
Abstract
Introduction:
Recent research indicates that mindfulness-based interventions are effective for stress, maladaptive weight-related behaviors, and weight loss. Little is presently known about their applicability and effectiveness when delivered electronically, including through Web-based and mobile device media. The primary aims of this review were to identify what types of electronic mindfulness-based interventions have been undertaken for stress, maladaptive weight-related behaviors, and weight loss, and to assess their overall effectiveness.
Methods:
A systematic search of PubMed (MEDLINE), Embase, CINAHL, and Web of Science databases was undertaken in June 2016.
Results:
A total of 21 studies were identified that met inclusion criteria and were selected in the final review. Of these, 19 were mindfulness-based interventions for stress reduction. Two were Web-based mindful eating/intuitive eating interventions for weight. Only one electronic mindfulness-based study was identified that targeted both stress and maladaptive weight-related behaviors. Most electronic interventions were effective for stress reduction N = 14/19 (74%). There were insufficient electronic mindfulness-based interventions for weight to determine if they were effective or not. Additionally, no mobile mindfulness-based intervention was identified for weight or weight-related behaviors.
Conclusion:
Electronic mindfulness-based interventions through diverse media appear to be effective for stress reduction. More studies are needed that target weight and weight-related behaviors as well as studies that target both stress and weight. More randomized controlled trials (RCTs) that assess mobile mindfulness-based apps are needed as we only identified four app trials for stress. Mobile mindfulness-based interventions for weight and weight-related behaviors are a future area of research novelty.
Introduction
Overweight and obesity are major global risk factors, putting affected individuals at greater risk of chronic diseases such as cardiovascular disease, diabetes type II, and premature mortality from heart attacks and strokes. 1 –3 Developing effective novel interventions that may target overweight and obesity is greatly needed to prevent these complications. The prevailing literature has linked maladaptive weight-related eating behaviors, such as unhealthy dietary intake, binging or emotional eating, and lack of sufficient physical activity related to stress. 4 –16 There has also been a breadth of research that suggests a likely mechanism is stress, which increases cortisol, which leads to adiposity, 17 –19 as well as mood issues with a postulated stress eating reward pathway. 20
Recent research indicates that mindfulness may hold potential for targeting psychological stress, maladaptive weight-related behaviors, and weight. 21 –23 Mindfulness refers to a state of higher awareness of the present moment through focusing one's thoughts on the present reality, breathing attentively, and not focusing on any judgmental thoughts or worries which may deter one from being present. 24 Mindful eating involves focusing on the process of eating through heightened attention to one's olfactory and salivary senses as well as the mechanical process of chewing food, while attuning oneself with one's internal cues by ceasing to eat immediately when full. 25
Given that mindfulness has been found to be effective for stress reduction and weight loss, 21 –23 its application for stress-induced emotional eating and weight gain appears promising. One hypothesis for the possible relationship between mindfulness, stress, and weight is that mindfulness enhances emotional coping mechanisms in response to stress such as engaging in maladaptive weight-related behaviors associated with weight gain. 26 –29 Support for stress as a mediator in the relationship between mindfulness, weight, and weight-related behaviors has been found in some recent studies. 30
While recent reviews have found support for mindfulness-based interventions for stress reduction and weight/weight-related behaviors through group in-person counseling sessions, 21 –23 it is presently unknown whether these interventions are effective when delivered through electronic media. In recent years, electronic health and m-Health have been used for psychological interventions 31 and weight-related behavior change interventions. 32 Electronic mindfulness-based media have recently begun to emerge as new methods for delivering various health and psychological interventions. 33 The benefits of electronic interventions, in particular m-Health, include their increased accessibility and portability at any time and place. 34
There have been two reviews of online mindfulness-based interventions for depression, anxiety, and stress. 35,36 Although Fish et al. reviewed mindfulness-based interventions for mental health, including broad electronic interventions, five of their studies were only specific to stress and were all Web-based. 35 Other reviews explored commercial mindfulness-based apps, finding that few employed mindfulness-based techniques 37,38 and that there is insufficient evidence regarding their effectiveness for increasing mindfulness and for assisting with various health conditions. 38
Furthermore, to date, there has not been a review on electronic mindfulness-based interventions for weight/weight-related behaviors as well as interventions that target maladaptive weight-related behaviors and stress in nonclinical populations.
The goal of this review is to identify the types of electronic mindfulness-based interventions (both stationary and mobile) that have been conducted to date for weight, weight-related behaviors, and stress and to understand their overall effectiveness. Additionally, areas of research novelty that may inform future electronic mindfulness-based interventions in the stress, weight, and maladaptive weight-related behavioral fields will be examined.
