
Abstract
Background:
Obstructive sleep apnea syndrome, a chronic respiratory disease, requires regular adherence to Continuous Positive Airway Pressure (CPAP) therapy. Telemonitoring may be relevant to support adherence, but nonetheless this raises ethical issues around the intrusive nature of the daily life of patients
Objective:
To explore the acceptance of telemonitoring by patients and the impact of this on adherence.
Materials and Methods:
A prospective and observational study has been performed with 160 patients who initiated their CPAP therapy. The acceptability of telemonitoring was studied using an attitudes' scale of 8 items. A total of 160 patients (111 men, 49 women) responded to the questionnaire at 1 month upon treatment. The adoption of both telemonitoring and adherence behavior were observed at 10 months of therapy.
Results:
A majority (78%) of patients expressed a favorable attitude toward telemonitoring, but nearly 40% consider this device like intrusive. However, at 10 months of treatment, 78% of patients are still telemonitored. We did not observe a significant difference between telemonitoring patients and nontelemonitoring patients with respect to the mean duration of use of CPAP therapy. However, the risk of stopping CPAP therapy is significantly more important in patients who refused telemonitoring.
Discussion and Conclusion:
It seems reductive to consider telemonitoring as a simple tool of surveillance to support adherence. It may be preferable to consider telemonitoring as a follow-up proposal. This will allow for more reactive management and close to the needs of the patients, in particular as telemonitoring is, in general, well accepted by patients.
Introduction
Obstructive sleep apnea syndrome (OSA), a chronic respiratory disease, causes to somnolence associated with increased cardiovascular risk in the long term. 1,2 OSA concerns 4% of the adult population 3 and mainly those between the age category of 50 and 60 years. 4 Continuous Positive Airway Pressure (CPAP) therapy, considered as the most effective treatment, 1,5 is a device that continuously sends air pressure into the airways through a mask, thus preventing the occurrence of apneic events during sleep. However, CPAP therapy can cause adverse effects such as rhinitis and skin problems. 6 CPAP treatment is palliative and requires at least 4 h of daily use so that patients can feel benefits on their energy status and on their quality of life 7 and by such reduce the risk of cardiovascular complications 8 –10 and the risks of work accidents 11 or traffic 12 . However, the rate of nonadherence, with a threshold set at 4 h per night, is estimated to be 20% at 3 months of treatment. 13
By consequence, to improve adherence to CPAP therapy, diverse technical adaptations and educational interventions have been evaluated. 14 With the emergence of new information and communication technologies, studies on telemedicine have brought new perspectives. Several telemedicine devices have been studied in the context of OSA. While telecommunication systems (automated calls and video telephony) appear to favor adherence to CPAP, 15 –17 the use of interactive applications by patients seems not to be very effective. 18,19 Moreover, the relevance of telemonitoring as support for adherence is not systematically found. 20,21 These studies are summarized in Table 1. Recently, the American Academy of Sleep Medicine emphasized the need for more research on the relevance of the use of telemedicine technologies in the context of OSA. 22
Studies Illustrate the Various Telemedicine Tools Tested in the Context of Obstructive Sleep Apnea Syndrome
p-Values not specified.
CG, control group; CPAP, Continuous Positive Airway Pressure; P-CG, placebo-controlled group; QoL, quality of life; RCT, randomized controlled trial; TG, telemedicine group; TLC-CPAP, telephone-linked communications for CPAP; UMC, usual medical care.
