
Abstract
Background:
Mobile health and telemedicine are rapidly evolving fields used to provide healthcare remotely to patients. For surgical patients, telemedicine can improve patient education and remote monitoring of postoperative symptoms. We performed a systematic review of studies involving the use of short message service (SMS) and mobile application-based interventions in surgical patients to evaluate the advantages and disadvantages of each system, as well as of mobile interventions as a whole.
Materials and Methods:
Major electronic databases were searched using relevant keywords from inception until November 2016. Studies involving SMS or mobile application-based communication protocols involving at least 25 preoperative or postoperative patients were included. Studies of systems involving communication exclusively between healthcare professionals were excluded.
Results:
A total of 2,492 unique studies were identified through keyword search. After applying inclusion and exclusion criteria, 15 studies were included in this review. Intervention modalities were SMS (8 studies), mobile application (4), combined SMS and application (1), automated phone call (1), and electronic transmission of pictures to the physician (1). Intervention methods were symptom monitoring (7), patient education (2), protocol adherence reminders (4), and combined symptom monitoring and protocol adherence reminders (2). Both mobile applications and SMS-based interventions increased adherence to medications and protocols and improved clinic attendance. Lower readmission rates and emergency room visits were reported. Satisfaction with automated communication systems was high for both patients and physicians.
Conclusions:
Mobile interventions provide a sophisticated yet simple tool to improve perioperative healthcare. Future considerations to address include usage fatigue and Health Insurance Portability and Accountability Act compliance concerns.
Introduction
Surgical outcomes heavily depend on effective patient education and adherence to perioperative protocols. Traditional tools used to educate patients include face-to-face counseling, printed materials, and more recently, tablet-based electronic interfaces. 1 Similarly, communication between patients and healthcare teams has largely been conducted through telephonic interactions often involving several layers of personnel. Mobile health (m-health) shows tremendous potential for improving communication between patients and providers, as well as increasing patient adherence through reminders and focused education. 2 –8
The application of telemedicine has expanded greatly as cell phone usage has become virtually universal. 9 Mobile devices have been incorporated into the medical realm in a variety of contexts ranging from medication reminder applications to algorithms that monitor patient symptoms postoperatively. 3,10 Numerous studies suggest that short message service (SMS) text messaging or applications that remind the patient to perform health-related activities can markedly increase treatment adherence. 2 –8
The use of telemedicine and m-health in the surgical realm is expanding rapidly. Telemedicine in surgery has been used as an educational tool to inform patients about their procedure and to remind patients to adhere to their prescribed health activities both preoperatively and postoperatively. 6,11 –13 SMS has also been implemented for earlier identification of postoperative complications by remotely evaluating patient symptoms after discharge. 10,14 –17 Various studies also suggest that telemedicine can reduce healthcare costs by lowering clinic no show rates, readmission rates, and preventable emergency room visits. 15 –19
While individual studies have documented improved perioperative patient care using electronic patient communication systems, there is no broad consensus regarding such applications. Hence, we conducted a systematic review to examine patient-centered outcomes in studies using SMS text messages or mobile applications in the perioperative period in an effort to summarize the data and identify future directions in automated patient communication interventions (APCIs).
Methods
Inclusion and exclusion criteria
The inclusion criteria required that the studies use some form of SMS-based or application-based interface to communicate reminders, treatment protocols, or perioperatively monitor a surgical patient's symptoms. All age groups were included. Studies were excluded if they used purely educational applications to increase patient understanding. Studies were also excluded if the applications or interfaces focused on interactions between healthcare providers without any patient involvement. Any non-English were excluded. We required a sample size of 25 patients to ensure clinical relevance and to exclude feasibility-only studies.
Search process
The literature search was performed in November, 2016 in eight databases using key terms by a medical librarian at Washington University in Saint Louis School of Medicine. The databases include Ovid MEDLINE, Embase, Scopus, the Cumulative Index of Nursing and Allied Health Literature, Cochrane Database of Systematic Reviews along with Cochrane Register of Controlled Trials, ProQuest Dissertations and Theses, and
After removing duplicates, the search resulted in 2,492 unique studies. This initial list of searches was split four ways between four researchers, and studies were selected by applying the inclusion and exclusion criteria to the abstracts. Seventy four (n = 74) studies remained after this preliminary screening. This shorter list of studies was further analyzed using the same inclusion and exclusion criteria by one researcher to identify the 15 studies that are examined in this review. Data were then gathered from these 15 studies by one researcher to standardize the collection process. The PRISMA flowchart details this selection process (Fig. 1).
