
Abstract
Objectives:
The aim of this systematic review was to evaluate the validity of using teledentistry in oral care examination and diagnosis.
Methods:
In June 2016, a systematic search of the literature was conducted without time restrictions in three electronic databases (Ebscohost, Pubmed, and Scopus). Two reviewers screened the retrieved articles first by title and then by abstract to determine relevant articles for full text review. Studies included were as follows: (1) related to teledentistry, (2) available in full text and English, (3) compared teledentistry application to a gold standard, and (4) provided clear statistical tests for validity. The methodological quality of studies was determined using the “Quality Assessment of Studies of Diagnostic Accuracy (QUADAS).”
Results:
Seventy-nine studies met the initial search criteria. Following removal of duplicate articles, only 58 were remaining and reviewed by title and abstract, yielding 14 full-text articles. Nine of the full-text articles met the inclusion criteria. Results of the QUADAS assessment varied from 9 to 13 out of 14 items; therefore, studies demonstrated high quality (>60%). Validity of teledentistry varied and is reported by range for the following statistics: sensitivity (n = 8, 25–100%), specificity (n = 7, 68–100%), positive predictive value (n = 5, 57–100%), and negative predictive value (n = 5, 50–100%). Kappa statistics were also reported for evaluation of reliability between gold standard and teledentistry examination (n = 6, 46–93%).
Conclusions:
Teledentistry could be comparable to face-to-face for oral screening, especially in school-based programs, rural areas and areas with limited access to care, and long-term care facilities. Identification of oral diseases, referrals, and teleconsultations are possible and valid. The need for methodologically designed studies with appropriate statistical tests to determine the validity of teledentistry exists.
Introduction
Teledentistry emerged as a part of telemedicine following years of global telemedicine practice. In 1989, at a conference in Baltimore, Maryland, focused on the delivery of dental care using dental informatics, the term, “teledentistry,” was introduced. 1 Teledentistry is defined as using telecommunication technology, electronic medical records, video, and digital images to facilitate dental services delivery for distant or isolated people or for consultations among specialists. 2 Teledentistry does not only encompass technology or a varied set of related forms of technologies but is also a collection of clinical processes and organizational arrangements combined with technologies. Incorporating teledentistry in dental health services has the potential when used appropriately to improve access, early intervention, and health education to enhance the quality, efficiency, and effectiveness of dental health services. 1
There are barriers that could slow adoption of telemedicine technology such as reimbursement issues, license regulations, costs, limitations in physical examinations, and equipment required. 2,3 Reimbursement is one of the main challenges that slows development and adoption of teledentistry. Medicaid reimbursement is available in some cases providing limited compensation, limiting adoption of this technology by dental professionals in their dental practices. 4 The use of telemedicine technology to deliver healthcare services has contributed to a reduction in the cost of healthcare treatment for patients and equipment for providers. 5 Yet, teledentistry has not been as widely accepted as telemedicine, even though use of teledentistry increases access to dental services for those who live in rural areas. 6
Systematic reviews of teledentistry, adoption, and use are few. The first systematic review published in 2013 comprehensively reviewed all published studies in teledentistry. 7 A second systematic review focused on the application of teledentistry in three areas: (1) clinical outcomes, (2) utilization, and (3) costs. 8 The third reviewed the accuracy of dental images for the diagnosis of dental caries. 9 It is crucial to assess the validity of teledentistry in the delivery of oral care before making a decision to adopt the technology and implement use in dental practice. No previous systematic reviews that evaluate the validity of teledentistry have been published to the best of our knowledge. Evidence that teledentistry is valid in the delivery of oral care may change policy makers' and dental professionals' decisions leading to adoption of the technology. The purpose of this systematic review was to evaluate the validity of teledentistry for examination and diagnosis.