To improve the medical care of patients and to respond to the economic, health, and social challenge of adherence to CPAP, telemonitoring has been imposed on patients in France in October 2013. 23 The Ministry of Health and the Ministry of Economy decided to reduce unnecessary expenditure of social security by suspending the reimbursement for nonadherent patients. Hence, telemonitoring was a suitable tool for monitoring the actual use of CPAP therapy. This legal obligation immediately raised ethical debate in relation to the contentious nature of the transfer of particularly sensitive data. 25 At the request of patient associations and medical-technical providers, this obligation was rapidly suspended by the Council of State in February 2014. 26
Telemonitoring has thus become a simple follow-up proposal made by some healthcare providers, leaving the patient entirely free to either accept it or not. Through the daily transmission of data from the use of CPAP, telemonitoring would enable rapid intervention in case of difficulties with treatment. 27 However, in a randomized trial, Stepnowsky et al. compared adherence with CPAP and improved symptomatology of OSA between two groups of patients, telemonitoring (n = 20) and nontelemonitoring (n = 20). According to their results, no significant difference was observed between both groups: the use of the treatment and its efficacy were similar. As noted by the authors, these results may nevertheless be the consequence of the small sample of this pilot study. 20 Especially since the results of the randomized trial of Fox et al., comparing two larger groups of patients with CPAP telemonitored group (TG) n = 39 and nontelemonitored group (nTG) n = 36), showed a significant difference at 3 months of follow-up in favor of telemonitoring. 21 According to the review of the literature of Paré et al., telemonitoring appears to be well accepted by patients in many clinical contexts such as diabetes and hypertension. 27 Nevertheless, to our knowledge, only the study of Stepnowsky et al. briefly investigated the point of view of patients with OSA, assessing their general satisfaction and concern about telemonitoring, concluding that patients were satisfied and not worried by telemonitoring. 20
Thus, within this context of ethical and strategic doubts, our main objective was to explore the patient's attitudes toward telemonitoring, as well as the acceptance of this device. To focus the debate on the experiences of the patients, evaluation of patients' attitudes makes it possible to understand their latent dispositions, favorable or unfavorable, to the adoption of telemonitoring. 28 Second, we observed the extent to which the legal obligation of telemedicine could impair its acceptance and whether, ultimately, telemonitoring yields an influence on adherence to CPAP (Table 1).
Materials and Methods
To evaluate patient attitudes and to understand the acceptance of telemonitoring in the context of standard care, we conducted a prospective observational study of patients who were newly diagnosed with CPAP. The Committee for the Protection of Persons South East V (France), approved this study.
Population
Between October 2013 and December 2014, participation in the study was proposed to patients 30–80 years of age, diagnosed for OSA, by a polygraph and not concerned by the following exclusion criteria: patients already included in clinical study, during pregnancy or breastfeeding, following an associated oxygen therapy, who have already had experience with OSA treatments, with a history of stroke with aphasia, or adults under trusteeship. The recruitment took place over 1 year and 3 months, within two AGIR à dom. Agencies (Grenoble and Chambéry, France), a medical–technical provider. Patients who agreed to participate in the study signed the informed consent in accordance with the World Medical Association Revised Declaration of Helsinki. As mentioned above, telemonitoring was proposed to patients after February 2014. The study population consists of two groups: (1) a group of 52 patients who started their treatment between October 2013 and February 2014 for which the telemonitoring was imposed (IG or imposed group) and (2) a group of 108 patients treated after February 2014 for which surveillance was proposed (PG or proposed group).
Procedure
Patients who agreed to participate in the study benefited from the usual follow-up of the medical–technical provider. The frequency of appointments was the same for both telemonitoring and nontelemonitoring patients (day 0, day 7, day 30, month 4, and month 10). For telemonitoring patients, a modem was installed either on the initiation day or 1 week later. Professionals could consult data on the use and effectiveness of CPAP outside of traditional appointments. When the professionals observed a low use of the device or a lack of efficiency beyond 3 days [high residual Apnea-Hypopnea Index [AHI] and/or large Mask Leakage], they contacted the patients by telephone to understand the problem and if necessary, organized a technical intervention.
