
Abstract
Background:
Cannabis use is common among young adults. Web-based interventions are an increasingly popular way to reach this population. The aim of this study was to evaluate the efficacy of a Web-based tailored intervention, developed on theoretical and empirical grounds, to reduce cannabis use among young people by promoting a more positive intention to abstain.
Methods:
An experimental design was employed to evaluate the efficacy of the intervention in reducing cannabis use (primary outcome) by bolstering intention (secondary outcome) to abstain from use. Participants were randomly assigned either to an experimental group that received the Web-based tailored intervention or to a control group that did not.
Results:
Of 588 young adults (18–24 years of age) recruited, 295 were randomly assigned to the experimental group and 293 to the control group. At baseline, 343 reported using cannabis at least once in the past year. An intention-to-treat analysis showed that, at postintervention, a higher proportion of participants in the experimental group had reduced their cannabis use compared with the control group [10.8% vs. 5.1%, χ2(2) = 9.89, p = 0.007]. A mixed model for repeated measures revealed a statistically significant difference in terms of change in intention to abstain from cannabis use in the coming month [Group × Time interaction, F(1,474) = 8.03, p = 0.005]: intention increased for the experimental group (5.07 ± 2.07 to 5.45 ± 1.88; p < 0.001), but stayed stable for the control group (5.32 ± 2.03 to 5.36 ± 1.99; p = 0.779).
Conclusion:
This study shows that the intervention can be efficacious in reducing cannabis use among young people attending adult education centers.
Introduction
Cannabis is the most widely used illicit drug in the world. Teens and young adults are its biggest consumers. According to the Canadian Alcohol and Drug Use Monitoring Survey, 34.8% of Canadians 15–24 years of age reported having used cannabis at least once in their life. 1 Prevalence of use in the past 12 months was much higher in this group than among adults 25 years or older (20.3% vs. 8.4%). In Quebec, a study by Kairouz et al. 2 showed that 53.2% of Quebecers 15–24 years of age had used cannabis more than once in their life and that 38.9% had used it in the 12 months preceding the survey. In a more recent study, conducted with 410 young people attending Quebec adult education centers, more than half of the respondents (52.7%) reported having used cannabis at least once in the past year, more than one-third (39.9%) reported having used cannabis in the past 30 days, and more than one-tenth (13.4%) reported using cannabis every day. 3
It is acknowledged that ∼1 out of 10 cannabis users will develop a dependence to the drug at some point. 4 Even if they are not dependent, some users seek help to reduce their consumption. Unfortunately, there are many access barriers to intervention aimed at reducing substance use: inability to attend face-to-face sessions, poor availability of interventions, cost of therapy, confidentiality, and stigmatization concerns. According to Gulliver et al., 5 the development of online interventions has the potential to circumvent these barriers.
Although the literature on Web-based strategies to reduce cannabis use remains sparse, the few existing studies in the field have yielded promising results. In this regard, Tait et al. 6 conducted a meta-analysis of the effectiveness of Internet and computer-based interventions in reducing cannabis use among adolescents and young adults. The results from the 10 studies they covered showed a small but significant overall effect size (g = 0.16; 95% confidence interval: 0.09–0.22). The majority of these studies focused either on adolescents (n = 5) or on service users with a consumption problem (n = 3).
Against this backdrop and to tap the Internet's potential, we drew on Intervention Mapping (IM) to develop a Web-based tailored intervention for reducing cannabis use among young adult dropouts 18–24 years of age returning to school in adult education centers in Quebec. 7,8 IM is a methodological approach involving six steps for developing health prevention and promotion programs. The strength of the IM protocol lies in the fact that it integrates theory, empirical evidence, and information collected from target populations to design an action plan for intervention. A detailed description of the methodology used to develop the intervention has been published elsewhere. 7 The aim of the present study was to evaluate the efficacy of this intervention.
