
Abstract
Background/Introduction:
Never before have parents had such immediate access to parenting support. The extension of the Internet to smartphones, offers the opportunity to provide families with the highest-quality information at the time and place that it can be the most useful. However, there remain considerable barriers to getting the right information to the right people at the right time.
Materials and Methods:
This study includes the initial feasibility testing of a smartphone application “ParentNet” that attempts to deliver on the potential of empirically supported therapy by connecting family members with specific behavioral goals and outcomes in real time. Participation was solicited from community parenting support groups and through online social media. Data were collected from 73 parents and 88 children on child behavior (adult only) and satisfaction.
Results:
Data analyses showed positive satisfaction and utilization results: (1) users rated the ParentNet app very positively (i.e., 85% of caregivers and 88% of youth would recommend the app to others), and (2) parenting behavior was improved with a small/moderate effect-size.
Discussion and Conclusions:
Findings from this initial testing are reviewed along with future development possibilities to be considered. Limitations of small pilot sample and brief administration period could have reduced effects. Further study would include a more robust sample.
Introduction
There is a strong body of evidence supporting the use of behavioral parenting strategies in dealing with child behavioral problems. 1,2 Empirically supported behavioral parent training (BPT) protocols exist to teach parents how to employ these strategies. 3 –7 However, there is also a large amount of misinformation, opinion, and conflicting ideas concurrently being disseminated.
The Internet has made the process of getting accurate, best-practice information harder rather than less cumbersome because of the overwhelming amount and variable quality of parenting information available. A Google search of “parent/parenting” produces 827,000,000 results, “behavioral parenting” reduces this is 46,700,000, and “empirically validated behavioral parenting” still returns 922,000 results (search conducted using Google Chrome November 5, 2016). Not only is this volume intimidating, but the results are often sorted by algorithms that do little to account for the quality of the information included. Parents need a resource to receive trustworthy information in a digestible format that would assist them in being able to use the resulting information to develop behavioral programs for their children.
As important as accurate information is implementation integrity. An effective empirically supported behavior plan is faced with numerous barriers to consistent implementation. There are a wide variety of factors that can interfere with the implementation of even the strongest parenting strategies, and both needing timely reminders and tracking the details 8 are frequently noted. These barriers, however, are also noted as exactly the kinds of factors that technology is often able to address. 9,10
In an attempt to overcome these barriers, we developed and began testing an application “ParentNet” that is intended to help parents to utilize best practices in behavioral parenting to create personalized, specific programs for their children. After the behavioral program has been created, ParentNet helps family members track timelines, incentives, and other details to assist parents in maintaining the program they have created. An initial proof-of-concept mobile/Internet version of this program and reminder set was developed and tested with a group of parents of children with challenging behaviors.
Child Antisocial Behavior and Parenting
Antisocial behavior in children (e.g., conduct and disruptive behavior disorders) represents a substantial financial, emotional, and educational problem for society. 11 –14 Conduct Disorder is typically more common among boys with prevalence estimates ranging from 2.1% to 8.8% for boys and from 0% to 1.4% for girls. 15 –17 Research has shown that poor parenting contributes significantly to adolescent risk for problem behavior, while consistent discipline practices and monitoring, parental involvement, positive parenting practices, and clear communication lower the risk of behavior problems and illicit drug use throughout adolescence. 18 –24
Behavior Parent Training
The well-established empirical and theoretical links between child disruptive behaviors, parenting practices, and family relationships have given rise to the development and evaluation of family-based interventions for the treatment of conduct and substance use disorders. In particular, with nearly 30 years of research support, behavioral interventions such as BPT have been established as best practices for disruptive behavior disorders including oppositional defiant disorder, conduct disorder, and drug abuse. 1,2,5,6,25,26 The benefits of parent training interventions have been documented for a wide variety of child conduct behaviors and for parents with diverse problems, including alcoholism, 27 divorced families, 28 and blended families. 29 These intervention strategies include the reinforcement of appropriate and “on target” behaviors as the primary catalyst to improve child behavior. Positive parent–child interactions create a foundation from which to build effective interventions.
