
Abstract
Background and Introduction:
Delivering care through telemedicine directly into the patient's home is increasingly feasible, valuable, and beneficial. However, qualitative data on how patients' and physicians' perceive these virtual house calls are lacking. We conducted a qualitative analysis of perceptions of these visits for Parkinson's disease to (1) determine how patients and physicians perceive virtual visits and (2) identify components contributing to positive and negative perceptions.
Materials and Methods:
Qualitative survey data were collected from patients and physicians during a 12-month randomized controlled trial of virtual house calls for Parkinson's disease. Data from 149 cases were analyzed using case-based qualitative content analysis and quantitative sentiment analysis techniques.
Results:
Positive and negative perceptions of virtual visits were driven by three themes: (1) personal benefits of the virtual visit, (2) perceived quality of care, and (3) perceived quality of interpersonal engagement. In general, participants who identified greater personal benefit, high quality of care, and good interpersonal engagement perceived visits positively. Technical problems with the software were commonly mentioned. The sentiment analysis for patients was strongly favorable (+2.5) and moderately favorable for physicians (+0.8). Physician scores were lowest (−0.3) for the ability to perform a detailed motor examination remotely.
Discussion:
Patients and providers generally view telemedicine favorably, but individual experiences are dependent on technical issues.
Conclusions:
Satisfaction with and effectiveness of remote care will likely increase as common technical problems are resolved.
Introduction
Chronic conditions benefit from specialist care and regular follow-up. 1 However, access to specialist care is often limited by distance, distribution of physicians, and patient disability. 1 –4 In recent years, virtual house calls have emerged as a potentially feasible alternative to office visits, with evidence of similar efficacy and high levels of satisfaction expressed by both patients and physicians. 5 –8
While it is known that patients and providers generally like telemedicine, 5 qualitative data on what motivates perceptions of virtual visits are lacking. 8 Implementation theory suggests that perceptions can serve as facilitators or barriers to the uptake of new technology and affect adoption of new approaches to care. 9,10 Thus, understanding how patients and providers perceive virtual visits is critical to wide-spread implementation. 10 To date, most research in telemedicine has focused on feasibility and efficacy of novel devices, remote monitoring, or site-to-site telemedicine consultation. 11 Only seven studies have explored videoconferencing delivered by physicians to patients at home. 12 –20 Furthermore, qualitative data on the patients' or providers' perceptions of these home virtual visits are almost entirely lacking. 21 Therefore, we conducted a qualitative study of patients and physicians during a randomized controlled trial to (1) determine how patients and physicians perceive virtual visits, and (2) identify components contributing to positive and negative perceptions.
Materials and Methods
Trial Design
As described previously, we conducted a 12-month randomized controlled trial to compare usual care with usual care augmented by four virtual visits with a Parkinson's disease specialist delivered directly into the home. 5,22,23 Internal review board approval from all participating sites and subject consent was obtained. A total of 20 physicians (Parkinson's Specialists) participated in the study. A total of 195 patient participants were randomized across 18 research sites. Individuals were randomized 1:1 to (i) usual care in the community (control) or (ii) usual care plus four virtual visits with one of the specialists. The control group optionally received a one-time virtual visit after study completion. Virtual visits consisted of a remote consultation with a Parkinson's disease specialist through secure videoconferencing. Most patients and physicians had no prior telemedicine experience. Visits consisted of patient history, Parkinson's-specific examination, and treatment recommendations. After each visit, patients and specialists completed an online survey with five open-ended questions (Table 4).
Analyses
Quantitative study findings of satisfaction with virtual house calls are published elsewhere. 5 For the qualitative analyses, two techniques were used: (1) case-based qualitative content analysis and (2) quantitative sentiment analysis.
Case-based qualitative content analysis
Case-based qualitative content analysis techniques allow for a more contextualized examination of responses. 24,25 Cases were defined as the total feedback from a patient–physician pair. Feedback was received for a total of 149 cases, with between 1 and 4 visits per case. Individual responses were placed into matrix form with rows representing a single visit (n = 399) and columns representing patients' or physicians' responses to the five open-ended survey questions (Table 4).
