
Abstract
Background:
Close, multidisciplinary collaboration with burn experts is the essential strategy to achieve the best functional and esthetic outcomes in burn wound treatment. Management of minor burn injuries, where no specialized care is available, might be challenging. One concept to achieve a fast and timely result is the application of telemedicine. The objective of this study was to assess and develop a simple telemedicine protocol, which can be applied globally.
Material and Methods:
We present a pilot study based on a pediatric population of four patients with minor burns. Based on the severity and burn area, two cases of ambulant pediatric patients (mean 1% total body surface area, superficial and deep 2° burn) with minor burn injuries met study criteria and were enrolled. A pediatrician performed the initial assessment, followed by plastic surgery video consultation, using telephone's digital camera. Treatment protocols were designed to optimize outcomes. After the initial treatment phase, which took place at a nonteaching local hospital in Poland from January 1, 2014, to December 31, 2014, clinical follow-up was performed by a plastic surgeon via smartphone in the United States.
Results:
We have achieved complete burn wound resolution, in all patients, with no scarring and only minor discoloration. A simple, reproducible treatment protocol was designed to include dressing changes and additional outpatient visits
Conclusions:
Implementation of a telemedicine protocol allows for easy access to burn consultations, helps multidisciplinary collaboration, eases follow-ups, and shortens specialists' consult wait times. Real-time evaluation provides fast and flexible treatment, without long distance travels, for patients and their families. Telemedicine increases the frequency of follow-up, contributes to the esthetic outcome, and together with improved cost-effectiveness is beneficial for both the patient and healthcare system.
Introduction
In 2014, the World Health Organization (WHO) estimated 265,000 burn-related deaths globally. The vast majority of these fatalities occurred in low- and middle-income countries. In high-income countries, mortality from burns has steadily declined over the past 30–40 years, primarily due to the implementation of public health policies, education, availability of smoke detectors, and hot water temperature regulations. 1
The WHO Plan for Burn Prevention and Care for 2008–2017 consists of seven key factors: advocacy, policy, data and measurement, research, prevention, services, and capacity building. All of these factors are essential in helping to provide better and more efficient burn prevention and treatment, especially in developing countries and rural areas. 2 Regions with the highest mortality rates, South-East Asia (11.6 deaths per 100,000 per year), Eastern Mediterranean (6.4 deaths per 1,000,000 per year), and Africa (6.1 deaths per 100,000 per year) are of particular concern. In the European Union, burns and scalds are the fourth leading cause of child trauma. These occur mainly in toddlers under the age of 2 years. The main etiologies include hot water (25%), soup (24%), and coffee or tea (21%). 3 Current prevention strategies do not appropriately address the most common mechanisms of scald injury, requiring hospitalization. The goals should be prevention and, if necessary, close collaboration with other physicians such as pediatricians and pediatric surgeons. 4
In areas where no specialized burn consultations are available, even minor burn injuries can be problematic. 5 While minor wounds are not considered life-threatening injuries, they can cause major disfigurement. The poor esthetic outcome can be physically challenging and negatively affecting a child's future. 6 Other than the impact of disfigurement, which often results in social stigma, poor burn outcomes can lead to psychological impairment. Moreover, although difficult to quantify, scars can also affect the quality of patients' lives and their self-esteem. 7 There is a need to provide proper training in burn assessment for surgical specialists. 8
Most injuries require a professional consult followed by adequate debridement and dressing changes, which currently are provided mainly by the plastic surgeons or burn specialists. In many locations, medical facilities and specialist expertise are limited and burn victims need to be transported considerable distances to receive adequate care. The transportation process is time-consuming, expensive, sometimes unnecessary, and typically inconvenient and exhaustive, especially for young patients and their families. 9 In addition to educating nonburn physicians on how to evaluate and treat burns, plastic surgeons can benefit from implementing simple digital imaging devices to establish a multidisciplinary approach.
