
Abstract
Objective:
To assess the use of Teledentistry (TD) in delivering specialist dental services at the Royal Children's Hospital (RCH) for rural and regional patients and to conduct an economic evaluation by building a decision model to estimate the costs and effectiveness of Teledental consultations compared with standard consultations at the RCH.
Methods:
A model-based analysis was conducted to determine the potential costs of implementing TD at the RCH. The outcome measure was timely consultations (whether the patient presented within an appropriate time according to the recommended schedule). Dental records at the RCH of those who presented for orthodontic or pediatric dental consultations were assessed. A cost-effectiveness analysis (CEA), comparing TD with the traditional method of consultation, was conducted. One-way sensitivity analysis was performed to test the robustness of the results.
Results and Materials:
A total of 367 TD appropriate consultations were identified, of which 241 were timely (65.7%). The mean cost of a RCH consultation was A$431.29, with the mean TD consult costing A$294.35. This represents a cost saving of A$136.95 per appointment. The CEA found TD to be a dominant option, with cost savings of A$3,160.81 for every additional timely consult. The model indicated that 36.7 days of clinic time may be freed up at the RCH to treat other patients and expand capacity. These results were robust when performing one-way sensitivity analysis.
Conclusion:
When taking a societal perspective, the implementation of TD is likely to be a cost-effective alternative compared with the standard practice of face-to-face consultation at the RCH.
Introduction
Teledentistry (TD) is the branch of telehealth that supports oral healthcare delivery through the organization, management, and distribution of health information in support of patient and professional health-related education, practice, public health, research, healthcare administration, information gathering and synthesis, and knowledge sharing. 1,2
TD has been applied in many areas of clinical dentistry, including pediatric orthodontic patients, and has been found to be a valid method for teleconsultation and referral. 3 In addition, evidence indicates that TD is comparable to visual/tactile examinations for dental caries screening. 4 Moreover, TD offers an alternative to face-to-face dental consultation and has the ability to improve access to oral healthcare, especially the access to specialist oral healthcare services where geographical distance and limited local resources result in a lack of specialist services in these areas. 5 –9 This ultimately should improve equality of oral healthcare and lower its costs. 9 –11
One area of application is for those who require management of Cleft Lip and Palate (CL&P). CL&P is seen in one in every 830 babies in Victoria. 12 The dental management of CL&P patients can involve multiple consultations to determine coordinated timing for orthodontic and surgical treatment in addition to the standard dental care and annual follow-ups. In Victoria, The Royal Children's Hospital (RCH) Department of Dentistry (RCH-DD) provides the bulk of specialist dental services for children and adolescents in the management of CL&P.
A field study into using TD consultations for a pediatric population was conducted at the RCH. The study demonstrated that TD can improve access to specialist dental care and can save time, concern, and money by avoiding travel to the central hospital for consultation. 6 In addition, this would also mean that the hospital could increase its capacity to provide dental services for minimal extra infrastructure costs.
While the potential benefits of TD have been identified and demonstrated, there has been minimal research done on the economic evaluation of TD and it has been marked as an area requiring further research. 8,13 The present study aims to take a societal perspective to assess the cost-effectiveness of TD in delivering specialist consultations at the RCH for rural and regional patients, compared with standard consultations at the RCH.
Methods
A model-based analysis was conducted to determine the potential costs of implementing teleconsultation at the RCH-DD. Under this model, eligible patients would present to their closest enabled Community Dental Clinic (CDC) for a teleconsultation instead of a face-to-face consultation at the RCH. CDCs were chosen based on classifications used by Dental Health Services Victoria, which divided the state of Victoria into five rural regions. 14 Twelve locations were nominated (i.e., two in each rural region and two additional centers, as a large number of patients were located close to these areas). Patients were assumed to attend the closest CDC location based on their residential postcode.
Decision Model
The model decision tree, which outlines how the source data were sorted to determine the dataset to be analyzed and to determine cost-effectiveness, is illustrated in Figure 1. From the initial dataset, with the approval of the RCH Human Research Ethics Committee, patients who attended the RCH during 2014 for specialist pediatric or orthodontic consultation were sorted into rural/regional and metropolitan groups. Rural and regional areas were defined using the Australia Post postcode classifications.