Data analysis was performed by a researcher previously uninvolved with the study (J.R.M.) and by a study researcher (M.J.E.), using Atlas.ti. 26 Coding was conducted jointly, and differences in coding decisions were discussed to achieve consensus. For first cycle analysis, open coding techniques were used in conjunction with a preliminary coding protocol 27 : (1) visit type; (2) patient versus physician feedback; (3) positive, negative, mixed, or neutral responses; and (4) concepts associated with each sentiment (such as “connection trouble” or “convenience”). Concept mapping techniques were used to derive a hierarchical thematic structure and define associations between developing concepts. 28 For second cycle analysis, pattern coding was used to further develop categories and themes. 27,29
Sentiment analysis
Sentiment analysis of free-text comments that accompany Likert-scaled item responses can provide more nuance to survey results. We performed automatic sentiment analysis on patients' and the physicians' comments. For each comment, scores representing the magnitude and polarity of the comment's opinion were calculated: the more negative the score, the more unfavorable the opinion conveyed; likewise, the more positive the score, the more favorable the opinion.
Several word-level sentiment dictionaries were combined, and sentiment scores made uniformly binary: −1 for words conveying negative sentiment and +1 for positive words. For each free-text survey response, the sentiment scores of the words were summed to give a sense of the overall sentiment of the response—negative, neutral (a score of 0), or positive. Summary statistics were then compiled (median and interquartile range, mean ± standard deviation) for each survey, overall and by visit, and to identify the highest frequency words used in each survey.