Taking the abovementioned into consideration, telemedicine could be, if basic Internet access is available, useful to start assessment and subsequent follow-ups, to achieve best functional and esthetic outcome. 10 Telemedicine, originally—Telediagnosis, a term coined in the 1970s, which means, “healing at a distance,” signifies the use of Information and Communication Technologies to improve patient outcomes by increasing access to care and medical information. 11 Even simple, cheap, cellular digital cameras can serve as a fast and efficient tool, giving both the treating physicians and their patients an opportunity to attain the best possible outcome. The implementation of telemedicine in the healthcare sector is a promising tool, especially in rural areas where no burn or plastic surgery specialized care is available. Furthermore, telemedicine has been noted to be efficient in the treatment of burn victims. It has been shown to be as effective in improving clinical decision-making, as face-to-face encounters. 12 However, few telemedicine protocols have been described or published to optimize esthetic outcomes so far.
While previous studies focused mostly on severe cases, in this study, we assess and provide a simple unified protocol for minor burns, including an emphasis on the esthesis.
Materials and Methods
Baseline Characteristics
As a plastic surgeon with experience in the treatment of burns, reconstructive and esthetic surgery, the first author of this study is familiar with the problems associated with long-distance consultations for adult and pediatric populations. Since a majority of minor burn injuries are underestimated and treatment plans poorly initiated, we devised a simple scheme based on digital photographs and an initial video consultation (Skype®, Microsoft®), including digital follow-up for minor burn patients in situations where no burn or plastic surgery consultations were otherwise accessible.
Inclusion Criteria
A minor burn was defined as a superficial burn to less than 10% of total burn surface area (TBSA) in adults and less than 5% TBSA in children.
Only pediatric patient populations, with minor, thermal burn injury, were included in this study. Electric or chemical burns or injuries involving the hand, foot, joint, genital, and perineal areas did not qualify for inclusion in the study (Table 1).
Study Criteria
× ≤ 5% in pediatric population; × ≤10% in adult population.
× > 5% in pediatric population; × >10% in adult population.
Aim of the Study
The objective of the telemedical evaluation was to implement a simple protocol to decide if inpatient or outpatient treatment is needed. Furthermore, the assessment of the entire treatment process, covering the follow-ups with the special focus on esthetic outcome, was evaluated.
Evaluation and Qualification
The first step was the utilization of a smartphone digital camera in the emergency room. After the image has been received, the body surface area and burn's depth were assessed. The assessment of burn wound area was based on Lund and Browder chart, and wound depth was based on the author's 10-year burn wound treatment experience. All the images were standardized in a simplified way; there was an only frontal view, over the wound area, forty centimeters from the injury, taken. All the photographs were executed in the series of three. If there was no need for inpatient treatment—no fluid resuscitation, intensive pain management, or operative procedures required, the entire wound healing process was managed via an online video consultation. We discussed the full videoconference-based treatment with the parents to develop a friendly and professional patient–parent–physician relationship. All drawbacks and limitations were discussed: when problematic and prolonged healing, uncontrolled pain, difficult physical therapy process, or uncertain esthetic outcome, reassurances were provided that in any complications outpatient follow-up would immediately be provided. Parents (or other family members) were instructed to document digitally all phases of the follow-up process. After a videoconference (Skype, Microsoft) and reviewing the digital images, we then formulated a treatment plan for monitoring. When using Skype software, the minimal bandwidth obtained was = 400 Kbps and maximal = 1.2 Mbps and the video resolution was = 720p. The second step of the telemedicine protocol, when qualified, was digital follow-up with the emphasis laid on the esthetic outcome and multidisciplinary collaboration.
From the initial group of four pediatric patients, we referred two patients to burn centers for further treatment. The other two patients qualified for a digital protocol implementation (Table 2).
Distributions of Burn Patients
Mean age and burn TBSA%.
TBSA, total burn surface area.
In these cases, on-site follow-up only occurred as part of the final consultation in the outpatient clinic. All patients were located in Poland, but the initial digital assessment and further follow-up were done in real time in Boston, Massachusetts. Data were collected over 12 months. Satisfaction rate was assessed by a simple three-question survey (0-dissatisfied, 1-neutral, 2-satisfied).
Results
After a thorough assessment of the initial digital images and with close collaboration with pediatricians from the small, urban nonteaching hospital, we determined that the first patient (Patient #1) did not present with any motion restriction in the affected limb and did not need further inpatient evaluation. Similar findings were observed in the second patient (Patient #2). All of the images were sent from a smartphone and assessed on a smartphone device (iPhone® Apple®).
For the two patients who qualified for burn referrals, we implemented outpatient treatment protocols (Fig. 1) with parental participation throughout the entire process.