Using the Internet to Increase Service Accessibility
The problem of service inaccessibility for youth and families, especially ethnic minorities and those living in rural areas, historically has cut across all sectors of healthcare. Medical healthcare providers were among the first, however, to envision using the Internet as a means of providing services to displaced or marginalized patients. 30,31 Although the use of the Internet for healthcare service delivery has been gaining strong momentum in the medical field, and in psychiatry in particular, for several decades, the expansion of this service delivery model into the domains of psychosocial and behavioral intervention has been much slower, particularly for children and adolescents. In fact, studies of Internet-based interventions for any type of child or adolescent disorder remain remarkably limited. 32,33
As of January 2017, 77% of American adults have a smartphone, up from 35% in the spring of 2011. 34 The use of a smartphone application to assist parents would be innovative in bringing together information, intervention, and feedback to parents through the use of the Internet, providing empirically supported practices to parents of children and adolescents with behavior disorders. We believe that digital technologies offer an important opportunity for population penetration, based on a solid understanding of the relevant family developmental science, prevention principles related to behavior and relationship change, and the capacities, advantages, and limits of digital technologies.
Conceptual Model of Change
Perhaps the most formidable barriers to seeing sustained effects are parenting issues: (1) defining effective goals and unrealistic expectations, (2) delineating pro-social behaviors and positive reinforcers, (3) maintaining effective follow-through, (4) maintaining communication across people (parents, caregivers, teachers, and child), and (5) youth buy-in. A conceptual model of the change process in the intervention to increase effective implementation is shown in Table 1. ParentNet was designed to specifically address these barriers through a Web portal and integrated smartphone application, which allows multiple family members real-time access to behavioral data. By virtue of the ParentNet system, parents will be able to implement BPT with much higher fidelity. These fidelity gains, in turn, will directly improve their parenting behavior, leading to healthier family functioning and a reduction in teen behavior problems.
Conceptual Model of Change
The purpose of this system is to make it easier for parents to do the kinds of daily parenting activities that they already know how to do. Most parents know that raising children requires consistency and clarity in our behavioral expectations. Parents know that if they sometimes allow a later bedtime, then it is not surprising that the children may request or beg for this treatment on other nights. However, in our day-to-day lives it is easy to get distracted by the thousand minor tasks that parents are called upon to complete: checking children's homework, making sure dinner is on the table, that the laundry is done, and that youth are at their sports practices on time. Parents are pulled in so many directions at the same time that it is impossible to keep track of it all. In our work lives we all have different systems, but at some level we all use calendars, assistants, post-it notes, and reminders to help us keep up with all of the tasks that we set out to accomplish.
Research Aims
The focus of this research was on translating empirically supported BPT skills into a coordinated ParentNet system, through an iterative feedback/revision development methodology and then test for feasibility/usability among caregivers of high-risk youth, ages 8–12 years. The system was intended to promote clarity in behavioral expectations, increase consistency and follow through, and allow increased communication between parents, children, caregivers, teachers, and clinical staff to encourage positive behaviors and decrease negative behaviors. Features included (1) training in developing a behavioral system, (2) push reminders across users (parents and children), (3) calendar functions, and (4) Web site management by users and administrators. The application started with cross platform mobile (i.e., Android and iOS). After the initial design and testing, focus groups were conducted to add qualitative feedback concerning the design and potential future development of the ParentNet system.
Materials and Methods
Participants
ParentNet outcomes were assessed with measures administered to parents/caregivers and child users. Data were collected from 73 parents and 88 children. Participation was solicited from community parenting support groups and through online social media. Parents averaged 44.77 years of age [standard deviation (SD) = 10.08] and most (77%) were female. The participating parents were 89% Caucasian, 3% American Indian, and 3% multiracial with 1% reporting their ethnicity as Hispanic/Latino, and 4% electing to not report race/ethnicity. Fifty-four percent were married, 63% had two adults living at home, 29% reported household incomes as less than $25,000, and 32% with incomes between $25,000 and $50,000 per year. Fifty percent of parents reported “some difficulty paying bills each month.” The children were reported by their parents to be 81% Caucasian, 3% American Indian, 2% African American, and 7% multiracial with 3% reporting their child's ethnicity as Hispanic/Latino, and again with 4% electing to not report.