Validity
Measures to enhance validity included use of diverse coders, peer debriefing, and triangulation of analytic techniques, combining both qualitative and quantitative analysis of free-text data. 30 The coding schema is shown in Figure 2, and participant quotes are presented with numeric (study identification number) and categorical identifiers (P = Patient; D = Doctor).
Results
Study Population
The recruiting diagram is shown in Figure 1. Table 1 summarizes baseline characteristics of the study population. Participants were largely white (96%), college educated (73%), older (mean age 66 years), and had Parkinson's disease for 8 years. Familiarity with the Internet was high (96% used the Internet or e-mail at home), and half had previously conducted a video call (54%). Baseline satisfaction with usual care was high (83% satisfied or very satisfied). 5
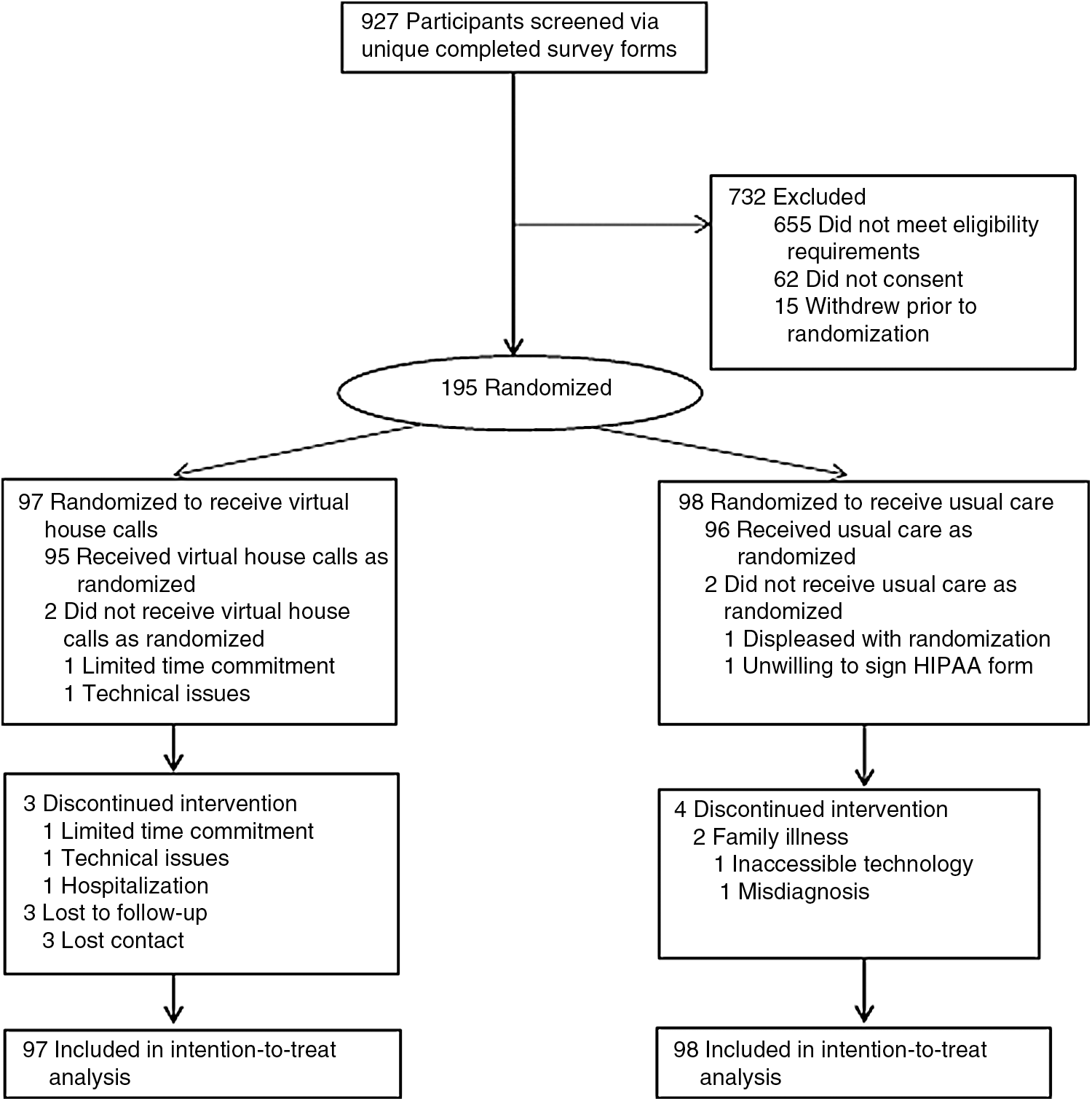
Flowchart of study participants.
Baseline Characteristics of the Study Population
All values are mean (SD) unless otherwise noted.
The number of responses is 195 unless otherwise noted.
Lower scores indicate greater disability.
SD, standard deviation.
Qualitative Content Analysis
Patients' perceptions of virtual house calls
Patients' perceptions of the virtual visits were based on three major themes: (1) personal benefits of the virtual visit, (2) perceived quality of care, and (3) perceived quality of interpersonal engagement. The coding schema used to develop themes is shown in Figure 2, and substantiating quotes are presented in Tables 2 and 3.
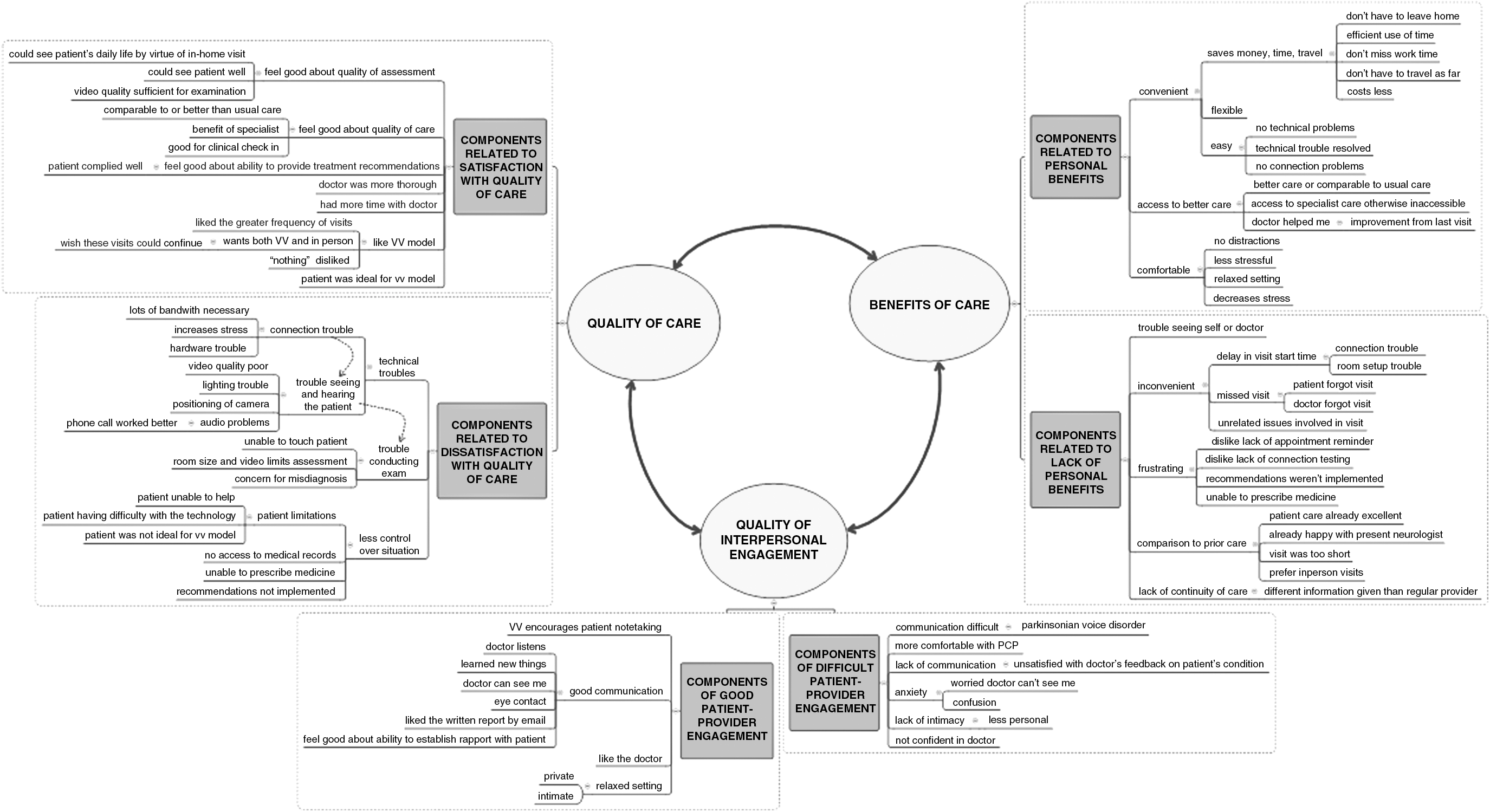