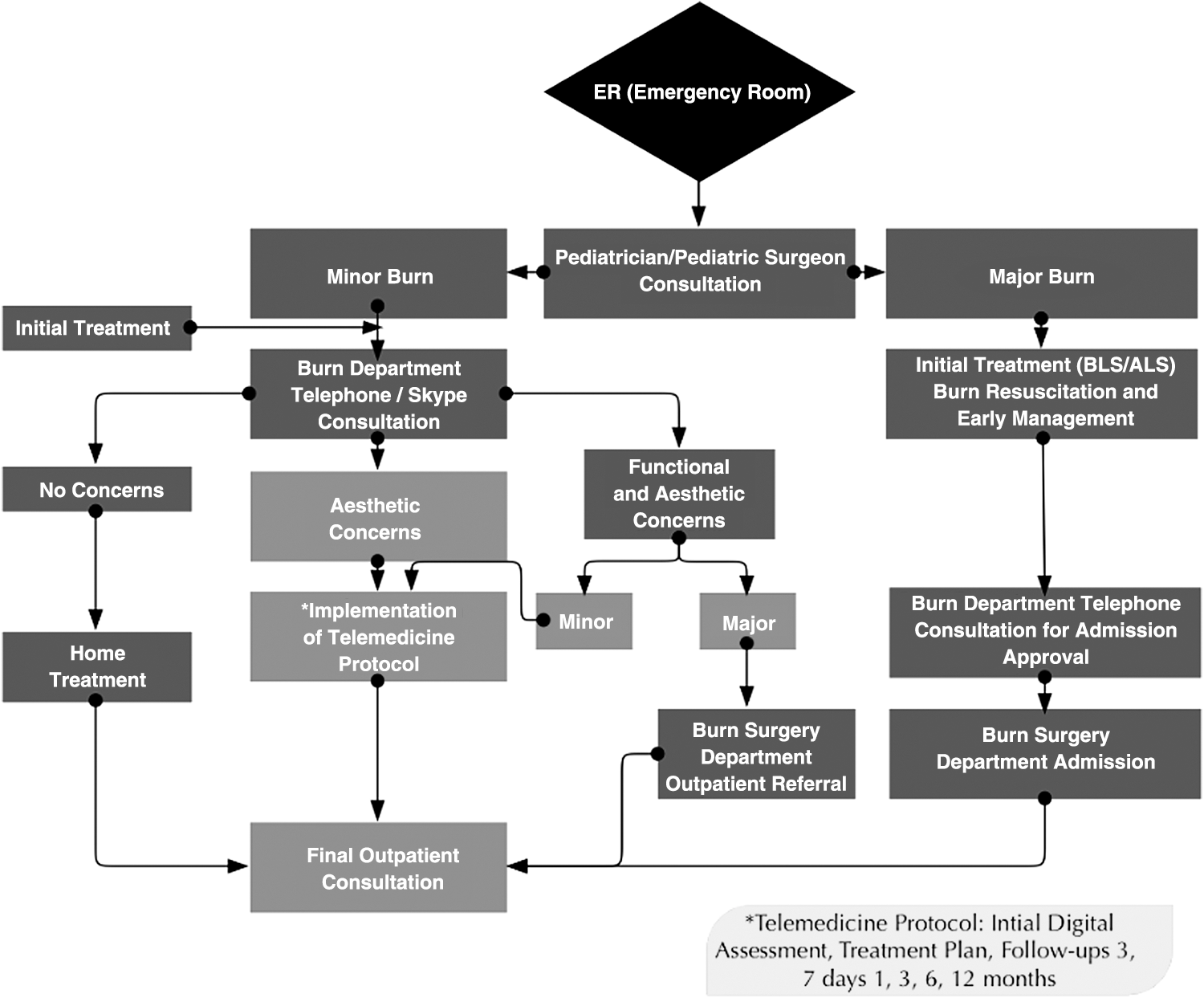
Telemedicine protocol algorithm.
Patient #1
A 2.5-year-old girl suffered a minor scald burn from hot coffee (2 min after preparation). The burn was classified as second degree; TBSA affected was 0.5%, on the right inner forearm (Fig. 2a). The patient was reported to be wearing a long sleeve cotton shirt and the time of liquid to body contact was about 20 s. Immediately following the accident, the wound was placed under cold tap water by her parent for 20 min, after which the family presented to the nearest pediatric emergency room. A pediatrician obtained a thorough medical history; all further burn consults were performed using a cell phone (Skype, Microsoft) utilizing a digital camera for imaging the burn. As there were no comorbidities, the patient qualified for the digital burns' protocol.

