU bed space is limited. The 9.6% of telemedicine patients admitted to PICU who were maintained on HFNC or continuous albuterol, modalities commonly found in the RIPCA, could be viewed as a failure to properly identify relatively “well” patients. However, the threat of decompensation at the time of telemedicine consult made it an acceptable tradeoff to admit to the PICU for observation rather than admit to the floor with a subsequent respiratory rapid response activation.
Twenty-four (40.7%) of 59 patients were discharged from the hospital 24 h or sooner after transport. This again suggests room for improvement in telemedicine transports. There may be several explanations for these findings. First, despite telemedicine consultation with an appropriate specialist, some ED physicians may be reticent to keep the patient locally for continued care. This may be due to lack of adequate inpatient admission areas or adequately trained staff for ongoing pediatric care, fear of patient decompensation, or fear of discharging an apparently stable patient with the possibility of return due to progression of illness. Despite the concern of unnecessary transport leading to increased cost and waste, travel burden on families, increased parental anxiety, and taxing of tertiary care resources, many geographically isolated referral EDs are uncomfortable with keeping pediatric patients. It remains to be seen whether education, additional training, and increased responsiveness to referral hospitals through telemedicine will change this culture. Transition from fee-for-service to value-based care, increased demands to maintain local care in medical homes, and advancement of telemedicine technology all may lead to a shift in the way care will be delivered in the coming years.
The rapid response rate remained the same pre- and post-telemedicine, whereas the code blue rate was 3 before telemedicine versus 0 with telemedicine, making it difficult to determine whether telemedicine made a distinct difference.
Potential cost savings provided by replacing unnecessary transport for telemedicine evaluation are not trivial. On average, in this geographic area, specialty care transportation by ground (e.g., NKTT) was estimated at 4,000 dollars. This accounts for pediatric trained personnel, equipment, fuel, and distance. Remote rural zip codes, which comprise the majority of NKTT transports and modality of transport needed (flight vs. ground), can double or triple the estimated figure. The move toward keeping care in local communities has merit but only if pediatric care can be provided in a safe and equal manner to that which would be found in transport to the tertiary care referral center. Telemedicine's impact on keeping care local has yet to be proven.
This study is limited by the fact that it was conducted at a single center. Expanding the study to additional facilities would strengthen the findings of this study. Another limitation was the retrospective nature of the review; thus, telemedicine consultations were not randomized. The MCO or outside emergency physician chose to use telemedicine based on the notion that the patient would require transport for additional care. Their preference to use the telemedicine tool may have potentially resulted in a bias for use in the more acutely ill patient, as seen by the lack of acuity level 5 transports.
There were a limited number of patients in the telemedicine group compared with the pretelemedicine group. This is partly because telemedicine was a new clinical program and only available at certain facilities. To date, the program has grown significantly to >35 hospitals with > 500 critical care transport consults. The pretransport data, however, were supported by > 4,000 patients over several years. A random selection of patients from the pretelemedicine cohort with similar acuity scores is being considered for further analysis.
In conclusion, this study demonstrates that telemedicine can be an effective resource for pediatric transports, and after telemedicine consultation, ED and PICU disposition patterns changed significantly. Further research to explore improved care coordination and subspecialty evaluation through telemedicine by taking advantage of multipoint videoconferencing applications is needed.
Footnotes
Disclosure Statement
No competing financial interests exist.