Methodology
Information Sources and Search Strategy
The primary investigator performed a systematic search of the literature for studies assessing validity of teledentistry without time limitation during June 2016. Search filters were to limit retrieval to peer-reviewed journal articles published in English. Books, editorials, reviews, commentary reports, dissertations, unpublished materials, and letters to the editor were not included in the search. Three databases to retrieve articles related to the purpose of this study were as follows: PubMed/Medline, Scopus, and EBSCO host (EBSCO host included several databases such as CINAHL, Dentistry and Oral Sciences, ERIC, Academic Search Complete, etc.). Search terms with different alterations included the following: “teledentistry and validity,” “teledentistry and reliability,” and “telemedicine or telecare or telehealth or teleconsultation and validity and dentistry or dental.” Table 1 shows search terms entered into each electronic database. The Boolean operator “AND” and “OR” were used to combine the search key terms.
Search Terms and Databases
Study Selection and Data Extraction
The first step was to evaluate each article identified from the database against the inclusion criteria. Second, two reviewers independently screened each article. Three articles required discussion between the reviewers to determine inclusion. Fifty-eight articles were reviewed by title and abstract. Forty-four articles were removed after reviewing title and abstract. Full-text articles were retrieved on the remaining 14 publications. Abstracts found to be relevant were obtained for review. Full text of 13 articles that met the inclusion criteria was retrieved and reviewed for eligibility. All the articles were analyzed, discussed, and reviewed by two investigators. Figure 1 shows the flow chart of article selection.
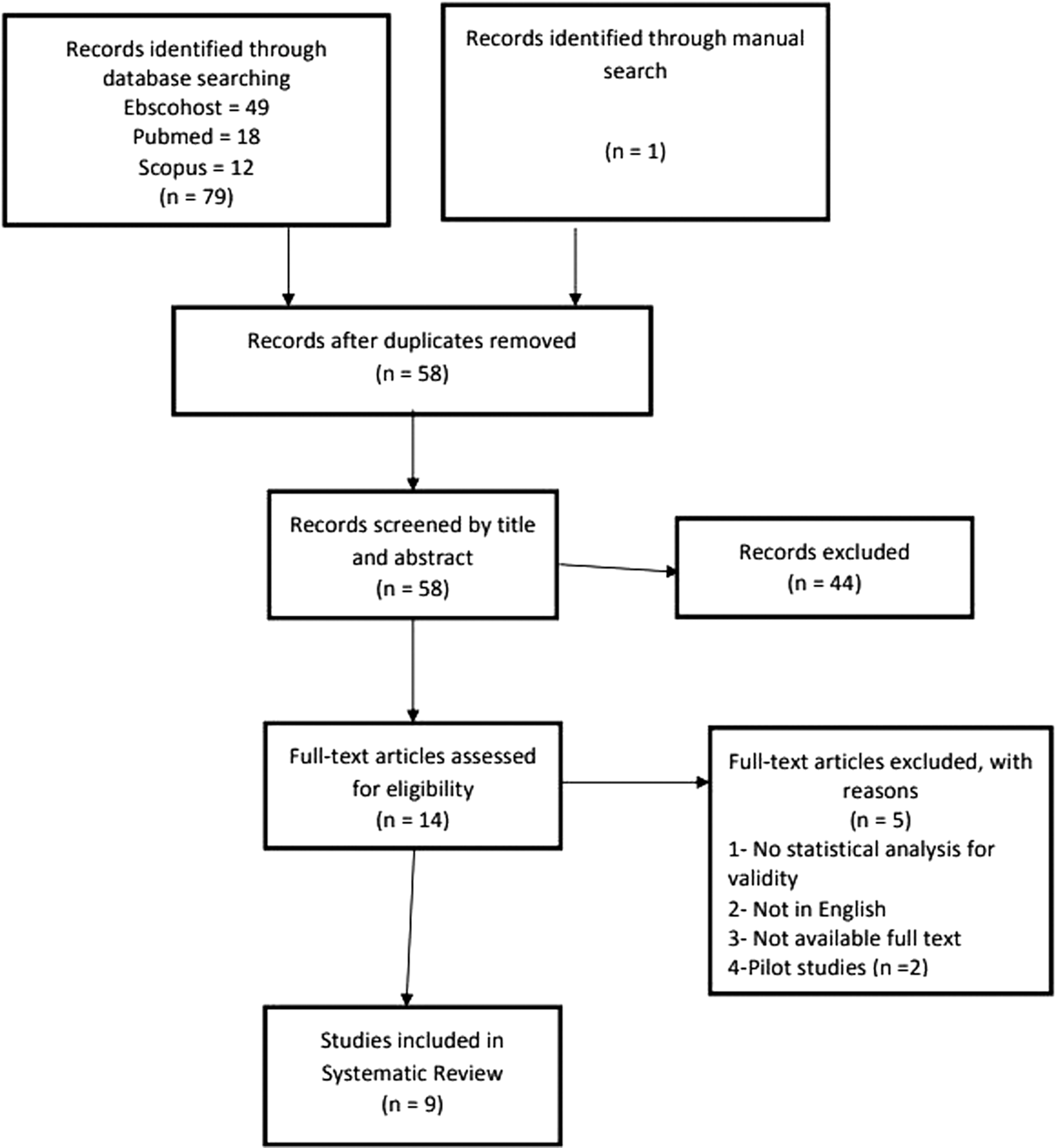
PRISMA flowchart of articles reviewed.