During outpatient treatment, therapy was initiated using AQUACEL® Hydrofiber® dressings, changed daily for the first 3 days. The healing process was uneventful and the hydrocolloid dressing Granuflex® was applied for the next 7 days (changed every third day) (Fig. 2b). On the 14th day of the treatment protocol, full wound closure was achieved. Subsequently, an ointment was initiated for the next 14 days, consisting of Alhydran® application five times daily and gentle massage for 5 min each time.
Video consultation was performed as necessary, and as the final step, burn scar massage and silicone dressings were advised for the next 12 months. The outpatient digital follow-up was scheduled for 3, 7, 14 days and then 1, 3, 6, and 12 months after the initial trauma. The patient's family was instructed to protect the injured area, from sun exposure (minimum sun protection factor [SPF] 20–25), up to 12 months. The esthetic outcome of the treatment was satisfying and received with high parental satisfaction (Fig. 2c).
Patient #2
A 3.5-year-old boy suffered from minor scald burns from hot tea immediately after preparation. The burn was classified as second degree; TBSA affected was 2% on the right, central torso, and neck (Fig. 3a). The patient was wearing a cotton t-shirt; the time of liquid to body contact was ∼30 s. The wound was placed under cold tap water for 20 min following the accident. An on-site pediatrician obtained a thorough medical history. During outpatient treatment, the family was concerned about the final functional and esthetic outcome, and thus, a plastic surgery video consultation (Skype, Microsoft) was scheduled. All clinical data were obtained over the phone. Since the patient lived in the countryside, far from the nearest burn center, and had no comorbidities, the patient qualified for the digital protocol.
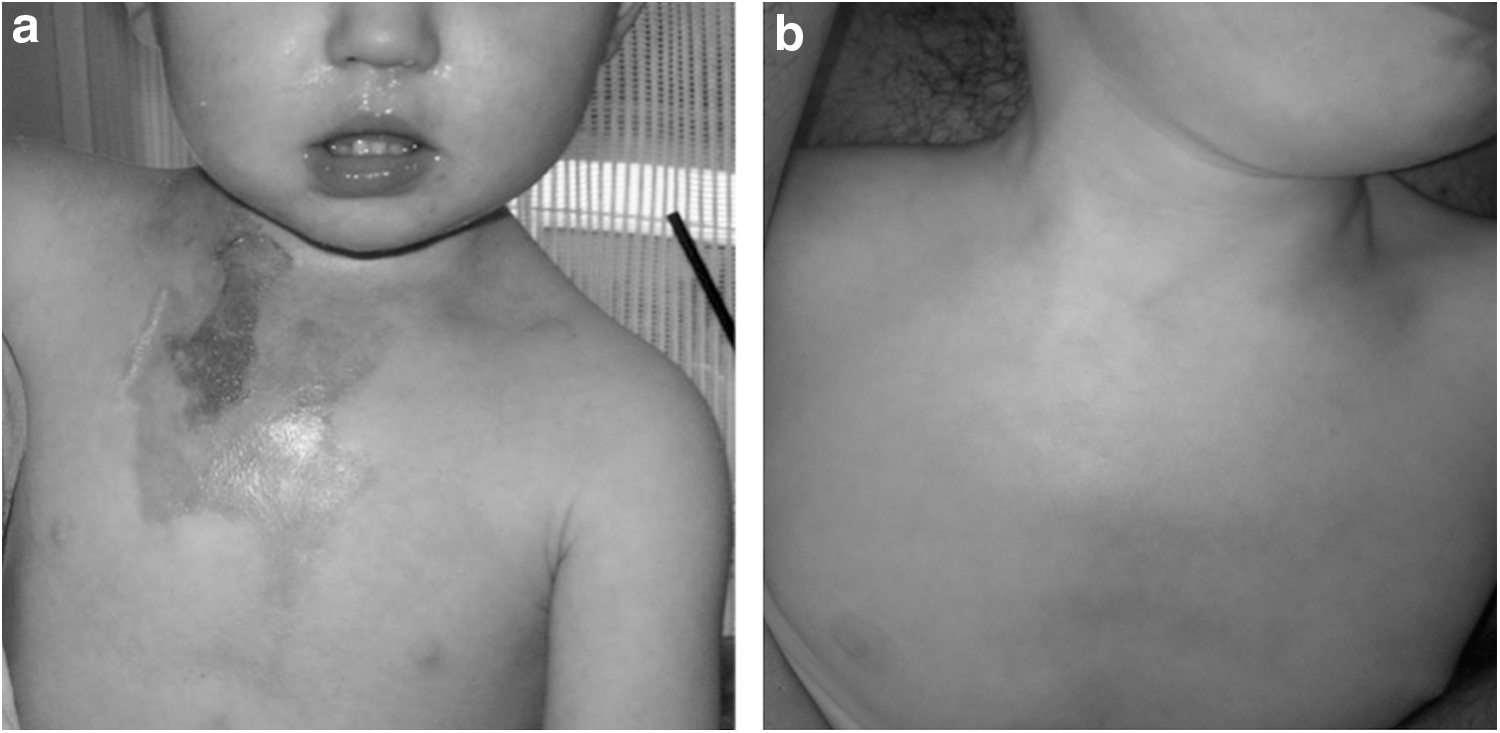
The wound treatment protocol was implemented. AQUACEL Hydrofiber dressings were changed daily for first the 3 days, with Alhydran ointment on the wound borders. Healing was uneventful, and the hydrocolloid dressing Granuflex was applied for the next 7 days (changed every third day). On the 19th day of the treatment, full wound closure was achieved. An ointment was initiated for the next 14 days using Alhydran, which was applied five times daily with delicate massage for 5 min. As a final step, burn scar massage, Granuflex Extra Thin and Alhydran application dressings were performed for the next 12 months. Alhydran and Granuflex Extra Thin were also used under a compression garment, instead of silicone dressings. Outpatient digital follow-up was scheduled for 3, 7, 14 days and then 1, 3, 6, and 12 months after the initial trauma. The patient's family was instructed to protect the injured area from sun exposure (minimum SPF 20–25) up to 12 months. The treatment outcome was graded satisfactory with a high parental satisfaction rate (Fig. 3b).