Themes underlying patients' and physicians' perceptions of virtual house calls, with substantiating coding schema.
Themes Underlying Patients' and Physicians' Positive Perceptions of Virtual House Calls, with Substantiating Quotes
D, doctor; P, patient; PD, Parkinson's disease.
Themes Underlying Patient and Physician Negative Perceptions of Virtual House Calls, with Substantiating Quotes
Of 149 cases, 124 (83.2%) expressed positive perceptions of the virtual visits based on substantial personal benefit, high-quality care, and high-quality patient–physician interactions. Nineteen expressed neutral perceptions (12.6%) and reported fewer personal benefits or reported lower quality of care or interpersonal engagement. Only six (4%) expressed negative perceptions.
Personal benefits of the virtual house calls
Personal benefits cited included increased convenience, decreased stress and effort of travel, decreased costs, increased personal comfort, and convenient access to a specialist. The following quote illustrates these benefits:
Patients who reported fewer personal benefits indicated they lived closer to their physician or were already satisfactorily engaged with a Parkinson's disease specialist. For example:
Perceived quality of care
Quality of care was mentioned in 68 cases (45.6%). Most of these (65/68) indicated that they were pleased with the quality of care and felt it to be comparable to or better than traditional care. Few (3/68) felt that quality of care was lower. Concepts cited included more thorough assessments, more time with the doctor, and increased frequency of visits.
Few (4/149) expressed concerns that inability to perform a hands-on assessment decreased the quality of care or limited the exam.