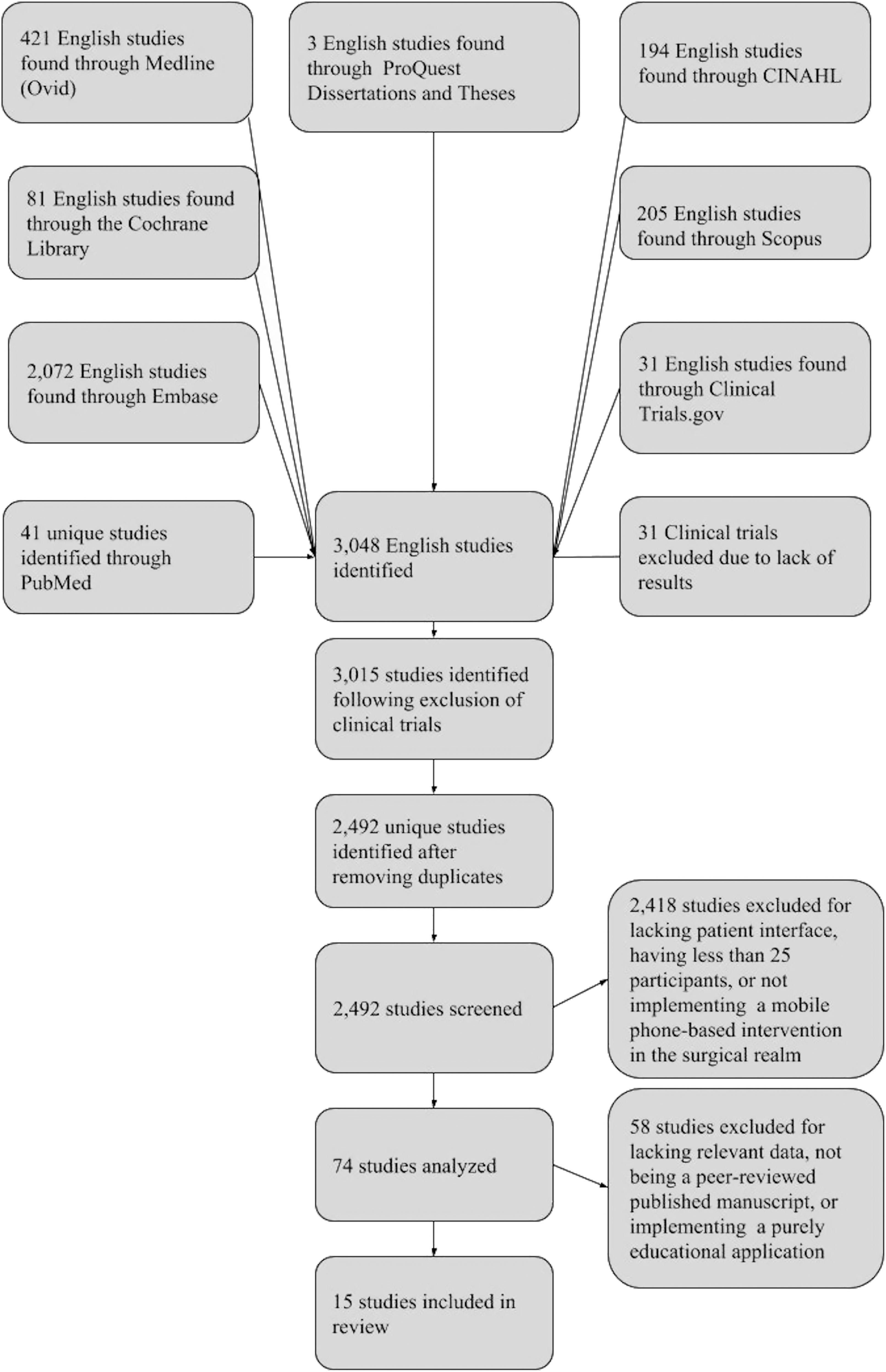
PRISMA flowchart outlining the study selection process.
For each of the studies, we recorded the type of intervention used (SMS or smartphone application), surgical procedure performed, purpose of the messages sent, number of patients enrolled, study design, results, and patient satisfaction with the system, if measured.