Inclusion and Exclusion Criteria
Articles were included if they met the following criteria: (1) related to telehealth or teledentistry, (2) written in English and full text available, (3) compared teledentistry to visual examination or gold standard examination, (4) used any form of telecommunication or telehealth for the examination, and (5) had clear statistical tests to evaluate validity. The following articles were excluded: (1) not related to teledentistry or telehealth, (2) pilot studies due to small sample size or the main study was included in the systematic review, (3) studies with insufficient or missing information to be included in the study, (4) full text was unavailable, (5) insufficient data analysis, (6) no description of “gold” standard, and (7) only a published abstract was available. Since this systematic review focused on the validity of teledentistry when compared to a “gold standard” or clinical assessment, there was no restriction with respect to the study design, population characteristics, and sample selection.
Quality Assessment
Two reviewers independently assessed the quality of methods for the included studies. The “Quality Assessment of Studies of Diagnostic Accuracy” (QUADAS) tool was used to assess the methodological quality of the validity for studies included in this systematic review. 10 The QUADAS tool has 14 components with a rating of “yes,” “no,” or “unclear” for each component. Reviewers discussed each component of the QUADAS to resolve any differences. According to the QUADAS guidelines, a study is considered high quality if the QUADAS score was more than 60%. 11 No studies were excluded based on the quality assessment.
Statistical Considerations
The focus of systematic review is to assess the literature on the validity of teledentistry. Statistical tests are crucial to determine the validity of research findings in any quantitative study and therefore, the need for appropriate statistical tests to measure validity in the reviewed articles. Agreement between teledentistry examination and visual examination as the gold standard is also important to assess validity. Statistical tests to measure validity such as Kappa, specificity, and sensitivity needed to be present to show the percentage of true or false agreement.
Results
Figure 1 shows a total number of 79 studies identified from database searches; 49 studies from EBSCO Host, 18 from PubMed, and 12 from Scopus. Once duplicate articles were removed, 58 potentially relevant articles were screened based on their titles and abstracts. Fourteen of these relevant articles met the criteria for full text review. After reviewing the 14, only 9 articles met the inclusion criteria and were included in the review.
Characteristics of the Included Studies
Most of the nine publication dates were 2002–2016. Research occurred in several countries: three from the United States, two in the United Kingdom, and one in each of the following countries: Brazil, Portugal, Australia, and Germany (Table 2). Four studies were in pediatric dentistry, two in general dentistry, and one in maxillofacial radiology, endodontics, and orthodontics, and publications were in different journals and one book. Most journals were not related to telehealth or teledentistry (Table 2).
Characteristics of the Included Studies
DFS, decayed and filled surfaces; DMFT, decayed, missing and filled teeth; GS, gold standard; MLDPs, mid-level dental practitioners; OMFS, oral and maxillofacial surgeons.
Only two studies used random sampling to recruit participants. 12,13 The remaining studies used convenience sampling; however, not all the studies involved human participants; one article used facial radiographs, and another study used extracted teeth as the basis for comparison. In those with human participants, the number of participants ranged from 29 to 327 (Table 2).