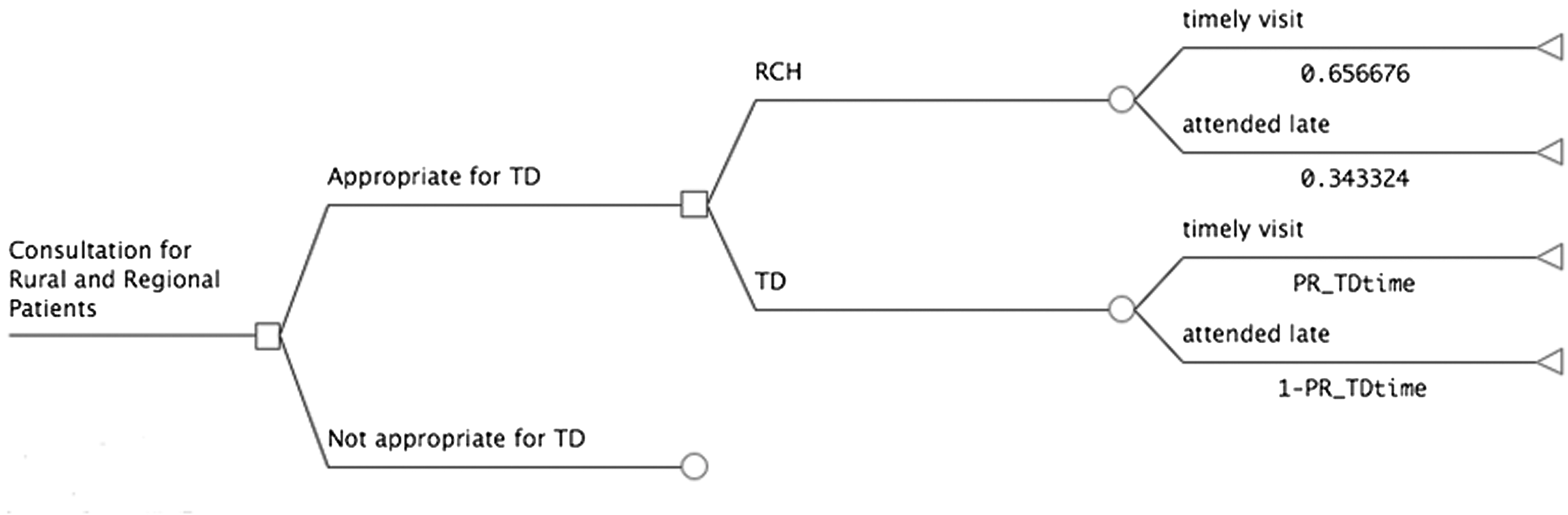
Model to determine Teledental cost-effectiveness. RCH, Royal Children's Hospital; TD, Teledentistry.
TD appropriate consultations were determined according to the following criteria: Presentation to the RCH-DD for orthodontic or pediatric dental consultation. Use of Medicare code for CL&P. Patient lives in a rural or regional area.
In addition to not fulfilling these criteria, the following consultations were not appropriate for TD: Patient's first visit under the cleft scheme. Patient undergoing existing course of care at the RCH-DD. Patient attending a multidisciplinary clinic involving consultations from multiple hospital departments. Patient required consultation and assessment for desensitization due to dental phobia.
Those appointments deemed appropriate for TD were put through two scenarios. The first assumed the patient presented for a face-to-face consultation at the RCH, and a hypothetical consultation time of 75 min was allocated. When a TD consultation was performed instead, a hypothetical consultation time of 60 min was allocated.
An extra 15 min was added to reflect higher likelihood of traffic and greater difficulties in finding parking around the RCH compared with a local CDC.
Measurement of Costs
All costs were valued at 2015 Australian dollar (AUD) prices (1 AUD = 0.75 US dollars) and were valued on a per-appointment basis. No discounting was applied to this 12-month model. A summary of the cost variables is given in Table 1. The costs were separated into three categories:
Summary of Costs
All costs are quoted in Australian dollars (AUD).