As this is an emerging area of research, we anticipated that there would be very little if any mindfulness-based approaches for weight and stress. For this reason, we kept the inclusion criteria broad to also include electronic mindfulness-based stress reduction (MBSR) interventions even if they did not target diet or weight to better understand what has been done electronically and to inform the development of a MBSR intervention that utilizes stress reduction techniques targeted at both weight loss, maladaptive weight behaviors, and stress.
Methods
Databases Searched
A systematic search of PubMed (MEDLINE), Embase, CINAHL, and Web of Science databases was undertaken in June 2016.
Search Terms
The search terms for intervention content were: mindfulness or mindful eating or intuitive eating or mindfulness-based cognitive therapy or ACT or acceptance and commitment therapy, and dialectical behavior therapy. The search terms for intervention media were: electronic, online, Web-based, mobile phone, mobile health, m-Health, app, smartphone, personal digital assistant (PDA) computer, laptop, text message, SMS and intervention, randomized controlled trial (RCT), and trial. The search terms for outcome were: weight, weight loss, weight gain prevention, body mass index (BMI), obesity, waist circumference, diet, binge eating, emotional eating, physical activity, and stress reduction. Word variations were searched and truncation was used where appropriate. The search strings were combined into one large search string. Details of the search criteria for each database are summarized in Table 1 below and the inclusion and exclusion summary criteria that follow.
Search Strategy Example: Embase
BMI, body mass index; PDA, personal digital assistant.
Inclusion criteria
• Electronic mindfulness-based interventions for stress reduction or weight loss/weight-related behavior change (or both), including Web-based/online (nonmobile) and mobile such as mobile apps, mobile text messages, PDAs, and iPods/podcasts.
• Electronic interventions consisting of mindfulness audios (CDs or online) were included if the main component of the intervention was electronic
• Healthy adults >18 (those with depression/anxiety included if subclinical or general)
• Studies published in the English language
• Must have either measured stress or weight as the primary outcome or both
Exclusion criteria
• Observational nonintervention-based studies
• Meditation studies that did not measure mindfulness levels or use a mindfulness-based intervention approach
• Studies that assessed psychological primary outcomes other than stress such as wellbeing or happiness
• Studies published in languages other than English
• Interventions in adults with clinical illness/comorbidity such as cancer or stress interventions for pain
• Studies in adults with major psychiatric illness/acute episode (bipolar or schizophrenia) other than general/subclinical anxiety/depression
• General well being/mental health promotion studies that did not assess stress
Screening
Titles were screened for relevancy to the research question, followed by abstract screening of relevant articles against the inclusion and exclusion criteria. Two reviewers (L.N.L. and L.C.) screened the abstracts against the inclusion and exclusion criteria. Where there was disagreement, the reviewers discussed their reasons until an agreement was reached. Abstracts meeting the inclusion criteria were screened at full text. Full text articles meeting the inclusion criteria were included in the final review along with any additional articles generated from hand, manual, and Web searches of the gray literature and article references.
Data Extraction
Data on study characteristics were extracted, including location, sample size, gender, duration, methods, and measures. Data were also extracted on electronic intervention components used and mindfulness-based techniques used. Outcome data on weight, weight-related behaviors, and stress changes were also extracted.
Appraisal
Studies were appraised using a set of adapted criteria from the Cochrane risk of bias grading tool, which included a consideration of selection bias, attrition bias, and detection and treatment biases. 39 The key domains that were assessed were randomization, allocation concealment, blinding of participants and study personnel, retention, and a whether an intention to treat analysis was undertaken. In addition to this, the validity and reliability of measures and a priori sample size calculations were added as criteria. Study duration was also added, with studies longer than 12 weeks receiving a strong score, 8 weeks moderate, and less than 8 weeks were scored as weak for this domain. All domains were assessed on a yes or no basis, with a weak score given for each domain that was not ticked as “Yes.” Very high-quality studies met all of the key domains. High-quality studies did not have more than one weak score (No/Not clear) in a single domain and met all the other domains (Ticked off as “Yes”). Moderate-quality studies had no more than three weak domains out of eight, whereas weak studies were graded as scoring low on 4 or more domains out of 8. The appraisal scores are in the appendix.