Results
After the initial search, a total of 3,048 initial studies were identified. Of these, 525 were duplicates, leaving 2,492 unique studies. A total of 2,451 results were obtained from the keyword literature search and 41 from an independent search in PubMed and MEDLINE. A total of 2,418 articles were eliminated from our review for not meeting the inclusion and exclusion criteria. After further review, another 59 studies were excluded for lacking relevant data, not being a peer-reviewed published article or implementing a purely educational application. All but 15 articles were eliminated. 8,13,16 –18,20 –29
Of the 15 studies that met our criteria, 8 studies utilized SMS, 4 used smartphone applications, 1 used both SMS and a smartphone application, 1 implemented automated phone calls, and 1 study provided phones for pictures to be sent to the physician (Table 1). Of the included studies, 6 were randomized controlled trials (RCTs), 7 were prospective observational, 1 was a retrospective cohort, and 1 was a cross-sectional correlational design study. Six of the 15 studies monitored symptoms, 3 provided patient education (of which 2 promoted postoperative adherence and 1 also provided supportive messages), 3 focused on encouraging patient adherence to medications or protocols, and 3 included a combination of monitoring symptoms while encouraging patient adherence to medications or protocols. The sample sizes ranged from 26 to 1,200. The duration of the interventions spanned from 5 days to 13 months. The studies were performed in 8 countries. None of the studies quantified costs and savings data, but three studies implied fewer clinic or emergency room visits and decreased utilization of resources. 17,20,29
Overview of the Message Type, Message Purpose, Study Size, and Study Design Implemented
SMS, short message service; RCT, randomized controlled trial.
The studies evaluated involved a variety of procedures (Table 1). Only one study offered a preoperative intervention. 13
Symptom monitoring
SMS and applications were implemented to monitor symptoms postoperatively. In the studies involving postoperative monitoring, temperature and pain were the most frequently monitored symptoms. 10,20,21,23,24,29 Other symptoms monitored included nausea, vomiting, constipation, dizziness, shortness of breath, weight, blood pressure, blood glucose, and drain output.
Four of the postoperative symptom monitoring systems generated alerts to clinicians based on patient responses, allowing for prompt responses by medical teams to abnormal symptoms. 10,20,23,29 Semple et al. 29 monitored postoperative symptoms in breast reconstruction and orthopedic patients by allowing patients to send daily pictures of their wound through an application to the medical team. Surgeons were able to cancel 6-week follow-up visits for orthopedic patients and first or second week follow-up visits in breast reconstruction patients if the pictures suggested normal wound healing. 29 Debono et al. 23 developed an application that could generate a nonresponse, green, orange, or red alarm based on the severity of symptoms reported by patients (i.e., pain, temperature, and so on). During the study, 31.7% of patients triggered an orange or red alarm that required response. In 18 of 19 patients who generated an orange or red alarm, concerns were settled by phone without further consultation. 23 Similarly, a study by Cleeland et al. 10 sent alerts to clinicians based on adverse events (i.e., pain, shortness of breath, and so on) using predetermined criteria. The intervention group reported more efficient symptom triage, which led to fewer threshold events (automatic alerts generated for concerning symptoms), a more rapid decline in adverse event rate, and better postoperative function. 10 Similarly, Carrier et al. 20 concluded that their SMS intervention resulted in earlier detection of postoperative colorectal complications.
In a study by Martinez-Ramos et al. 17 30 of 96 patients generated a surgical wound alert. Complications were resolved in 29/30 of the cases without readmission. About 55% of the patients who reported complications stated that they would have returned to the hospital if not for the intervention. 17
Clinic attendance
Lin et al. 18 studied the influence of SMS reminders on clinic attendance in an RCT. They noted higher attendance at an ophthalmology clinic in the SMS intervention group, resulting in a significantly greater number of vision-saving surgeries being performed. Clinic attendance rates in the intervention group continued to increase throughout the study, suggesting that SMS was effective at improving long-term attendance. 18
Efforts to limit unnecessary clinic visits have also been studied. When patients texted their daily drain outputs to providers, Rao et al. 16 reported a fewer number of return clinic visits within the first 30 days (p = 0.0004) and 90 days (p = 0.017) postoperatively and reported fewer unplanned clinic telephone calls in the messaging group (p = 0.0002). Patients in the messaging group were also more likely to undergo drain removal at the first clinic visit. 16
Age of Patients
Four of 15 studies focused on pediatric populations; 2 of these studies had parents or caregivers respond to messages, while 2 studies required pediatric patients to respond themselves. 8,18,21,28 The other 11 studies focused on adult populations; the average age ranged from 25.330 to 62. 24 None of the included studies focused solely on a geriatric population; however, many included geriatric patients.