Methods
Study Design
An experimental design was developed to evaluate the efficacy of the Web-based tailored intervention to reduce cannabis use (primary outcome) by bolstering intention (secondary outcome) to abstain from use. The participants were randomly assigned either to an experimental group that received the intervention or to a control group that did not. The control group completed the measurements only. Cannabis use and intention to abstain were measured at baseline and at 2 months postintervention on brief online self-report scales. A 2-fold hypothesis was posited: at postintervention, a higher proportion of participants in the experimental group would have reduced their cannabis use and the experimental group would have increased their intention to abstain more, compared with those in the control group. The study was approved by the Université Laval Research Ethics Board (2009-116).
Sample and Study Setting
The study population consisted of young adults 18–24 years of age attending adult education centers in Quebec (Canada). To ensure a sample large enough to conduct analyses as planned, we recruited 588 people in 7 different centers. This number was based on an anticipated attrition rate of 20% and on data from Gagnon et al., 3 which showed that 52.7% of young adults had used cannabis at least once in the past year.
To participate in the study, individuals had to meet the following inclusion criteria: 18–24 years of age, enrolled in a regular diploma program, and would be attending the center for the entire data collection period. They were solicited by a youth worker at each center. Students who agreed to participate met with a member of the research team and received an explanatory letter to read and a consent form to sign.
Throughout the process, a youth worker at each center reminded participants when to log in to the intervention. However, since the youth worker was unable to work with a large number of people at the same time, three student cohorts were formed at each center. This made it easier to provide individualized follow-up, thereby limiting the number of withdrawals during the study period. Pseudonyms were used to preserve the anonymity of the participants while retaining the capacity for data matching. The youth worker kept the list of pseudonyms under lock and key to ensure individualized follow-up. Data were collected in the adult education centers from January 2012 to March 2013. Over this period, three cohorts of students enrolled at each center.
Intervention
The Web-based tailored intervention was intended to support young people to reduce cannabis use by strengthening their intention to abstain. The intervention was based on Ajzen's theory of planned behavior because of its capacity to explain the behavior of not to use cannabis in a preliminary study. 3 According to Ajzen, the immediate predictor of behavior is the intention to engage in the behavior. 9 To reduce cannabis use, young people must recognize their vulnerability in situations that put them at risk, make the decision to abstain, and avoid risky situations. The intervention focused on three determinants: (1) attitude, (2) perception of control, and (3) habit (i.e., frequency of use). Accordingly, the intervention was aimed at developing a positive attitude and a sense of control regarding cannabis abstinence. The behavior of high-frequency users (i.e., daily users) may be impulsive and rooted in their habits. Reducing frequency of use could have an impact on their motivation to abstain.
Seven user profiles were generated based on frequency of cannabis use in the past month/year and intention to abstain in the coming month (Fig. 1). These would be targeted by the Web-based tailored intervention.