Parents believed themselves to be fairly computer literate with 60% reporting that they were “very comfortable with computers” and averaged 15.30 h (SD = 7.14) of computer use per week. Eighty-nine percent of parents use the Internet daily, 67% of parents reported using Facebook on a daily basis and 70% use smartphone applications daily. Caregivers rated their children as high-risk with a mean Total Problems on the Strengths and Difficulties Questionnaire (SDQ 35 ) of 15.37 (SD = 6.13), which is in the “borderline” range of conduct problems. Scores on the Parenting Scale (PS) 36 were in the borderline region, with an average of 3.00 (SD = 0.59) where the clinical cutoff is 3.20.
After completing informed consent procedures and T1 (baseline) assessment, participating families were randomly assigned to (1) ParentNet/experimental/immediate-implementation or (2) wait-list/control conditions. All families were offered a preloaded smartphone and 1-month prepaid phone plan to participate if they did not already have a phone. The majority of families elected to use their own devices to access the application, and only seven families requested the use of project phones. Parents and youth also received monetary compensation for participation. The experimental group used ParentNet for 4 weeks before research staff collected T2 (post) measures. Control group families completed the T2 measures 4 weeks after T1 assessments, then received access to ParentNet for 4 weeks. Fifty-six families were randomly assigned to a condition with a final N of 42 (i.e., primary caregiver who completed both T1 and T2 assessments; 20 in Experimental and 22 in Control groups), resulting in a 25% attrition rate.
Developed Structure of Parentnet
Using our experience with previous Internet-based interventions, we developed a graphic user interface that is both appealing and easy to navigate (Fig. 1). The ParentNet system's Caregiver Home Dashboard contains an icon/picture for each child and a list of pending/completed behaviors that the parent can either approve or ask for follow-up (green thumbs up or red thumbs down). The back arrow in the upper left of the Home dashboard allows the caregiver to invite others to link to the family account. Selecting a child's icon/picture brings the caregiver to Child Summary. The Child Summary has the child's access code information (for youth without a smartphone or email account), total points earned, rewards and behaviors/task tracking. The Child Summary page serves as