Quality of interpersonal engagement
Quality of the interpersonal engagement was mentioned in 88 cases (59.1%). Patients who described positive interactions with the physician (71/88) also perceived virtual visits positively. Some reported trouble engaging with the physician (17/88), but still felt positive about the virtual visits (9/17), while others expressed neutral to negative perceptions of the visits (8/17). Patient-identified components of quality interpersonal engagement included good communication, feeling seen and understood, feeling that the doctor listened, and liking the doctor. Comments from patients included the following:
Few patients (6/149) expressed negative perceptions of the visits. Those who did also reported technical problems, feelings that the virtual visit was less personal, or confusion as to whom they should follow up with:
In summary, most patients liked the virtual visits and expressed wishes that the virtual visits could be used as part of routine Parkinson's care. When asked if there was anything they disliked about the virtual visit, many responded “NOTHING.” One patient expressed it this way:
Physicians' perceptions of virtual house calls
In contrast to patients, who heavily emphasized the personal benefits of care, physicians' free-text responses were predominantly focused on technical problems (present in 187/399 visits; 46.9%). This included connection trouble (noted in 51/339 visits; 12.8%), audio (31/399 visits; 7.8%) and visual (129/399 visits; 32.3%) difficulties, which limited the physician's ability to see, hear, and communicate with the patient, and which thus interfered with ability to conduct the examination. These difficulties were generally greatest in initial visits and diminished over successive visits. Typical comments from physicians included ones such as the following:
Inability to touch the patient, although less commonly cited as a problem by physicians (16/399 visits; 4%), occasionally contributed to difficulty conducting the examination.
Despite technological difficulties, physicians made many comments like these:
Sentiment Analysis
The overall mean sentiment score for each survey (i.e., combined for all visits) is shown in Table 4, and permits the following observations:
Summary of Survey Sentiment
1. The mean score for general patient feedback (“Participant virtual house call”) suggests a relatively favorable opinion.
2. The overall mean score for patients' dislike of virtual house calls is close to zero, which reflects neutrality in their comments rather than outright expression of dislike.
3. The mean score for general physician feedback (“Doctor virtual house call”) is lower compared with patients, perhaps reflecting a more tempered consideration of telemedicine.
4. Physicians' comments on performing remote motor assessment are scored near zero, suggesting balanced or neutral opinion.
Highest frequency words found in items that direct commenters toward a particular valence can give insight into patients' common opinions. Tables 5 and 6 shows the most frequently found words in comments from “Like about virtual house call” and “Dislike about virtual house call.” The patients liked, for example, the convenience of virtual house calls, with concomitant reductions in their time and their drive to the doctor's office. Although patients disliked technical problems (e.g., computer and connection), their most common dislike was “nothing.”
Highest Frequency Words from Patient Surveys, “Like About Virtual House Call” and “Dislike About Virtual House Call”
Highest Frequency Words from Physician Survey, “Feedback About the Experience of Performing the Motor Assessment Remotely”
Discussion
In this study, patients' and physicians' perceptions of virtual visits were positive and driven by perceived benefits of telemedicine, quality of care, and quality of interpersonal interactions. As frequently reiterated by patients in our study, reduced burden of healthcare access (convenience, comfort, and not having to leave home/travel) is one of the major benefits of virtual over office-based care. These benefits maybe greatest for patients with multiple comorbidities and longer duration of chronic illness. 31 While there are patently disadvantages to virtual care (e.g., technological hurdles and touchless examinations), the potential benefits to chronically ill patients warrant ongoing efforts to improve the utility and feasibility of this care modality.
It is important to note that pursuit of convenient care does not imply quality should be compromised. Responses from this and other studies suggest that quality of care remains important to both patients and providers, and affects how telemedicine is perceived. 32 However, definitions of “quality care” may differ substantially between groups. 33 Physicians in this study, as in others, indicated that the ability to conduct the physical exam was limited by audio/visual problems, which translated into a sense of diminished quality of care. 34,35 Conversely, patients rarely commented on limitations of the examination, instead prioritizing communication and relational closeness. With increasing emphasis on providing patient-centered care, finding a middle ground that meets the needs of both parties will be essential to preparing telemedicine for mainstream use. Encouragingly, the majority of concerns expressed by providers were related to technical issues, which will likely be resolved with time and increased technological familiarity. 36,37
As with office-based care, patients' perceptions of quality of care in telemedicine appears to be strongly connected to the quality of the patient–provider interpersonal engagement. 31,32,38,39 Whether virtual or otherwise, the patient–provider relationship will likely retain a central role in how care is perceived. Our data further suggest that interpersonal engagement during telemedicine may in some ways be considered superior by patients, who value a comfortable environment with fewer external distractions and greater opportunity to ask questions. Similar findings have been noted elsewhere. 40
Overall, sentiment in patient responses was strongly positive, while provider sentiment was only moderately positive, most likely due to persistent technical issues. The strong positive valence of patients' perceptions is well supported by prior research, 18 as well as concurrent survey data showing 96% were satisfied with the virtual visits. 5 In contrast, providers' surveys revealed a stronger quantitative satisfaction ranking (83% positive) than was evident in the qualitative data. 5 This maybe due to the fact that providers used the free-text responses to discuss technical issues pertaining to the visit. Thus, our qualitative data may not fully reflect providers' overall feelings toward telemedicine, and should be interpreted cautiously. Despite this, the provider data give valuable insight into issues that are central to telemedicine, and highlight the connection between technical quality and overall impact on quality of care in the telemedicine context.