Results
The search generated 1,054 titles. Details of the search process and reasons for exclusion at each stage are summarized in the flowchart in Figure 1. The total number of full text articles meeting inclusion criteria that were included in the final review was 21. 40 –60
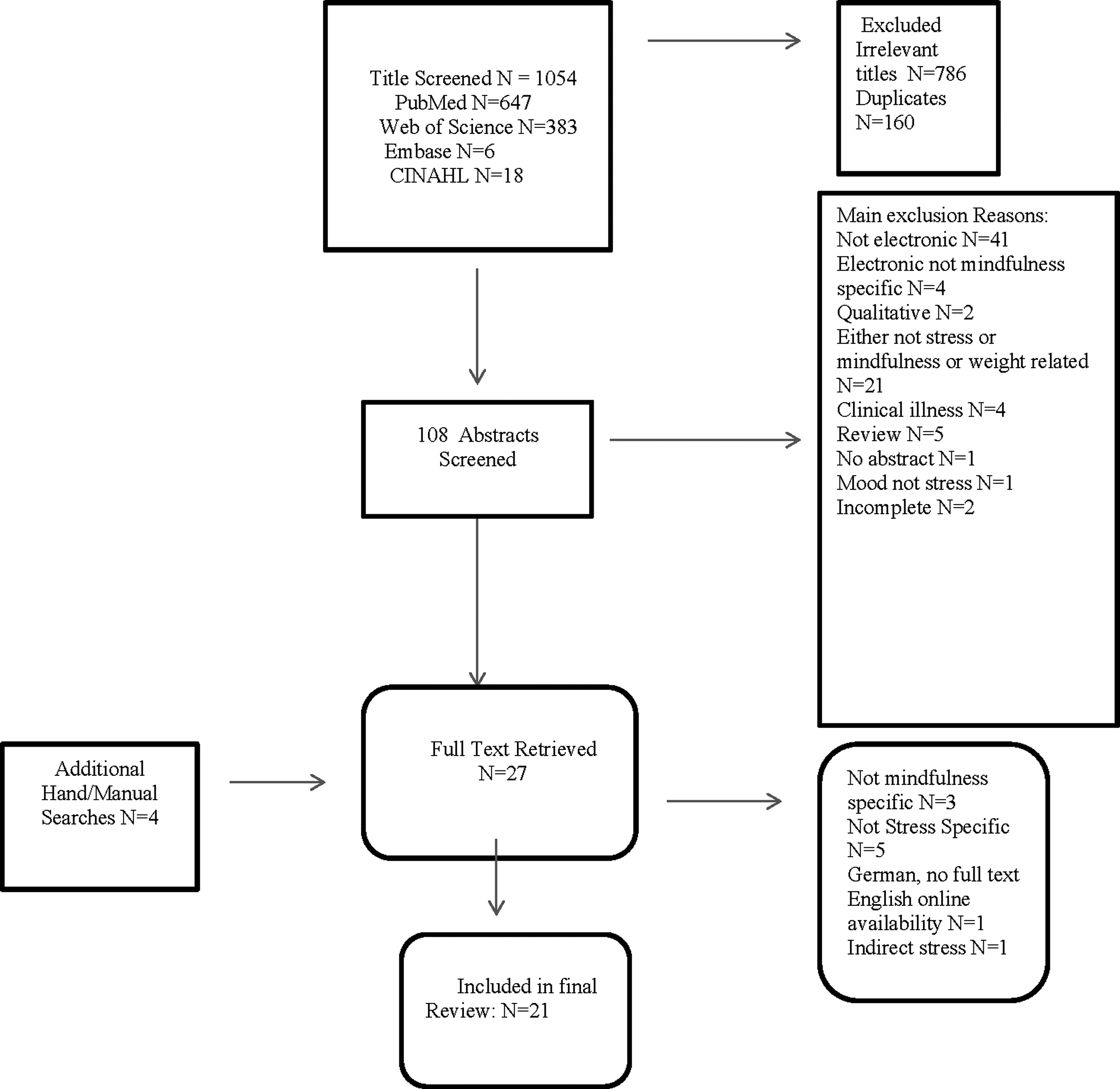
Flowchart.
Study General Characteristics
Study general characteristics are summarized in Table 2. Of the 21 included studies, the majority were electronic mindfulness-based interventions that targeted stress. 40 –60 Additionally, one of these included studies targeted both stress and weight-related lifestyle behaviors. 41 There were two studies that targeted weight. 43,48 The study sample sizes varied from 2659 to 32153 participants. Study duration ranged from 245 to 14 weeks. 43 The study with the largest age range was from 18 to 79 years of age, 54 with the remainder of the studies having sample ages within this range. Two studies had only female participants. 48,56 Study locations included the United States, 41,42,48,49,51,54,57,58 Finland, 40,55,58 the United Kingdom, 45,50 Australia, 60 New Zealand, 43 Sweden, 52 Italy, 44 China, 53 Ireland, 56 Switzerland, 47 and Norway. 46
Study Characteristics Electronic Mindfulness Trials for Stress Reduction and Weight Loss
ACT, acceptance and commitment therapy; FFMQ, Five Facets of Mindfulness Questionnaire; ITT, intention-to-treat analysis; MAAS, Mindfulness Attention Awareness Scale; PSS, Perceived Stress Scale; RCT, randomized controlled trial.