DHSV, Dental Health Services Victoria; GDP, General Dental Practitioner; RCH, Royal Children's Hospital; RCH-DD, Royal Children's Hospital Department of Dentistry.
1. Costs to the patient;
2. Costs to the RCH; and
3. Costs to the CDC.
Cost to the patient
To determine direct (travel, accommodation) and indirect (productivity loss) costs for each patient attending a consultation, postcodes were used to calculate the time taken (minutes) and distance traveled (km) to both the RCH and the closest CDC, using Google Maps™ Mapping Service. Patients traveling over 175 km were deemed to require accommodation overnight in Melbourne. A cost of $138.46 per night was determined by the average market rate for the five closest accommodation options around RCH. Transport costs were determined with the cents per kilometer rate taken from the Australian Tax Office for work related car expenses for a small car (65 c/km). 15
The hourly rate for Australian Minimum Wage ($16.67/h) was chosen to value productivity lost using the Human Capital Approach method. 16
Costs to the RCH and Costs to the CDC
Costs borne to the RCH and CDC are similar and will be discussed together.
Wage costs were determined according to the wage award during the TD field study. For specialist services, a sessional rate was used ($150.73/h). 17 For General Dental Practitioners (GDPs) and Dental Nurses, annual pay scales were used, with the GDP Level 2a ($32.59/h) 18 and Dental Nurse Level 2.1 ($22.57/h). 19
Based on dental specialist opinion at the RCH, a 45 min appointment time was allocated to both the RCH and TD groups.
Training of the GDP to conduct a TD consultation involved a trainer visiting each site to brief staff about the operation of the intraoral camera. Based on the time taken to train the staff in the RCH TD field study, it was determined that it would take 2 h. Google Maps® was used to calculate distance and time taken to travel from the RCH-DD to each CDC.
Equipment costs were based on current prices (as of July 2015) for the equipment used in the Field Study (SoproLife® direct USB Camera [Acteon® Group], ClearOne Chat 50 speakerphone [ClearOne], and Logitech HD Pro Webcam C920 [Logitech International S.A]). The annuitized costs for the total technology capital expenditure were done over a 5-year period with a 5% interest rate applied. The cost per use was determined by estimating the expected usage of an intraoral camera (20% of appointments) then calculating the number of appointments in the year (based on 45 min appointments). This allows a single usage cost to be determined and the cost apportioned to each TD appropriate consultation.
Internet and computer utilization, utilities, clinical and office space use, and dental consumables were not included as they are unlikely to have any material effect on the results of this study. Technical support for TD was not included in this study as this was reported as minimal by clinicians who conducted the pilot study.
Outcome Measurements
Timely appointments were chosen as the outcome measurement for this study. According to World Health Organization, this is an intermediate measurement of the responsiveness of a health system. 20 Data regarding the timeliness of each appointment were collected assessing the record of those who under this model would receive a TD consultation. If the patient was seen within 2 months of the suggested recall, the patient was deemed to have received a timely consultation. If the patient did not present within 2 months, it was recorded as a late appointment. If there was no suggested recall, a 1-year recall was assumed.
In the TD model, we assumed that the rate of timely appointments with TD would be higher than in the usual care model. We postulated a higher rate of timely appointments in the TD model due to increased ease of access to a local clinic, thus making it easier to present for a dental consultation in a timely manner.
In addition, the potential clinic time (days) saved at the RCH by introducing TD was calculated using the assumption that each consultation was 45 min long, and the chair is operational for 7.5 h a day.
An Incremental Cost-effectiveness Ratio (ICER) was determined based on the costs per appointment and the number of timely appointments.
Microsoft Excel® and TreeAge Pro® (TreeAge Software, Inc.) were used to calculate costs, determine cost-effectiveness, and perform sensitivity analysis.
A subgroup analysis was conducted to provide a better understanding of how distance traveled would affect cost-effectiveness. Travel distances used in this analysis were: (1) <50 km, (2) 50–80 km, (3) 81–150 km, (4) 151–225 km, and (5) more than 225 km.