The study had several limitations. First, participation in this study, was not equitable and likely reflected the digital divide. 3,41 Study participants were overwhelmingly white, well educated, and more familiar with the Internet than the general population. 3,41,42 Second, not all participants and physicians responded to every survey, and responses may have been biased toward those who felt most strongly about the visits. Third, we specifically asked what patients did or did not like, which may have elicited more negative or positive responses than patients might have volunteered otherwise. Because data were collected in survey rather than interview format, we were unable to explore or further contextualize responses, and we could not assess if nonresponders' or partial responders' perceptions qualitatively differed from those who responded.
Future efforts may address these limitations. Inclusion of underserved populations and those with less familiarity with the Internet may help determine the generalizability of these results. Use of interviews with patients and providers, as opposed to online surveys, maybe helpful in reducing response bias due to impaired motor function.
Despite the noted limitations, this study provides valuable insight into factors underlying patients' and providers' perceptions of in-home virtual visits. These findings may be applicable to other conditions associated with aging (e.g., Alzheimer's disease), 2,43 reduced mobility (e.g., amyotrophic lateral sclerosis), or limited specialty access (e.g., rare conditions). 44 Although a new technology, the age-old issues of quality care and interpersonal engagement remain central to healthcare. Thus, prioritizing good interpersonal communication, quality of care, and benefits to patients will help ensure that telemedicine achieves its potential to deliver quality patient-centered care to anyone, anywhere.
Footnotes
Acknowledgments
Statistical analysis conducted by Dr. J.R.M., PhD, NP-C, University of Rochester School of Nursing, University of Rochester, Rochester, NY, and by Dr. J.J.J., PhD, Department of Biostatistics and Computational Biology, University of Rochester, Rochester, NY. The Patient-Centered Outcomes Research Institute had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; or preparation, review, or approval of the article. Software used in the study was provided and supported by SBR Health (Cambridge, MA), Vidyo (Hackensack, NJ), and ID solutions (Indianapolis, IN).
Author Contributions
J.R.M.: Analysis or interpretation of data, design or conceptualization of the study, and drafting or revising the article for intellectual content. M.J.E.: Analysis or interpretation of the data and drafting or revising the article for intellectual content. J.J.J.: Analysis or interpretation of data, design or conceptualization of the study, and drafting or revising the article for intellectual content. C.A.B.: Analysis or interpretation of data and drafting or revising the article for intellectual content. D.B.B.: Analysis or interpretation of data and drafting or revising the article for intellectual content. K.M.B.: Analysis or interpretation of data and drafting or revising the article for intellectual content. C.M.B.: Analysis or interpretation of data and drafting or revising the article for intellectual content. P.N.S.: Analysis or interpretation of data and drafting or revising the article for intellectual content. R.S.: Analysis or interpretation of data and drafting or revising the article for intellectual content. A.W.W.: Analysis or interpretation of data and drafting or revising the article for intellectual content. E.R.D.: Analysis or interpretation of data, design or conceptualization of the study, and drafting or revising the article for intellectual content.
Industry Sponsor
This study was sponsored by the Patient-Centered Outcomes Research Institute (AD-12-11-4701).
Disclosure Statement
Dr. E.R.D. serves on the medical advisory board of and has stock options in Grand Rounds. All other authors report no disclosures.