Electronic Content and Mindfulness Techniques
The electronic intervention media most often were Web based across the stress reduction interventions 41,42,45 –47,50,54,58,59 and mindful/intuitive eating interventions for weight. 43,48 Four interventions used mobile electronic media consisting of mindfulness stress reduction apps, 40,44,45,52 one of which also used app features that enabled therapist messaging. 52 Three interventions utilized mindfulness audios as intervention media consisting of mindfulness meditation and instructions. 53,57,60 Seven interventions were multicomponent interventions that combined different components such as written materials (diaries, instructions) with components such as videos and audios. 42,45,46,50,54,55,59 The mindfulness techniques that were integrated into the electronic media often included MBSR techniques adapted from Jon Kabat Zin's MBSR program such as yoga, body scans, breathing exercises, and sitting, as well as walking meditation demonstrations. 41,47,49,50,56,57,59 Although the most common mindfulness-based approach adopted was MBSR, five studies informed their interventions by acceptance and commitment therapy (ACT). 40,51,52,55,58
Electronic Interventions for Stress
Fourteen out of 19 electronic mindfulness-based stress interventions were effective for stress reduction. 40 –42,45 –47,49,50,52,54,57 –60 However, in one of the studies, stress was reduced postintervention in the intervention group. 46 Five studies did not find that the intervention significantly reduced stress. 44,51,53,55,56 A stress reduction app trial found that among those who adhered to the intervention, stress was reduced. 55 However, barriers relating to participant time management and having to login to the app resulted in low adherence. 55
Electronic Interventions for Weight and Weight-Related Behaviors
Two electronic mindfulness-based interventions for weight were identified that were Web based and adopted mindful or intuitive eating techniques. One found that an intuitive eating Web-based intervention increased intuitive eating in mid-age women, but did not result in significant reductions in BMI at 16 weeks. 43 The other intervention in college students utilized mindful eating as one component of a multicomponent intervention delivered through an online learning site (Blackboard). The intervention was not guided by mindfulness, but by social cognitive theory. It found reductions in BMI in intervention participants receiving e-mails in addition to the Web-based component. 48
Electronic Interventions for Stress, Weight, and Weight-Related Behaviors
One electronic mindfulness-based intervention was identified that targeted weight-related eating behaviors such as dietary intake, eating behaviors, or physical activity in addition to stress using MBSR, 41 which was partly described earlier under Electronic Interventions for Stress. The intervention found promising results not only for stress described earlier, but also healthy eating behaviors, including reduced fast food consumption and an increase in fruit and vegetable intake in participants. 41
There were no electronic mindfulness-based interventions that targeted both stress and weight or that utilized MBSR or stress reduction techniques for weight loss specifically.
Study Quality
Study quality is summarized in Table 3. Overall, some studies were graded as being of moderate quality, 42,46 –48,51,52 whereas the remainder received overall weak scores. 40,41,43 –45,49,50,53 –59 Only one study received a strong overall score. 60 Twelve interventions (80%) received a strong score for using a RCT design. 41,42,44 –46,48,51 –54,56,58 The majority of interventions received a strong score for using valid and reliable instruments. 41,42,45,46,48,51,53,57,58 Eight studies had weaker scores in the attrition domains with attrition ranging from 30% to 50%. 42,45,46,49,53 –56 Several interventions received a strong score for using an intention to treat analysis (ITT) protocol (75%). 41,42,45,46,48,51 –53,58 A few interventions performed sample size calculations 42,51,52,54 and resultantly received strong scores for this domain. The interventions also received weaker scores in the blinding of participant or study personnel domains. The majority of interventions received weak scores for allocation concealment.
Intervention Scoring Partly Adapted from the Cochrane Risk of Bias Scoring Criteria Domains
Randomization yes/no (no = weak), allocation concealment yes/no (no = weak), assessors/participants blinded yes/no (no = weak), Intention-to-treat analysis yes/no (no = weak), sample size yes/no (no = weak), valid/reliable data collection yes/no (no = weak). Study duration 12 weeks = strong 8 weeks moderate <8 weeks = weak. Overall Score very strong (VS) = no weak domains strong (S) = 1 weak domain moderate (M) = 2–3 weak domains weak (W) = 4 weak domain.