Patients' attitudes toward telemonitoring were evaluated using a self-administered questionnaire at 1 month of treatment, appointment performed in an agency or at home, according to the modality of follow-up. Sociodemographic and medical data were collected from patients: conjugal status, occupational status, and cardiovascular comorbidities. The remaining sociodemographic and medical data were collected from the patient file: age, sex, lifestyle, type of follow-up, AHI, body mass index, and Epworth daytime sleepiness score. 29 Use and therapeutic efficacy data were downloaded from the CPAP processing memory card. At 10 months of treatment, we collected residual AHI, the presence of significant leakage, as well as the following compliance data from the last 28 days: average usage, percentage of days of nonuse, and percentage of days of use below 4 h. We noted the date of stopping CPAP therapy during the study period.
Tools
The questionnaire of attitudes is a semantic differential scale, composed of eight peers of opposite adjectives. The indicators of the questionnaire were selected from the review of the literature, 16,20,30 but also to a committee composed of 20 professionals from AGIR à dom. After a pretest with 30 patients, the following eight adjective peers were selected: useful/harmful, justified/aberrant, discreet/cumbersome, motivating/demotivating, nonintrusive/intrusive, reassuring/stressful, effective/ineffective, and necessary/superfluous. Patients were asked to answer the following question for each pair of adjectives on Osgood rating method: “For me, the presence of telemonitoring modem is: −3 = very harmful; +3 = very useful.”
Statistical Analyses
Analyses were carried out using the software SPSS Statistic 20. Informatics problems hindered the collection of usage data for six patients (3.8% of missing data), which we replaced by the median. Early descriptive analyses were conducted to explore the scores obtained on the attitudes scale. We also compared subgroups of patients to understand the acceptance of telemonitoring: the Pearson's chi-squared test was used for the categorical variables and the nonparametric U test of Mann-Whitney for the quantitative variables, not following the normal distribution. Logistic regressions were not only done to understand the factors associated with the acceptance of telemonitoring, but also to evaluate if telemonitoring avoids nonadherence or abandons CPAP therapy.