the anchor for each child's information and much of the application navigation begins and ends here. Tapping/clicking on the blue pencil icon in the bar by the youth's name allows the caregiver to edit child information: sticker set (points, marbles, or stars), upload profile image, and behavior/tasks. Tapping/clicking on the blue chart icon on the Child Summary page brings the caregiver to the Child Chart Screen showing behaviors due and completed per day or week with corresponding point values. Caregivers can also indicate behaviors that have been completed on the Child Chart Screen.
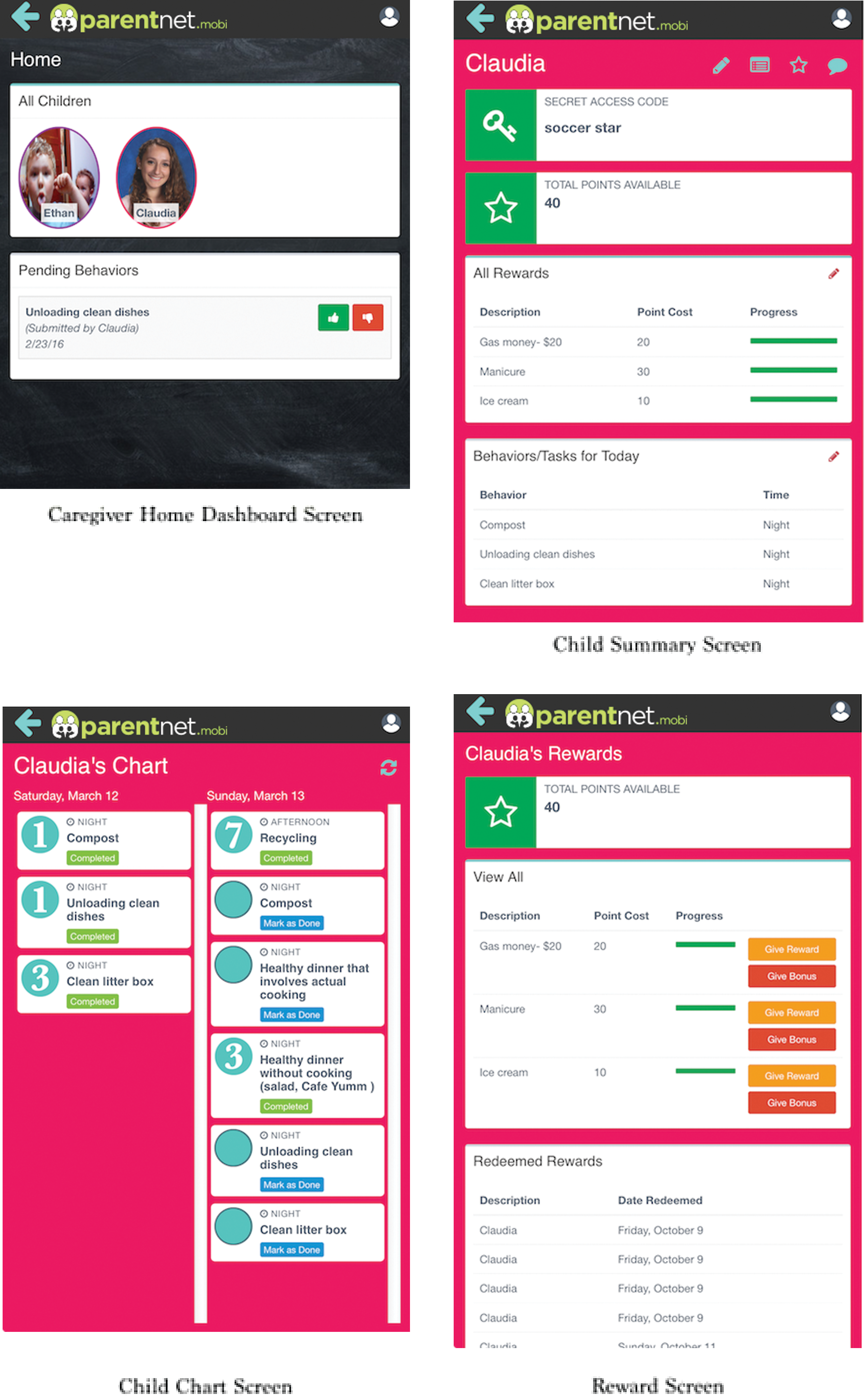
ParentNet Screens. Color images available online at
In the pictured example, Claudia is tracking completed behaviors using points (the large numbers to the left of the listed behaviors) to earn rewards. Selecting the blue star icon on the Child Summary brings the caregiver to the Reward Screen. On the Reward Screen, the caregiver can assign a previously defined reward for a completed behavior and can choose to give a bonus for additional positive reinforcement. The Reward Screen also allows the caregiver to see a history of redeemed rewards. The caregiver can allow and personalize the frequency of reminders (within app and push notifications) for both themselves and their child via a branching series of drop down menus. Initially, parents are guided through this series of screens to create a child behavior and reward, but later parents are able to edit their child's program starting at any point.
Measures
T1 (baseline) and T2 (post) measures included child behavior (SDQ 35 ) and parenting (PS 36 ). SDQ is a brief valid and reliable parent-report questionnaire about child behavior (aged 4–16 years) that can be completed in about 5 min. The instrument assesses child challenging behavior and competencies. Scores from the SDQ and CBCL 35 and the Rutter Questionnaire 37 are highly correlated. The SDQ has high discriminant validity, and it is sensitive to both child internalizing and externalizing behavior. The PS includes two subscales that measure lax and overly reactive parental discipline. These two subscales, consisting of 10 items each, demonstrate adequate internal consistency, test-retest reliability, and construct validity. They also have been shown to be sensitive to change as a function of parent training interventions. 38 In addition, we collected data on utilization, satisfaction, ease ofuse, marketing, and general impressions from focus groups.