To determine the full financial benefits TD can bring that go beyond the cost-effectiveness analysis, the value of extra revenue generated from freed chair time was assessed. The RCH could use the freed chair time to treat more patients, generating additional income for the service. This value was determined by multiplying the number of TD appropriate appointments with the current average per patient from the Child Dental Benefits Scheme (CDBS). The CDBS was introduced in 2014 to assist lower income families to access dental care.
A one-way sensitivity analysis was conducted to test the robustness of our study results, in line with recommendations from previous TD and telemedicine studies.
21,22
The variables considered for sensitivity analysis included the following: • Productivity measurements (Australian Minimum Wage vs. Average Weekly Earnings). • Fixed costs annualized over 1 year, 3 years versus 5 years. • Equipment utilization rate—TD versus general treatment utilization for record keeping and educating patients. • Interest rate for technology costs (3% vs. 5% vs. 7%). • Accommodation utilization—varying the distances required before accommodation is needed.
Results and Materials
There were 1,439 consultations at the RCH under the CL&P Scheme in 2014. Of those, 673 consultations were from rural and regional patients, with a total of 367 (54.5%) appropriate TD appointments. For those consultations, the average distance traveled for consultation at the RCH was 257.4 km per round-trip. The average distance traveled for teleconsultation at the closest CDC was 78.8 km per round-trip. On average, a TD consult would save the patient 2 h and 21 min and they would travel 178.6 km less compared with traveling to a RCH consultation.
The annualized cost of the teledental equipment was $2,383.61 per CDC annualized over a 5-year period at a 5% interest rate.
A total of 74.1 h and 4,488 km would be required for the trainer to travel to each of the 12 locations. The total cost of this initial training would be $9,738.47.
Under conventional care, the expected costs per consultation are $431.29. For TD, the total costs per consultation are $294.35. TD on average would save $136.94 in societal costs per consultation. The largest cost in the RCH model was transport costs ($167.31 per consultation), while the largest single cost in the TD model was for the specialist pediatric dentist ($104.09). The total extra cost to implement a TD consultation at a CDC would be $71.48 per consultation (Table 2).
Total and Average Costs
All costs are quoted in Australian dollars (AUD).
From a societal perspective, TD would save $50,258.92 in total costs per year. Costs to the patient were reduced by 69% in the TD model ($102,897.10–$32,177.74) and made up a significant proportion of the overall cost savings.
Regarding responsiveness of the consultations, 65.7% (241 vs. 126) were considered timely appointments. Those who did not attend on time lived further away from the RCH than those who did attend their appointment on schedule (137.5 km vs 124.1 km). Under TD, it was assumed that the number of timely appointments would be 257 (70%), which corresponds to the next highest tenth percentage value.
The ICER comparing TD and RCH indicates that for every extra timely appointment that is seen with the implementation of TD, there will be a societal cost saving of $3,160.81 ($294.35–$431.29)/(0.7000–0.6567).
The largest difference in cost savings was the costs to the patient (transport, accommodation, and lost productivity costs), a saving of $70,719.19. Costs to the RCH are greater in the traditional model, with the increase attributed to dental nursing costs, while CDCs would need to spend a total of $24,167.66. This is expected as CDC's are not involved in the traditional method of consultation at the RCH.
When looking at the subgroup analysis, the greater the distance a patient resides from the RCH, the greater the cost-effectiveness of a potential TD intervention would be (Table 3). However, if a patient lives within 50 km of the RCH, TD is not as cost effective.
Subgroup Analysis: Distance to Royal Children's Hospital
All costs are quoted in Australian dollars (AUD).
ICER, Incremental Cost-effectiveness ratio.
Overall, a total of 275.3 clinic hours or 36.7 clinic days would be saved under the TD model. This amounts to potentially an extra half-day clinic per week. This time represents the potential dental clinic time freed up at the RCH that could be used to increase the current capacity for service provision at the dental clinic. The potential CDBS revenue from freed chair time from shifting 367 consultations to TD would be $73,400 (367 consultations × $200/per patient). This value gives an indication of the additional benefits that the free chair time could bring to the RCH-DD.