Results
Presentation of the Population Study
The sociodemographic and medical characteristics of the 160 participants are presented in Table 2. Due to the legislative change during the study, our sample is composed of two groups: the IG of 52 patients (32.5%) and the PG of 108 patients (67.5%). Nobody of IG refused CPAP therapy with the obligation of monitoring. For the PG, the initial adoption rate for telemonitoring was 77%. At 10 months of treatment, more than three quarters of the patients, still with CPAP therapy, were telemonitored (n = 111 or 78%). Our sample is composed of different subgroups of patients (Fig. 1), for which we studied sociodemographic, medical, attitudinal, and behavioral differences.
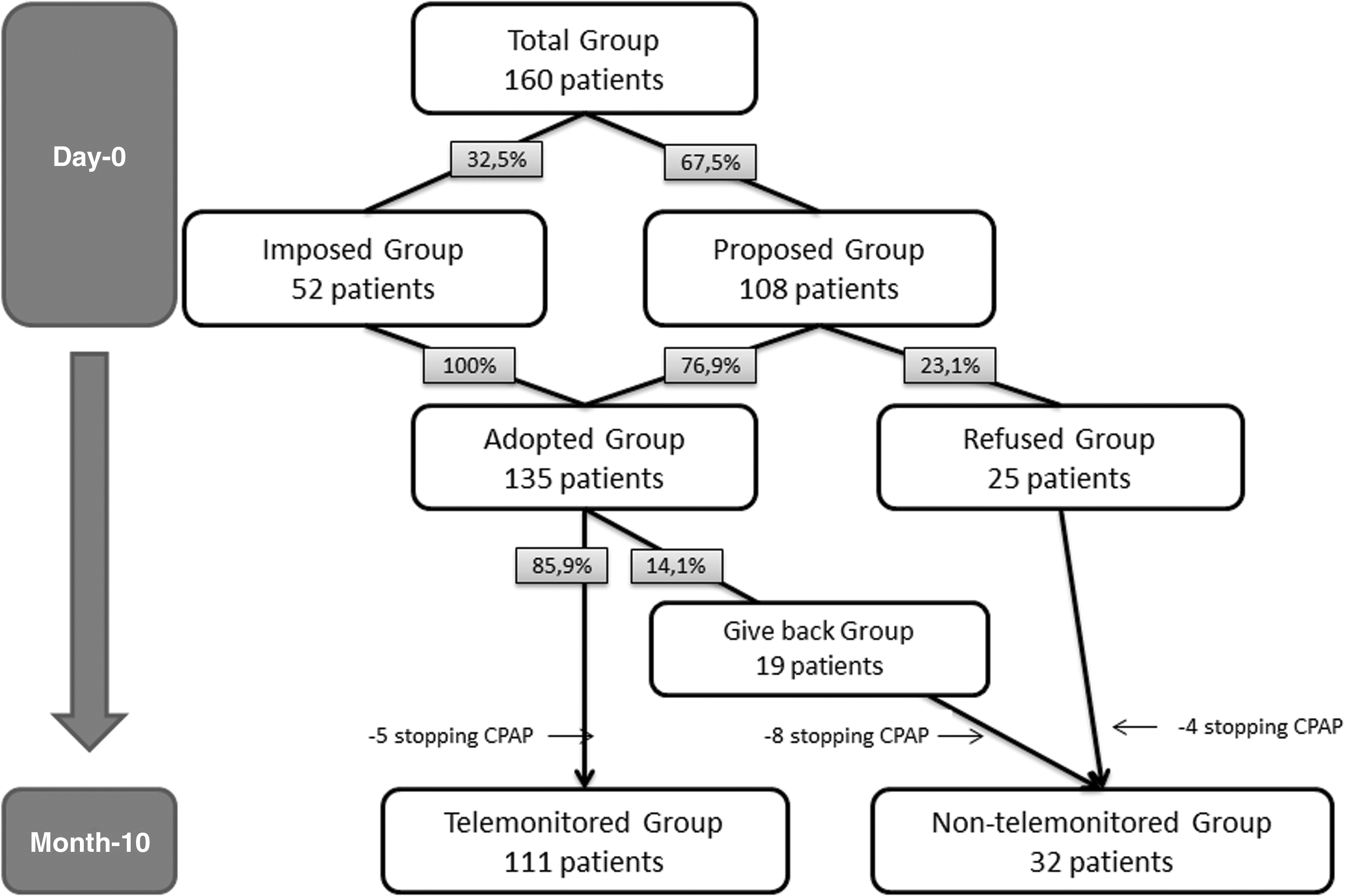
Composition of the sample during the study. CPAP, Continuous Positive Airway Pressure.
Baseline Patient's Characteristics
AHI, Apnea–Hypopnea Index; BMI, body mass index; SD, standard deviation.
Attitudes Toward Telemonitoring
We evaluated the latent disposition of patients about telemonitoring, using an attitudes' scale with internal consistency acceptable (Cronbach's alpha = 0.86). Over the full sample, the majority of patients expressed an attitude favorable toward telemonitoring, with an average score of 8.1 out of 24 [standard deviation (SD) = 9.6, minimum = −18, maximum = 24). Nevertheless, 22% of patients score was ≤0, meaning a “very unfavorable” to “mixed” attitude toward telemonitoring. Figure 2 illustrates the distribution of the population according to the observed score on attitudes scale. We found two significant differences by comparing these scores according to the sociodemographic and medical data: (1) men have a more favorable attitude toward telemonitoring than women (p = 0.03) and (2) nonworking people are more favorable toward telemonitoring than active people (p = 0.04). On the basis of the results obtained for each item, we observed that telemonitoring is mainly perceived as justified and useful, but nearly 40% of the patients consider this device like intrusive (Fig. 3).

Distribution of patients according to their scores on the attitudes scale.