Discussion
The results of this review suggest that overall mindfulness-based interventions delivered through diverse electronic media, including Web-based, mobile app-based, and audio are effective for stress reduction. Web-based interventions far outnumbered mobile app interventions for stress reduction as we only identified four app trials for stress reduction. Thus, there is a need for more MBSR app trials in the future.
Additionally, we only identified two studies that integrated a mindfulness-based component to a weight loss study, which involved mindful/intuitive eating. 43,48 While the multicomponent intervention which integrated mindful eating in an online learning site as one component found reductions in BMI, 48 the latter Web-based intuitive eating intervention did not. 43 Based on this very limited number of studies, we were unable to assess their overall effectiveness. Thus, this is an emerging area of research that requires further exploration in future randomized controlled trials. As there were only two interventions that used mindfulness-based eating approaches, it is unknown whether other types of mindfulness-based approaches are effective and feasible when delivered electronically for weight loss. It would be of research interest to explore if other mindfulness-based approaches, such as MBSR or ACT, may be effective for weight loss when delivered electronically.
In addition to this, we only found one study that utilized a mindfulness approach (MBSR) that led to increased dietary intake and reduced fast food intake, and one study, described above, targeted eating behaviors through intuitive eating approaches which led to increased intuitive eating. 43 Given that the prevailing literature suggests that mindfulness may assist with these lifestyle behaviors, particularly eating behaviors such as emotional eating and binge eating, 22 there is a need for studies to explore if these interventions may be delivered successfully through an electronic medium.
Given that stress is associated with maladaptive weight-related behaviors 4 –16,61 and it may act as a mediator in the relationship between mindfulness and weight, 30 future interventions should target both stress and maladaptive weight-related behaviors. We only found one electronic mindfulness-based intervention that targeted both stress and maladaptive weight-related behaviors using MBSR. 41
As research indicates that mobile health is effective for weight loss, 32 and there is a rapid take up of apps for weight loss, it is timely to evaluate whether mindfulness-based approaches delivered through the mobile medium may be effective for weight loss alone and in conjunction with traditional behavior change techniques used in these m-Health weight loss interventions. 32,62 We did not identify any trials that have assessed the effectiveness of mobile mindfulness-based apps for weight loss despite the fact that there are commercial apps. Importantly, future investigations should adopt a randomized controlled trial design to assess the effectiveness of these mindfulness apps for weight loss as currently their effectiveness is unknown. Other mobile phone features could also be explored as well as the use of other mobile devices such as iPods.
Quality
While some studies were of moderate quality, many were weak overall. The domains that could, in particular, be improved include increasing retention as well as explicit methods of allocation concealment and blinding of study personnel. Future research should be adequately powered by conducting a priori sample size and power estimates. Finally, not all studies assessed mindfulness. It is also important to assess the mechanism of change and whether the intervention increased mindfulness, something raised in a previous review of mindfulness interventions in the general adult population. 23
Strengths and Limitations
A strength of this review is that we reviewed four databases for diverse electronic media, including Web-based and mobile interventions and assessed their effectiveness for both stress and weight. We identified an area of novelty research that requires further exploration and proposed new emerging research possibilities through linking the fields of m-Health, mindfulness, and weight. While we systematically searched four databases, there is always a possibility that some studies may have been missed.
Conclusion
In summary, this was the first review to examine electronic mindfulness-based interventions for weight, weight-related behaviors in the field along with being one of the first review to thoroughly explore mindfulness-based e-interventions using diverse media for stress. Mindfulness-based interventions appear to effectively assist with stress reduction. It also appears that mindfulness-based interventions for weight may be delivered electronically, but due to the very few studies identified, we were unable to draw conclusions on their overall effectiveness. To date, there has not been a mobile mindfulness-based intervention for weight loss. It is time for the fields of m-Health for weight loss and mindfulness to unite as a new research area, which may be referred to as “mobile mindfulness-based interventions for weight,” MMBIW through novel research in this field of possibilities.
Footnotes
Acknowledgments
The authors would like to thank medical librarian at UQ Lars Erikson for his advice with the searches. Funding was provided by the UQ Centennial Scholarship and Australia Research Training Scheme Scholarship.
Authors' Contributions
All authors contributed to the article. L.N.L. and L.C. screened the articles against the inclusion and exclusion criteria and appraised the studies. S.E. and M.B. assisted with the article development and approved the final version. Contributions included peer review of abstracts, study appraisal, development of the article, and final approval.
Disclosure Statement
No competing financial interests exist.