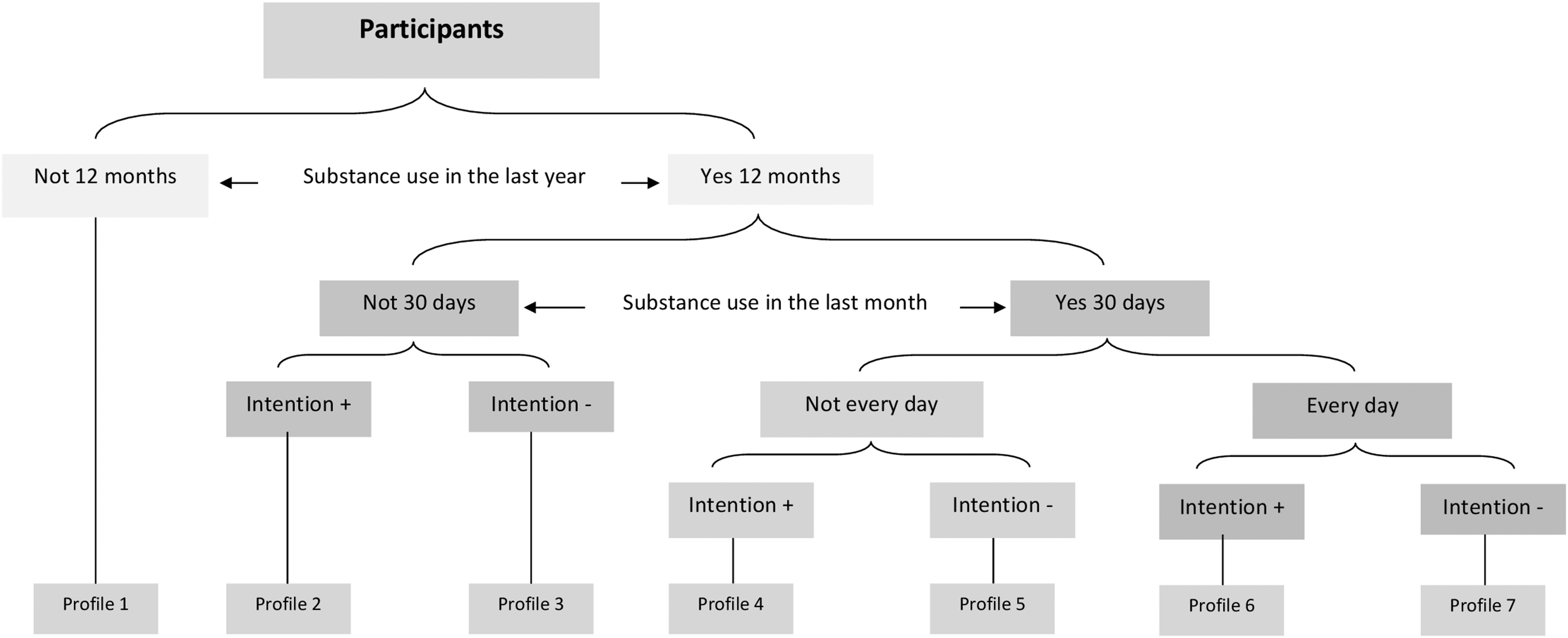
User profiles.
Each profile corresponded to an intervention sequence comprising five brief visits to the Web platform (around 10 min each) at 2-week intervals (Fig. 2). During the first visit (first exposure), participants had to log in with a username and complete a brief questionnaire to assess behavior (cannabis use) and cognitive dimensions (intention, attitude, perception of control). Answers were instantly analyzed by a computer algorithm to establish the user profile (1 of 7). At each visit, an educational message was delivered by a credible character in short video clips. This character resembled a young adult that might have used cannabis and decided to quit. Language, gestures, and posture were chosen to instill a sense of trust and confidence. These educational messages targeted the determinants and were geared to bolstering a positive attitude and a sense of control regarding cannabis abstinence. There were 35 educational messages and up to 16 reinforcement messages, depending on reported past-month cannabis use (Table 1 shows sample messages). At the first visit, once the participant's profile was established, an initial educational message was presented based on the profile. Two weeks later, on the second visit (second exposure), participants entered their username to log in to the Web platform and the intervention continued with a new educational message. On the third visit (third exposure), 1 month after the first, behavior and intention were measured. The algorithm then compared the measurement against the behavior reported on the first visit and delivered a personalized reinforcement message followed by an educational message. On the fourth visit (fourth exposure), 2 weeks later, another educational message was presented. On the fifth and last visit (fifth exposure), a final educational message was delivered and behavior and cognitive dimensions were measured once again. At this point, a final personalized reinforcement message was received. At each visit, a member of the research team was on hand to assist the participants as needed.

Web-based tailored intervention sequence.
Sample Messages at Session 1 for Profiles 1 and 6
Measured Variables
Primary outcome: reduction of cannabis use
The behavioral outcome measured was frequency of cannabis use in the past month. The following question was asked: “How often did you use cannabis in the past month?” Possible answers were on a 4-point scale: never; several times, but not every week; several times a week, but not every day; and every day.