Results
Parentnet Utilization
Caregivers and children actively used the application during the research period. Across the 4 weeks of testing, caregivers had an average of 34.35 sessions (SD = 36.66) and each session lasted an average of 2.84 min (SD = 2.42) with an average of 8.32 interactions (SD = 4.85) per session (interaction defined as any discrete data entry by the participant; did not count sessions in which the application was opened but no other manipulation occurred). Children had an average of 21.75 sessions (SD = 13.53) and each session lasted an average of 1.38 min (SD = 1.99) with an average of 3.33 interactions (SD = 2.20) per session. During the testing, caregivers created a total of 314 behaviors/tasks for their children. Ninety-eight rewards were redeemed by children and approved by caregivers. Caregivers completed 97 daily behavior reports on their own prompting during the pilot research period. This high activity illustrates the high usability of ParentNet for both parents and children.
Overall Parentnet Satisfaction and Ease of Use
We were very encouraged by the positive ratings and comments we received from participants. Eighty-five percent of caregivers and 88% of youth reported that they would recommend ParentNet to others. Seventy-one percent of caregivers found ParentNet helpful for tracking children's behaviors and providing rewards. Forty-seven percent felt that ParentNet helped positively change their parenting behavior.
Caregiver comments included: “I am glad that I am able to keep the program and hope to try it to change some of my own behaviors” and “I enjoyed showing her (my daughter) the points she earned and discussing what rewards to redeem, it was fun.” Parents with children who did not complete tasks still found ParentNet helpful: “When my daughter wanted to do things and she hadn't done her chores, we had a point of reference to look at.” As well, even parents who were not as engaged found ParentNet to be useful: “My wife is the primary caregiver of the kids… so… this was more for her than for me. I did check it a few times to see if my daughter had done her chores and things… so that was useful.”
Comments from children also showed a positive view of ParentNet: “The whole concept of ParentNet is very useful and important, because it reminded me to do my chores and it persuaded me to do more than just those few chores,” “The useful thing about the ParentNet app is that it made sense,” and “The system that you get a job, and they are all in one place.” With this high level of satisfaction and ease of use, we are positioned for a viable and successful commercial product.
Parenting Behaviors