Four studies were conducted on children and young adults from 1 year to 19 years of age. 12,14 –16 The study that used facial radiography did not include the age of participants. 17 Two studies recruited subjects of different ages as the age of the individual was not the variable of interest. The variable of interest was accuracy of diagnosis. 13,18 An additional study used extracted comprised teeth from adults aged between 40 and 70 years. 19 The majority of studies were of cross-sectional design, performed in a specific time; and, there were only two randomized controlled studies. 12,13 Eight studies were conducted in a clinical setting and only one in a laboratory. 19 (Table 2).
Quality Assessment of Validity Studies
The QUADAS 10 was used to assess each article (Table 3). The results of the assessment varied from 9 to 13 out of 14 items; therefore, those reviewed demonstrated good quality (>60%). Table 4 shows the results of the quality assessment appraisal. Most of the studies addressed the validity of teledentistry technology in dental diagnosis and did not include random sampling, instead convenience sampling was used, which is unlikely to be representative of the population.
Quality Assessment of Studies of Diagnostic Accuracy
The Result of the Quality Assessment Appraisal by Two Reviewers
UN, unclear.
The Intervention
There was some variation among studies in the type of equipment used for teledentistry. Four out of nine studies used an intraoral camera to gather images of teeth for later examination. 12,16,19,20 Three studies used a digital extraoral camera 13 –15 and one study used a smartphone camera. 18 All the included studies utilized store-and-forward (asynchronous) mode and no study used real-time (synchronous) communication or videoconferencing.
The gold standard reported most often was the traditional visual examination. Methods and items used for visual examination varied among the studies. Methods and items used for examinations included the following: use of light soucrce, 14,12 sterilized exploration kit, 15 probe, 14 air syrange, 14 mirror, 12,14,16,20 explorer, 12,20 and palpation. 20 Visual clinical examination for dental caries assessment was used in four studies. 12,14,16,18
The validity of teledentistry compared to visual examination in the decision accuracy of referrals was reported. 13 –15 Diagnosis from a radiograph gold standard (GS) was compared to the diagnosis of the same radiograph accessed remotely through the telemedicine system. 17 Treatment decisions based on a dentist or allied dental professional's visual assessment as GS to virtual examination have been reported. 20 An endodontic study captured, intraoral images of the entire pulp canal floor of extracted third molars for later visual examination. Remote assessment of canal orifices compared to the histological images of the dental pulp (GS) determined validity. 19
Personnel varied in the studies. General dentists who performed both the gold standard and teledentistry examination possessed a range of experience. 12,16,20 Oral and maxillofacial surgeons, and accident and emergency personnel assessed maxillofacial fractures from radiographs. 17 Two dental therapists performed the teledentistry examination in another study 18 ; and an oral surgeon and an orthodontist conducted the gold standard examination in two studies. 13,15 Other studies reported only that the examination was performed by a dental examiner, researcher, or observer with no specifics as to experience or type of examiner. 14,16,19
Statistical Analysis
Table 5 shows sensitivity and specificity reported by the majority of studies. Eight out of nine studies reported calculated sensitivity with values ranging from 25% to 100%, and seven with specificity values from 68% to 100%. Moreover, positive predictive value (PPV) of teledentistry examinations ranging from 57% to 100% and negative predictive value (NPV) ranging from 50% to 100% were reported (Table 5). Five studies used the Kappa statistic to evaluate agreement between teledentistry and visual examinations.
Summary of the Statistical Results of the Included Study
NPV, negative predictive value; PPV, positive predictive value.
Agreement between gold standard and teledentistry examinations ranged from 46% to 93% (Table 5). One study found that the mean difference of decayed filled surface scores between the teledentistry and control groups was not significantly different (p > 0.001). 12 In the area of maxillofacial radiology, 17 the diagnosis of facial fracture by plain radiograph was more accurate than images sent by a telemedicine system. Images with low quality were poorly diagnosed by a telemedicine system (sensitivity 25–100% and specificity 68–100%) 17 (Table 2).
Discussion
The aim of this systematic review was to explore the body of literature to determine the diagnostic validity of teledentistry for use in dental practice. System validity reflects the degree of accuracy of measuring what is to measure. 21 Investigating teledentistry validity is an important step in determining whether teledentistry is as accurate as traditional oral examinations. The validity of a teledentistry system is crucial because clinical decision-making through telecommunication may not be accurate as face-to-face traditional examinations. Moreover, there is a shortage of studies with consistent methods to assess the validity of teledentistry applications. For this systematic review, nine studies met the inclusion criteria to assess the validity of teledentistry compared to a traditional visual examination as a gold standard.