Secondary outcome: intention to abstain from cannabis use
Intention to abstain from cannabis use was measured with three items on a 7-point scale, as recommended by Ajzen. 9 The items were the following: (1) “I intend not to use cannabis in the coming month”; (2) “In the coming month, the chances of my not using cannabis are…?”; and (3) “In the coming month, I will not use cannabis.” For the first item, the possible answers ranged from strongly disagree (+1) to strongly agree (+7). For the second, the scale ran from very low (+1) to very high (+7). For the third, it went from very unlikely (+1) to very likely (+7). 3 Cronbach's alpha for the intention construct was 0.87.
The instruments and measurements for cannabis use and intention to abstain were tested in a prior study of predictors of cannabis use among 260 young adults. 3 Data regarding the sociodemographics of participants, including age and sex, were gathered as well.
Analysis Plan
A chi-square test was used to compare the proportion of lost to follow-up by groups (experimental and control), sex, and frequency of cannabis use. A Student's t test was used to compare average age and intention to abstain of groups of participants by lost to follow-up status.
To examine the intervention's efficacy in increasing intention to abstain and reducing frequency of cannabis use, we analyzed the data using a mixed model for repeated measures and chi-square tests. For the intention-to-treat (ITT) analysis of the frequency of cannabis use, a last-observation-carry-forward strategy was used to impute missing data at 2 months postintervention. To assess the impact of data imputation on results, sensitivity analyses using nonresponder imputation and complete cases only were carried out as well. All analyses were done with SAS software 11 version 9.4 and a significance level of 5% was applied.
Results
Of the 588 young adults recruited in 3 cohorts across 7 adult education centers, 295 were randomly assigned to the experimental group that received the intervention and 293 to the control group that did not (Fig. 3). The percentages of lost to follow-up by groups were 19.7% and 18.4% (p = 0.753) for the experimental and control group, respectively. No significant differences emerged on any of the variables at baseline between completers (n = 476) and noncompleters (n = 112).