We are very encouraged and impressed that we were able to make a small/moderate effect-size change in parenting behaviors. Figure 2 shows the T1 (baseline) and T2 (post) scores on the PS Total Negative. The experimental group's scores decreased while the control group increased slightly. While this effect was not significant (F(1,40) = 1.13, p = 0.29), the trend and direction of effect was very encouraging. On the PS Hostility subscale, we found a small/medium effect-size with an η2 of 0.06. Given the short intervention period and “light-touch” of the program, we were surprised with such a high potential for significance in an adequately powered randomized control trial. Interestingly, 40% of caregivers reported that they believed ParentNet prompted a productive conversation between themselves and their children.
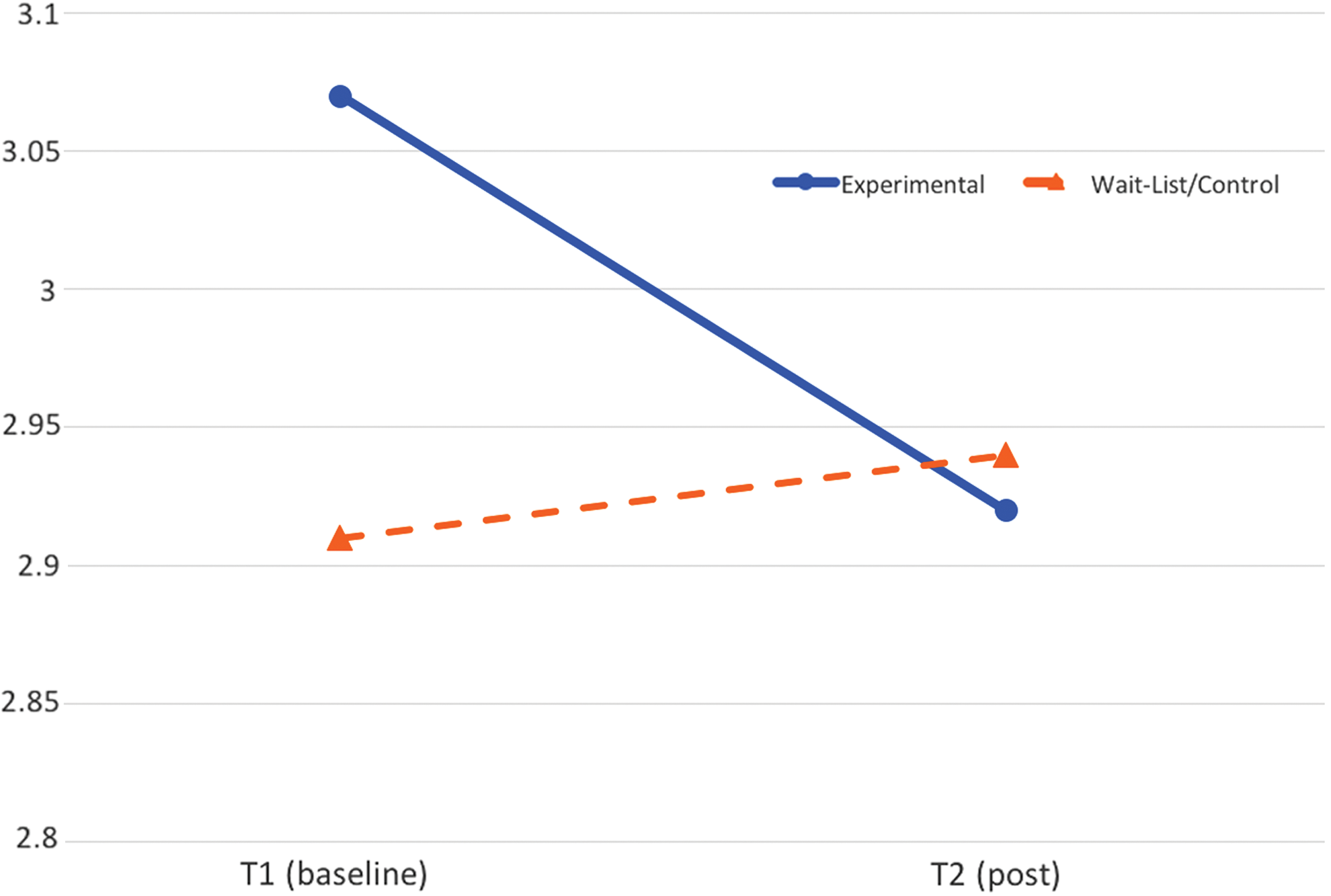
Parenting Scale Total Negative Pre and Post by Condition. Color images available online at
Discussion
The research team was able to develop and test a user friendly and secure system using state-of-art computer-based protocols for utilization of BPT best-practices. We are encouraged by the positive satisfaction and utilization results that (1) users rate the app very positively (i.e., 85% of caregivers and 88% of youth would recommend the app to others), and (2) parenting behavior was improved with a small/moderate effect-size with a very small pilot sample with a brief administration period. Limitations include our lack of documentation for the costs, lack of direct observation of behavior changes by the subjects, and lack of significant results due to the small number of subjects.
This test, while limited in scope and generalizability, does seem to lay an initial foundation for the use of behavioral parenting tools to be deployed to smartphones and other mobile devices. Our ability to reach families in real time with best practice information holds the potential to be a categorical shift in the ability to work effectively with families and for parents to overcome some of the most common barriers to effective parenting. Parents of youth with behavioral difficulties often report feelings of isolation and lacking resources. The development of a mechanism for connecting caregivers and youth in real time and to track progress toward clinical goals opens a variety of possibilities for future development of this and other tools. With the positive findings from the pilot study and focus group, this group has been encouraged to continue development of the ParentNet system. We would like to add accessibility for Spanish-speaking families.
Footnotes
Acknowledgments
The authors acknowledge the support of this research by grant number 1R43HD081831 from the National Institute of Child Health and Development.
Disclosure Statement
Drs. Feil and Sprengelmeyer are co-owners of Effective Human Services, LLC.