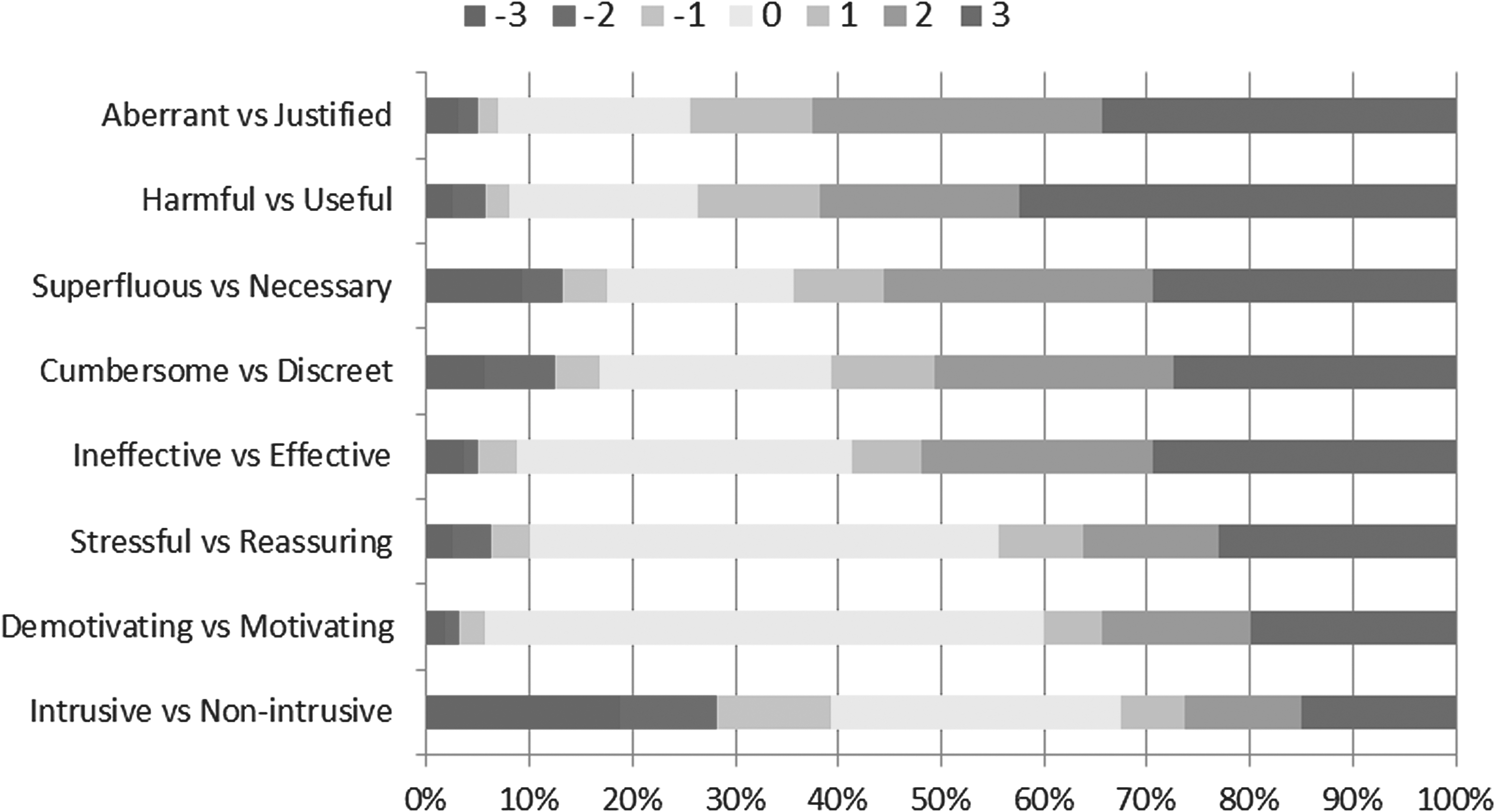
Distribution of patients according to the score obtained for each pair of opposing adjectives.