Discussion
Over 70% of burn patients are children, where more than 55% of burn injuries occur in boys. 13 In the two cases presented, complete wound closure was achieved within 21 days, diminishing the likelihood of hypertrophic scarring. 14 By collaborating with pediatricians and the patients' parents, and utilizing an easy and reproducible digital follow-up protocol (using the family's cellular digital camera), the burn treatment team was able to achieve excellent results in presented cases. In the process of treating the burn wounds and using the digital protocol, we avoided unnecessary travels expenses, long waits, and stressful physical examinations in the hospital setting. Our digital protocol was easy to implement, cost-effective to both the families and the healthcare system, achieving a good esthetic outcome (Fig. 1). We agree that the addition of video to enhance standard static telemedicine, as presented by Wibbenmeyer et al., helped to communicate with the specialists and patients more effectively. 15
In the grand scheme of medical practice, telemedicine is not a novel concept. Gardner et al. stated in 1990 that telemedicine is an important tool for an around-the-clock hospital specialist to provide necessary consults. 16 As physicians, we should be open to the numerous applications of telemedicine, especially given the many technological breakthroughs and continued evolution in the field. This concept has been previously implemented for burn consultations in severe burn cases, as mentioned by Ajami and Arzani-Birgani. The authors reported that acute evaluation of burn patients can be managed by telemedicine and that it plays an important role in improving access to prompt expert consults. 17 While this study introduced the concept and utilization of video consultation and digital follow-up, it did not provide a protocol that could be used in cases involving minor burns assessing final esthesis.
Wibbenmeyer et al. showed one of the similar approaches we presented. 15 They incorporated a structured system for telemedical patient consultation and further treatment. The authors compared the videoconference-enhanced model with telephone protocol only and found that the use of their system, despite not quantitatively assessed, may cause a decrease in healthcare costs associated with the addition of video to a telephone-only transfer program. In this study, we present a combination of the static and live video stream. Those models presented similarly. Nevertheless, we focused on the minor burn treatment and intensive follow-up with the emphasis laid on the functional and esthetic outcome.