SMS versus application-based interventions
Both SMS- and application-based interventions led to greater adherence in all studies where the primary outcome was adherence to medications or protocols (Table 2). The studies utilizing SMS interventions reported increased adherence to prescribed protocols, 22,25,28 earlier detection of postoperative complications, 20 increased attendance to clinic, 18 decreased episodes of rejection in organ transplant patients, 8 and decreased time to drain removal compared to control groups in the respective studies. 16 The studies utilizing applications reported increased adherence 31 and increased self-monitoring. 26 Miloh et al. 8 suggested that some of the advantages of SMS are its relative simplicity, low cost, minimal time commitment for health professionals, high levels of acceptance, and ability to be used for a large number of patients. DeVito et al. 24 suggested that applications like Pocket PATH were advantageous because they could monitor health indicators, display trends over time, calculate out-of-range values, and guide their decision-making about what and when to report to clinicians.
Message Type Sent to the Patient and Conclusion for Each Study Evaluated
BMI, body mass index; CI, confidence interval; OR, odds ratio.
Satisfaction
For the broad range of APCIs, both patients and surgeons reported high satisfaction rates (Table 3).
Patient Satisfaction Scores with the Intervention
Discussion
In this systematic review, we evaluated the results of automated SMS and application-based interventions used in the surgical setting. The APCIs evaluated overwhelmingly impacted patient adherence, outcomes, communication, patient satisfaction, and physician workflow positively.
SMS-based interventions were implemented twice as frequently as application-based interventions in the studies evaluated (8 vs. 4, respectively). We hypothesize that smartphone applications are used less frequently because they have higher barriers of entry for the patient than SMS interventions. A smartphone is required to download an application, while any cell phone can send and receive SMS. An SMS-based intervention is preferred over an application-based intervention due to this cost barrier.
In contrast, applications have the potential for a superior graphical interface with more modalities of communication, such as videos and pictures. 13,29 For example, the Pocket PATH application allows lung transplant patients to track their own progress through charts, facilitating instantaneous feedback. 31
m-Health interventions showed promising results in increasing patient adherence. 8,22,25,28,31 Patient noncomprehension of discharge instructions has been a documented problem. 32 The hospital is a stressful environment and discharge instructions from clinicians may not be clear to the patient. 33 Patients may have difficulty understanding and remembering details of discharge instructions. 34,35 Based on the increased patient adherence suggested by numerous m-health intervention studies, we hypothesize that automated information delivery may be more effective because it is not as overwhelming for the patient. Automated information delivery allows for reminders and feedback from the medical team to patients in the comfort of their home instead of the hospital. These reminders also address unreliable patient recall of discharge instructions. The observer effect, where people behave differently when they are aware of being monitored, may also be involved. This m-health mediated increase in adherence may translate into improved clinical outcomes.
Lin et al. 18 suggested that SMS-based interventions may have a significant impact on clinic attendance in developing countries, specifically China. Lin et al. 18 showed a 47.2% increase in ophthalmic clinic attendance post-SMS intervention. While providing medical care to underserved populations in developing countries in a formal clinic may be difficult, cell phone possession is virtually universal. 36 Given the suggested benefits of m-health interventions and high cell phone possession rates, m-health interventions may be an effective tool to monitor and remind patients to perform their health-related activities when they cannot be examined in a formal clinic.
Symptom monitoring by m-health interventions postoperatively reduced the need for patient visits 29 and produced effective alerts for rapid triage and care. 8,10,20,23 One consideration when determining the threshold for alerts involves whether an alert should be generated for a patient nonresponse to a message. Carrier et al., 20 Miloh et al., 8 and Debono et al. 23 generated alerts for nonresponse. They hypothesized that a nonresponse could have resulted from a negative patient outcome and may necessitate follow-up from the provider. However, the frequency of alerts and how the medical team receives alerts (SMS, e-mail, phone call, etc.) should also be considered. Debono et al. 23 reported that 19 patients generated 29 alarms. Such a high frequency of alerts requires response from the medical team and is an increased burden.