Furthermore, a cross-sectional design was used with only two randomized controlled trials that divided participants into control and intervention (teledentistry) groups. 12,13 The randomized controlled trial is preferable and therefore provides stronger evidence to support the validity of teledentistry. Both studies using the randomized controlled trial reported the teledentistry group not significantly different from the control group, supporting the validity of teledentistry. 12,13
Table 4 shows that most studies reported scores higher than 75% for sensitivity and specificity, indicating teledentistry screening could be comparable to traditional examination. However, few studies reported low sensitivity scores (<60%), 14,17,18 which indicate weak comparability to traditional examination. Thus, the majority of studies reported that the value of specificity and NPV was higher than sensitivity and PPV, indicating more true negative agreement between visual examination and teledentistry. These results mean that teledentistry assessment is more consistent with the visual examination in the assessment of sound teeth without any lesion.
In addition, Kappa statistics revealed that there was moderate to almost perfect measures of agreement between teledentistry and the visual examination (Table 4). Some studies reported that examiners found it difficult to detect oral lesions using photographs as detail on all teeth was not clear. Face-to-face interaction with patients was reported as an important factor that could result in moderate agreement between teledentistry screening and visual examination. However, the Kappa findings strengthen the assumption that the two modalities are comparable methods for use in dental examinations. These findings were also consistent with other studies investigating the reliability of teledentistry. 22,23
More than half (n = 5) the studies found teledentistry examination comparable to the traditional clinical examination when screening for dental caries. The teledentistry system was able to transmit a clear picture of teeth with dental caries to a doctor for the purpose of caries assessment. Interproximal caries was not evaluated in these studies because radiographs provide the best diagnosis unless the lesion spreads to the proximal from another tooth surface. Dental caries is one of the most prevalent chronic diseases causing tooth loss, pain, time away from school or work, and decrease in quality of life. 24 Also, dental caries is one of the most prevalent diseases among children. According to the Centers for Disease Control and Prevention, 28% of children between 2 and 5 years are affected by dental caries. 25 No statistically significant differences in early childhood caries detection between teledentistry and visual examinations have been reported. 16,12 Therefore, teledentistry is a viable technology for early diagnosis of dental caries among children. Teledentistry is cost effective for dental caries assessment to reduce the epidemic of dental caries among the population. 16
Teledentistry examination can be useful in rural areas where people cannot access dental services or specialists. Methodology in many of the articles transmitted oral images from remote sites for teledentistry screening. Distance diagnoses of oral lesions, such as dental caries, provided very good sensitivity and specificity scores. 12,15 –18 Teledentistry is not only an effective tool for dental examinations but can also increase access to dental specialist consultations and subsequent care. 2,26 Teledentistry provides access to dental care and reduces travel miles, costs, time, and suffering. 26 –28 Berndt et al. 29 found that interceptive orthodontic treatments delivered by trained general dentists remotely supervised by orthodontists through teledentistry are a feasible approach to treat the severity of malocclusions for underserved children with limited access to the specialist.