The sensitivity analysis indicates that after adjustment of potential variables, the TD is still the dominant option in all scenarios, compared with the current RCH consultation system (−$3,160.81 vs. −$1,980.04). If the equipments were only used for TD, the cost-effectiveness would be more than halved (−$3,160.81 vs. −$1,454.93), with annualized total equipment costs rising markedly, from $1,751.57 to $28,603.35 (Fig. 2).
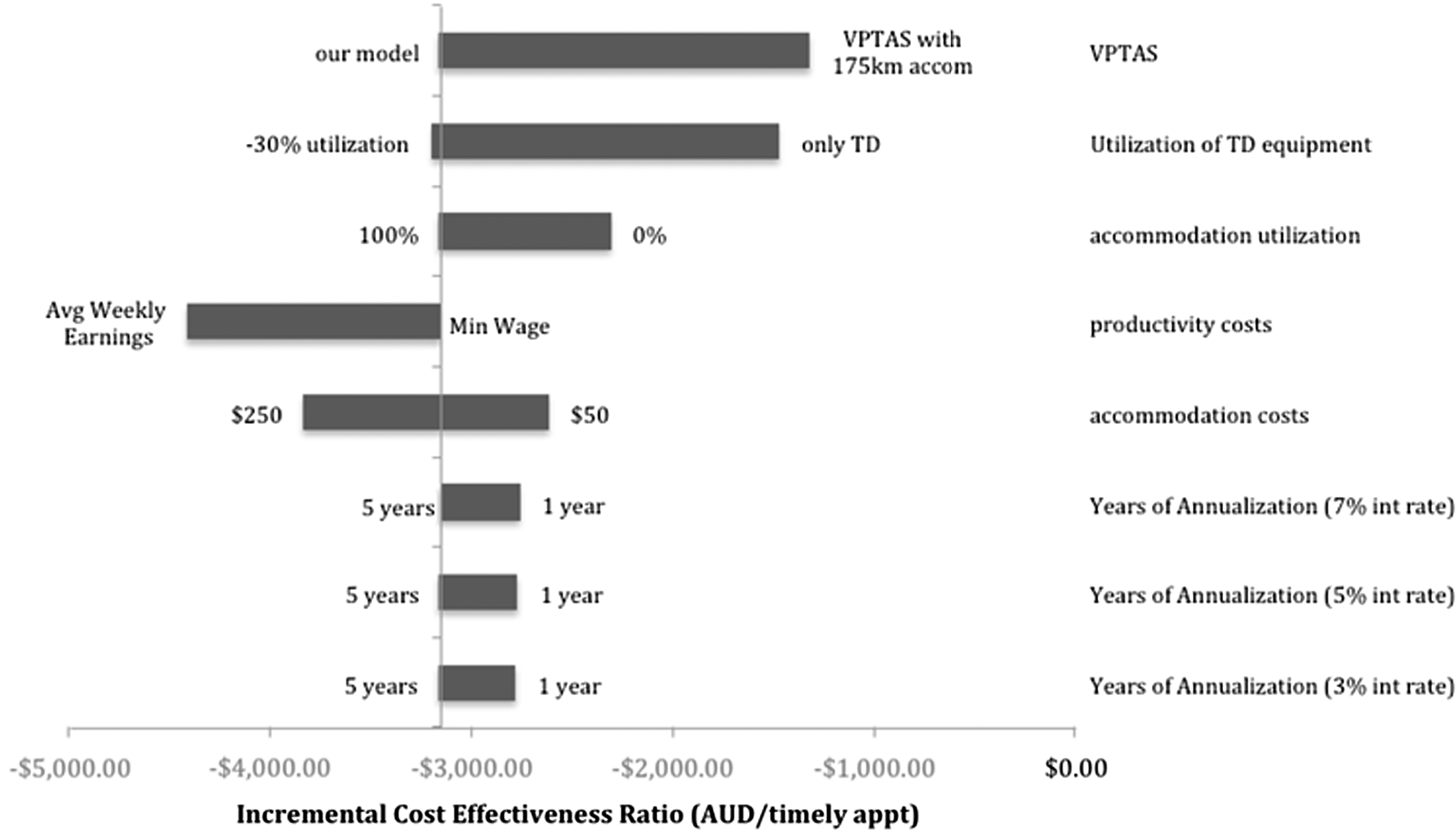
Tornado diagram representing the influence on the Incremental Cost-effectiveness Ratios from a set of one-way sensitivity analyses. All costs are quoted in Australian dollars (AUD). VPTAS, Victorian Patient Transport Assistance Scheme.