The advent of fast track recovery programs, such as Enhanced Recovery After Surgery, and a possible movement toward outpatient surgery for specific procedures in fast track units make remote monitoring of systems increasingly important. Length of effective patient monitoring will depend on the procedure and the time window and severity of possible complications, as suggested by the APCIs evaluated. Patient monitoring ranged from 5 days (Carrier et al. 20 ) to over a year (Miloh et al. 8 ).
While the relative underuse of mobile phones within geriatric populations may present a barrier to implementation of m-health interventions within this demographic, the studies evaluated in this review suggest that both young and old patients (ages ranging from 2 to 84) can benefit from m-health interventions. 8,17
Although not directly evaluated, potential cost savings were suggested in some of the studies reviewed. Carrier et al. 20 implied that their intervention resulted in fewer emergency room visits. In Martinez-Ramos et al.'s 17 study, 55% of patients who reported complications stated that they would have returned to the hospital if not for the intervention. Chen et al. 21 suggested that costs and resources could be saved if low-risk patient groups, whose symptoms could be monitored through applications, made fewer clinic visits. Conversely, monitoring of high-risk patient groups and earlier detection of complications may also lead to a reduction in costs. Mobile interventions that reduce the requirement for in-person follow-up may provide a financially advantageous alternative to traditional office visits.
One concern for all m-health interventions is Health Insurance Portability and Accountability Act (HIPAA) compliance and protection of patient health information (PHI). 37,38 Current standards specify that all m-health interactions should be secured to the “greatest practical extent through use of a private, point-to-point circuit, Integrated Services Digital Network, Advanced Encryption Standard 5 encryption, or virtual private network for Internet transmissions.” 37 Even if the server containing the patient data is secure and the connection is difficult to intercept, record of all interactions will be on that patient's phone. Anyone with access to the patient's phone can observe all transmitted conversations. HIPAA compliant messaging applications exist, but they require use of a smartphone and thus are inaccessible to some patients. 39,40 Regular SMS cannot be encrypted. 41 While finding an ideal solution to this issue is difficult, protecting PHI on secure servers, securing the connection, and transmitting the minimal amount of PHI as possible limits patient exposure.
SMS or application usage fatigue, where users may stop responding to the interface, is a limitation for all such interventions. Semple et al. 29 reported that logins were higher in the first 14 days versus days 15 through 30. Miloh et al. 8 reported 41% dropout rate by 4 months. Miloh et al., 8 Mundi et al., 13 and Semple et al. 29 also suggested decreased response rates later into the study. Interventions should be designed in a way to maximize patient retention. An excessive number of notifications, messages, or required responses may decrease engagement. Strategies used in commercial mobile applications may be effective. They include personalization of message content and sending of notifications at times when a user is most likely to view them.
Our review has several limitations. The number of studies included, 15, was relatively small. Only a few articles for each of the categories of monitoring, adherence, and reminders were available to analyze. The studies were heterogeneous, with varying study design, patient demographics, messaging modalities, procedures performed, and outcome measures. This precluded meaningful statistical analysis. Publication bias was also of concern. We attempted to minimize publication bias by searching multiple databases with a wide range of search terms.
Conclusions
This review found that SMS-based and application-based interventions can efficiently and accurately evaluate surgical patient symptoms postoperatively, improve patient adherence to prescribed protocols, improve clinic attendance, and have the potential to reduce healthcare costs. Mobile interventions have high patient satisfaction rates and can be used for wide age ranges. Future issues of concern include the difficulty of maintaining patient engagement and protection of PHI.
Currently, m-health interventions are not widely used, and data reporting their effectiveness are limited. However, m-health interventions have the potential to achieve an amount of precision and personalization in healthcare that present manpower limits cannot support. By utilizing a patient's own technological resources, m-health not only provides useful information to the medical team but also engages the patient in their own healthcare and facilitates joint decision-making between patient and provider. A practical application of these benefits is in addressing patient dissatisfaction with appointment availability. With the information obtained through m-health data, providers can better customize an appointment to target a patient's needs and even avoid unnecessary appointments.
Footnotes
Acknowledgments
The authors thank the library at Washington University in St. Louis School of Medicine for their assistance in the literature search and members of the Epharmix Research Center for their support. The authors also thank Craig Yugawa for his help in the acquisition of data.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure Statement
No competing financial interests exist.