A 12-month teledentistry trial was conducted in general dentistry practices to evaluate the cost-effectiveness of teledentistry. 28 The study obtained costs associated with a visit to a dental practice, loss of productivity time, and accommodation expenses. Patients could lose about 2–12 hours of productivity by visiting distance dental offices. The study found that patients who live in rural areas could save about 900 Euro by implementing teledentistry in dental practices. 28
Time management is important to providers; therefore, teledentistry could improve time utilization to assess needs and perhaps provide care to those in rural areas. Teledentistry is a useful tool for consultations between providers providing electronic access to a patient's oral condition before the appointment time. The time saved would provide more time for treatment. 30 The findings of this review support dental professionals not being present physically with a patient to perform an oral assessment and treatment needs. This finding is consistent with a teledermatology study that reported a 69.05% agreement between teledermatology and face-to-face diagnosis, representing a high level of validity and considered a useful method for the diagnosis of distance patients reducing the face-to-face consultations by 40%. 31
The intraoral camera captured the dental detail for remote diagnoses in most studies. Intraoral cameras are not available in every practice; however, a smartphone camera can obtain images for remote diagnosis or assessment. Only one study used the mobile phone camera in this review. 18 Transmission of patient data over the Internet may require encryption. Furthermore, healthcare personnel are not to use personal camera phones for patient data. Most importantly, the quality of the photographic image is key to the validity for teledentistry adoption and application. Poor quality images reported lower sensitivity and specificity scores than higher quality photographs. 17 Low photographic quality might prevent the dental professional from accurate identification of treatment needs. An advantage of using good quality photographs obtained during a teledentistry assessment is that magnification on the computer can provide better detail of the image. Magnification and illumination provided by teledentistry were contributing factors to better accuracy in the examination over the visual examination. 16,32,33 Findings of this review were consistent with the findings of a systematic review to investigate whether photographic screenings were comparable to visual clinical examination. 9 Three studies in their review found photographic analysis superior to visual clinical inspection, while six studies found the two methods comparable. 9 Teledentistry use requires appropriate training of personnel to obtain and review quality images. To implement an accurate teledentistry system, training and quality equipment should be used to deliver accurate images to dental professionals. 34
Differences among dental professionals exist concerning use of teledentistry. Some professionals reported that they were not satisfied making a diagnosis using telecommunication images without clinical information. 13,20 Access to patient information is one of the main limitations that could affect the validity of teledentistry. Face-to-face examinations provide an opportunity to talk with patients to obtain information to assist with diagnosis. Lack of information could decrease the dental professional's confidence in making a diagnosis using a teledentistry system only and therefore, decrease the validity score of teledentistry. With the availability of videoconferencing, a consultation could occur in real time or after the review of oral images.
Furthermore, the experience of dental professional plays an important role in the ability to diagnose using teledentistry. Remote diagnosis by experienced professionals provided more accurate diagnosis than those with less experience. 19 Experience could affect the validity of teledentistry and increase or decrease the sensitivity or specificity scores. A teledentistry system could assist experienced specialists with consultations, provide a more accurate diagnosis to patients, and reduce untreated disease. These findings were consistent with previous studies that found no differences between intraexaminer agreements in treatment decisions when using teledentistry. 20,22,23
Limitations and Future Research
While the number of teledentistry studies is increasing, few use research methods and statistical analyses that can provide strong evidence for comparison of traditional visual examination to teledentistry examination. The searched databases and search terms might not identify all the studies published on teledentistry. The included studies were different in the area of application, settings, methods, equipment, and examiners. Therefore, because of the methodology variability among studies, it was difficult to generalize findings of this systematic review. Future studies need to look at standardization of cameras, examiners, settings, and type of statistical analyses to facilitate comparisons. Further research is essential to examine the accuracy of using live video in conjunction with photoconferencing for dental diagnosis and consultation. Further investigation is needed to enhance the quality of images to improve validity of teledentistry. This review suggests that more investigation to foster the validity of teledentistry outside the clinical setting is needed, such as the use of mobile phone cameras and a cost analysis to address savings from teledentistry.
Conclusions
Teledentistry examinations are valid, feasible, and comparable to visual examination for oral screening. Studies concluded that dental professionals make valid decisions about treatment based on a virtual examination. One study reported a loss of picture quality when using the telecommunication system, which could decrease diagnostic confidence, sensitivity, and specificity. Nevertheless, diagnostic collaboration between dental specialists using teledentistry could improve dental treatment and access to care.
Teledentistry is a valid tool to reduce inappropriate orthodontic referrals. 13 Teledentistry use in general dentistry does not appear to affect judgment of the dental professional significantly when compared to the judgment with a visual examination. Moreover, the same conclusion can be reached and appropriate decision regarding needed treatment and referral using the two modalities. Teledentistry could be a comparable tool to face-to-face technology for oral screening especially for school-based programs, caries assessment, referrals, and teleconsultations. Some studies reported low scores of sensitivity for teledentistry when compared to traditional clinical examination. Therefore, the validity of teledentistry in dental specialties requires further research.
Footnotes
Disclosure Statement
No competing financial interests exist.