Discussion
The present study is one of the few economic evaluations of TD. 4,8,23 TD is a cost-effective option for management of CL&P patients living in rural and remote areas, with an estimated cost saving to society of $3,160.81 for every timely CL&P consultation. These findings support the implementation of TD as a cost-effective option for the delivery of dental services. Travel avoidance has been noted as one of TD's primary benefits 5,24 and this study helps to quantify this benefit. The results are also in line with previous telehealth studies, indicating greater cost-effectiveness, when greater travel distances are required. 13
In the present study, a conservative approach was taken, and some of the assumptions made may underestimate the true costs of attending the RCH for CL&P consultations (e.g., the rate used for productivity lost and transport costs). In addition, while it is difficult to place a figure on the opportunity costs, it is likely that the space in a tertiary institution like the RCH is more valuable than that at regional primary healthcare centers. Despite these conservative assumptions, the TD model still proves the dominant option.
Our findings indicate that distance can be a barrier to accessing specialist CL&P care in a timely manner. As discussed, there are plausible arguments that TD should improve the rate of timely appointments. Thus, the implementation of TD is likely to reduce CL&P patient costs without a large increase in costs to the oral healthcare provider ($10,319.85 per CDC). In addition, an extra $73,400 could be generated by the RCH if the chair time freed by TD was used to see other patients.
Taking a pragmatic approach to the design of this model would imply high internal validity. In contrast, generalizability may be more difficult given this approach. 25 Despite this, our contention is that TD may prove even more cost effective in larger Australian states (e.g., Queensland and Western Australia), where traveling greater distances is often required to access specialist dental services.
Present results must be assessed in view of the limitations in this study. First, this study was based on a model rather than real-life operation of TD; the study assumed that CL&P patients would prefer a TD consult, but the level of acceptance of TD by patients is unknown with some patients or clinicians potentially preferring a face-to-face consultation. Timely appointment rates are one of many possible clinical outcome indicators. Previous TD studies have used inappropriate referral rates and failed appointments as an outcome measurement. 26 Further investigation into how TD could be used to improve inappropriate referral rates could help strengthen the case for TD. Better data collection regarding other outcome measures, such as failed appointment rates, could also assist in providing better information to evaluate TD. In addition, a 1-year time frame was chosen. This restricts the amount of analysis that can be done for this population. Additional investigation and further improvements of the model could help policy makers and researchers in better understanding TD making more informed decisions regarding health service delivery. Specific areas of further research have been highlighted to better test the robustness of our model.
The purpose of the evaluation was to assess the cost-effectiveness, from a societal viewpoint, of the implementation of TD for CL&P patients living in rural and remote areas of Victoria, versus face-to-face consultation at a metropolitan location. While the analysis has inherent limitations due to its dependence on a range of assumptions, TD represents an option that addresses inequality in access to specialized oral healthcare. As such, results provide important information for future economic analysis and may help health program managers to determine the economic and service provision impact of TD, under the conditions prevailing in Australia. Since the analysis indicates consistent cost-savings for society without increasing costs to the oral health providers, the likelihood of economic and human benefits to society is considerable.
Footnotes
Acknowledgments
This study was a collaboration between the University of Melbourne School of Population Health, Melbourne Dental School and the Royal Children's Hospital Dental Department as part of an MPH research project.
Disclosure Statement
The authors have no financial or non-financial relationships to disclose.