Acceptance of Telemonitoring
To understand the factors associated with the acceptance of telemonitoring, we compared the patients who adopted it (AG or adopted group) to those who refused it (RG or refused group) at the start of CPAP therapy. The analysis only concerns the data of the PG (n = 108) due to the legal duty of telemonitoring for IG. The sociodemographic, medical, and attitudinal data for both subgroups are presented in Table 3. We can observe that the proportion of retired patients is significantly higher in AG than in RG. More of the working people have rejected telemonitoring than retired people (31% vs. 15%). In addition, patients who refused the telemonitoring were significantly more unfavorable than the patients who adopted it.
Comparison of Subgroups: Initial Acceptance of Telemonitoring (n = 108)
Analysis carried out on PG (n = 108).
Numbers shown in bold denote significant values.
AG, adopted group; PG, proposed group; RG, refused group.
Using a logistic regression model, we assessed the extent to which attitudes are associated with the initial acceptance of telemonitoring. We incorporated the covariables, gender and occupational status, because of the more favorable attitudes found among men and retired people. The results, presented in Table 4, show that an initially very unfavorable attitude is associated with more refusals of telemonitoring.
Logistic Regression, Modeling the Risk of Refusal of Telemonitoring (n = 108)
Numbers shown in bold denote significant values.
CI, confidence interval; OR, odds ratio.
The Impact of the Legal Obligation on the Acceptance of Telemonitoring
Unexpectedly, the patients of IG have a more favorable attitude toward this telemedicine device, unlike patients in PG (p = 0.03). The results show that these patients perceive telemonitoring as more useful (p = 0.02), more justified (p = 0.02), and necessary (p = 0.04), but also less intrusive (p = 0.02). What differentiates the IG from the PG is the start date of the treatment, but unexpectedly there are other significant differences between both groups, for AHI and the presence of cardiovascular comorbidities. Patients of IG had a higher AHI (p = 0.04) and had fewer cardiovascular comorbidities (p = 0.03). However, we observed that these medical variables do not have a significant influence on the general attitudes of patients from a linear regression, contrary to the imposition of telemonitoring, which is positively associated with a better attitude (Table 5). In addition, more than 91% of the patients in the IG are still telemonitored at 10 months of treatment, a proportion significantly higher than that of the PG (p = 0.007).
Linear Regression, Influence of Medical Data on Attitudes (n = 160)
R2 = 0.053 (adjusted R2 = 0.035).
Numbers shown in bold denote significant values.
Telemonitoring as a Support for Patient Adherence
On the overall sample, the proportion of adherent patients was 70%, that is, 111 patients out of 160. Seventeen patients stopped CPAP therapy and 32 patients (20%) were nonadherents at 10 months of treatment. Of the 135 patients who started their CPAP therapy with telemonitoring, 19 patients (14%) no longer wanted to be monitored during their treatment. At 10 months of treatment, 143 patients are still treated with CPAP, 78% of which were telemonitored. We found no significant differences in the sociodemographic and medical variables between TG and nTG at 10 months of treatment. We also found no significant differences in the use of CPAP between both groups (Table 6).
Comparison of the Continuous Positive Airway Pressure Use According to Telemonitoring at 10 Months (n = 143)
Twelve missing data n = 131.
nTG, nontelemonitored group; TG, telemonitored group.
These results are confirmed by a logistic regression model that evaluates the risk of nonadherence on condition, telemonitoring is refused (RG), kept (KG), or given back (GbG) within 10 months (n = 143; Statistic of Wald = 3.307; p = 0.19). Nevertheless, the risk of therapeutic failure is increased according to the acceptance of telemonitoring (Table 7). Indeed, the risk of stopping CPAP therapy is 4 times greater in patients who initially refused the telemonitoring and 16 times more important in patients having given back the telemonitoring device.
Logistic Regression, Modeling Therapeutic Abandonment Risk (n = 160)
Numbers shown in bold denotes significant values.