The capabilities of telemedicine applications are continually advancing. In 2014, Godwin et al. presented a novel mobile software that provides a straightforward, and interactive Lund and Browder diagram for automatic calculation of total body surface area, which includes fluid formula recommendations and serial wound photography on a single platform. 18 The idea of handheld-based software established the foundation for further development of other smartphone and now even smartwatch (iWatch, Apple, Gear S3, Samsung®) applications for the assessment of burn injuries. A few examples include the BurnMed (Johns Hopkins University), Mersey Burns applications, and BurnCase 3D. They can facilitate quicker and more accurate burn wound evaluations when comparing to standard clinical assessment only. 19 –21 As presented by Parvizi et al., a combination of clinical knowledge and software evaluation can have a true impact on the quality of treatment. 22 The next steps of treatment ladder will be a routine implementation of mobile device protocols and their subsequent validation to become a daily practice. 23
Telemedicine is being partially utilized to coordinate care between multidisciplinary clinical personnel and patients in remote and rural locations. 12,24 This was also our experience when we used easy-to-work digital protocols, for better burn assessment, and shared video consulting platforms such as Skype Microsoft, for further clinical follow-up. Our digital concept due to the ease, cost-effectiveness, and feasibility might prove a useful tool in countryside locations that have not yet been able to take advantage of previous, more expensive technologies. 25
Our study suggests that even simple cellular phones or more sophisticated smartphones, phablets, and tablets are an ideal way for “digital protocol” implementation. 26 When utilized appropriately, this form of e-consultation provides a cheaper alternative in ways of transportation to the specialized burn centers, and a detailed, remote follow-up is cost-effective from the society and healthcare system perspective. 27
New research on the devices such as Google Glass® (Google), or in a short perspective HoloLens® (Microsoft), appears to be promising for possible telemedicine clinical applications. 28,29 As telemedicine evolves, increased utilization of digital imaging, video consultation follow-up, and augmented reality devices may prove useful tools for patient care. Surgical professionals might benefit from the development of software applications, especially in collaboration with software programmers and information technology specialists, to provide better treatment globally. It was demonstrated by Wurzer et al. that even freeware software application can give an objective burn wound estimation leading to better patient care. 21
A possible telemedicine restriction would be in cases where real, on-site consultations are needed for patients whose psychological burden cannot be addressed through virtual consultation.
Conclusions
This study provides insight into our initial experience using the digital protocol in the treatment of minor burns with the esthetic outcome assessment. Implementations of a telemedicine protocol allow easy access to burn consultations, follow-up clinical encounters, and shorten specialists' consult waiting time. Real-time telemedicine evaluation allows fast and flexible treatment without long-distance travel for patients and their families, based on multidisciplinary approach. Videoconference-based assessment and treatment increase the frequency of follow-up and combined with improved cost-effectiveness are beneficial for both patients and healthcare systems.
Limitations
We know that the described protocol is not free from limitations. One of them, when used in rural regions, might be the lack of professional dressing. Even though standard moisture dressings, such as gauze, were applied, telemedicine would still provide better wound control, a proper treatment qualification, and accurate follow-up. Another concern was network security since the highly confidential patient information was being transmitted. This problem was nonexistent when Skype, Microsoft software, was used, as it utilizes the advanced encryption standard (AES). 30 As presented in 2016 by Wallis et al., a well-structured cloud consultation system is safe and efficient when used in the burn evaluation process. 31
We know that the protocol, based on the pilot study, may be improved when a higher number of patients are evaluated. We are also going to perform further assessments to eliminate all the drawbacks for patient's safety and future ease-of-use. We would like to emphasize that the patients' safety was our primary goal. In the case of any unusual complications, parents and legal guardians were informed to contact a supervising physician directly. Although the above situation did not occur, we developed a standard protocol for emergent situations.
Footnotes
Acknowledgment
We thank Kuzniacka A., MD, Department of Pediatrics, Oncology and Pediatrics Center, 7 Truchana, Chorzow, Poland, who participated in this study as a consulting pediatrician. Ethical Approval: The patient information in this study is deidentified.
Authors' Contributions
All the authors listed contributed to the study design, interpretation of data, and article preparation for final submission.
Disclosure Statement
None of the authors has a financial interest in any of the products, devices, drugs, or procedures mentioned in this article.