Discussion
We have submitted an attitude scale to 160 patients to explore the acceptability of telemonitoring. The study sample respects the gender ratio (one woman for two men), as well as the average age of people with OSA, according to epidemiological data. 3,4 The observational approach of our study leads to a multiplicity of subgroups, limiting statistical analyses. However, this allows us to understand the acceptance of telemonitoring and its evolution in standard care. Another limit of our study is a single measure of attitude: we have submitted in this study the attitude scale at 1 month of therapy. Of course, measurements at other time points would enrich our approach. The attitudes' scale developed for this study, with acceptable internal consistency, has been shown to be relevant to understanding the adoption of telemonitoring.
The adoption of telemonitoring is correct, since 78% of patients are still telemonitored at 10 months of treatment. As found in the literature, 20,27 the majority of patients are favorable to this device, which is perceived as justified, useful, and necessary. Thus, the economic and social interests of telemonitoring are appreciated by patients, despite the intrusive character evoked by nearly 40% of them. The disputed and nonethical nature mentioned during the suspension of the legal obligation is not highlighted by our results. Indeed, in agreement with the conclusions of Stepnowsky et al., this device of telemedicine is experienced as stressful by a minority of patients. 20
The nonacceptance of telemonitoring by patients is associated with less favorable attitudes. This minority of patients does not consider telemonitoring to be justified and necessary and referred more intrusive and stressful nature of being telemonitored. At the same time, we observed that the retired patients adopt significantly more telemonitoring than active patients, while age is not associated with the adoption of the system. The fact of being monitored remotely by professionals thus seems to be better accepted by the patients staying longer time at home.
The special feature of this study is due to a legislative change in France, which led to the formation of two subgroups: imposed telemonitoring group and proposed telemonitoring group. What could have constituted a sampling bias, in fact, allowed us to evaluate the impact of a legal imperative on patients' attitudes. Contrary to our initial hypothesis, patients in the imposed telemonitoring group were not only positive, but also significantly better than those in the proposed telemonitoring group. These counterintuitive results could be the result of the avoidance of cognitive dissonance. 31 The legal obligation is internalized, integrated by the individual, to avoid a psychological discomfort. Moreover, the effect of this legal imperative is found in the long term since the rate of telemonitored patients is significantly greater in the IG at 10 months.
In a second step, we studied the impact of telemonitoring on the long-term use of CPAP therapy. The proportion of nonadherent patients in this study (20%) corresponds to the nonadherence rate found in the literature. 13 Based on our analysis of the frequency and duration of CPAP's use, it appears that telemonitoring does not promote adherence to treatment. These results are congruent with those presented by Stepnowsky et al., 20 but differ from the study of Fox et al. 21 These results are consistent with the perceptions of patients who do not consider this device as a motivational vector to use CPAP therapy. Moreover, we do not observe better treatment efficacy for telemonitored patients; this also strengthens the conclusions of Stepnowsky et al. although with a smaller number of patients. 20 This difference between nonadherence and nonpersistence of CPAP therapy, could in part explain the contradictory results found in the literature. 20,21 Although a little impact on the low use of CPAP therapy, it would seem that telemonitoring has a real protective interest against therapeutic failure in the OSA context.
According to the results of our study, from the viewpoint of patients, it seems reductive to consider telemonitoring like a simple tool of surveillance to address the economic issues of nonadherence. Indeed, it would probably be more realistic to envisage this technology as a follow-up proposal, allowing a more responsive care and closer to the needs of patients, especially since telemonitoring is generally well accepted.
Footnotes
Acknowledgments
This study is part of a research protocol on the psychosocial factors of nonadherence with Continuous Positive Airway Pressure (CPAP) treatment, the ACCEPTability of ApNEA (ACCEPTNEA) protocol promoted by AGIR à dom. Assistance, medical–technical service providers at home, with Convention Industrielle de Formation par la REcherche (CIFRE) funding from the National Association of Research Technology. The authors sincerely thank Dr. Petrus J. Pauwels for fruitful discussion and for proofreading the English version.
Disclosure Statement
No competing financial interests exist.