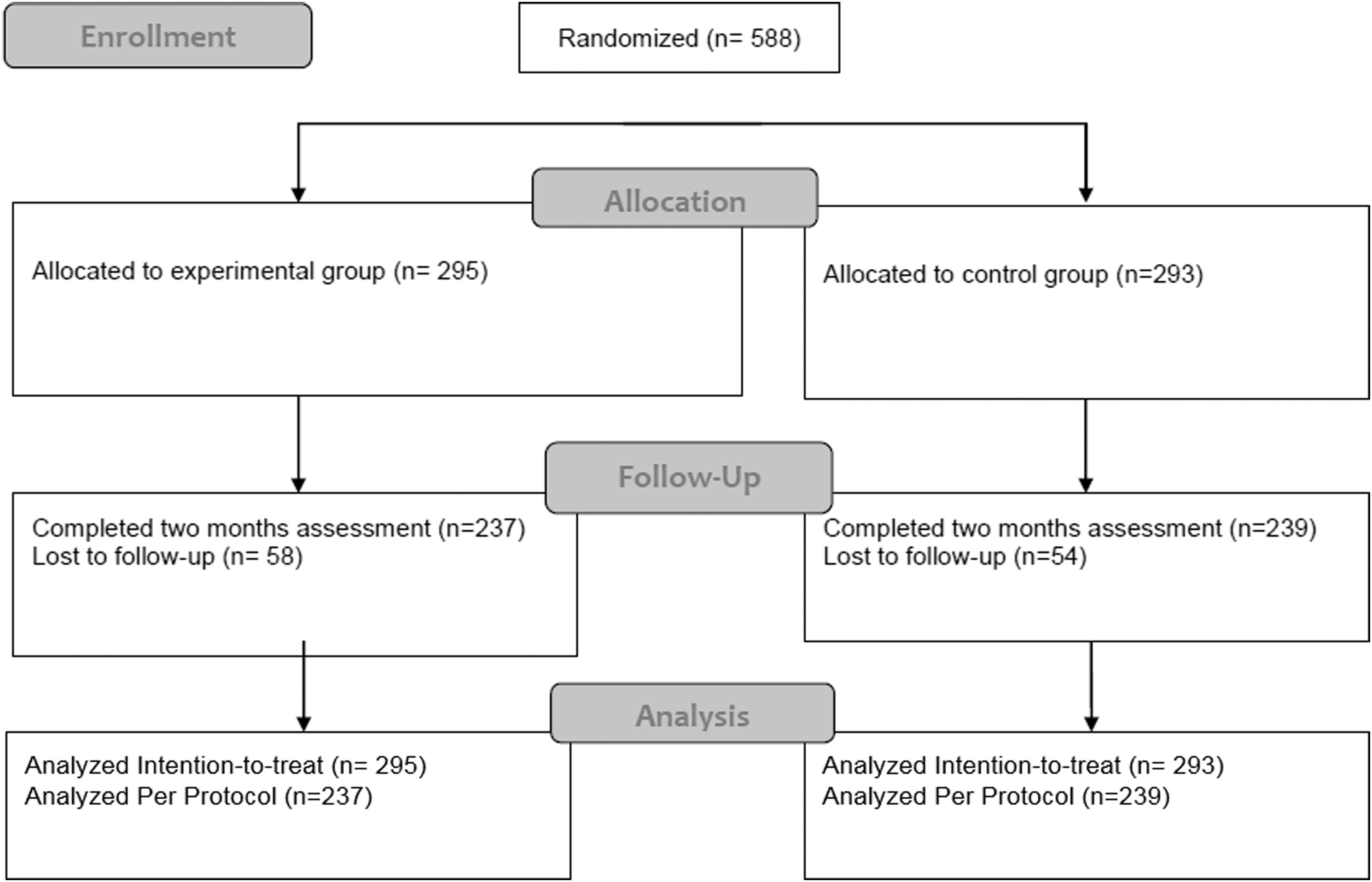
Flowchart of participant.
Sample Characteristics and Descriptive Statistics
The mean age of participants was 19.8 ± 1.9 years; 54.3% were women. At baseline, 58.3% of the participants (n = 343) reported having used cannabis at least once in the past year.
Table 2 gives the percentage of participants that had used cannabis in the past month in the two groups at baseline and at postintervention. At baseline, the proportion of participants who reported having used cannabis was significantly higher for the experimental group compared with the control group [48.5% vs. 38.2%, χ2(1) = 6.29, p = 0.013].
Proportion of Participants Reported Using Cannabis in the Past Month in the Experimental and Control Groups
Effect on Cannabis Use And Intention to Abstain
To test the hypothesis that at postintervention a higher proportion of participants in the experimental group would have reduced their cannabis use, chi-square tests were run using three different missing data management techniques: ITT approach using last observation carried forward; ITT approach using nonresponder imputation; and per-protocol analysis. As shown in Table 3, a higher proportion of participants in the experimental group did reduce their cannabis use.
Analysis of the Evolution of Cannabis Use
CI, confidence interval; ITT, intention-to-treat; LOCF, last observation carried forward; MD, missing data; NRI, nonresponder imputation; PP, per-protocol analysis.
Regarding intention to abstain from cannabis use in the coming month, a mixed model for repeated measures revealed a significant difference in terms of change over time [Group × Time interaction, F(1,474) = 8.03, p = 0.005]. Intention increased for the experimental group (5.07 ± 2.07 to 5.45 ± 1.88; p < 0.001), but stayed stable for the control group (5.32 ± 2.03 to 5.36 ± 1.99; p = 0.779).
Discussion
The Web-based tailored intervention that we developed and implemented, demonstrated its potential to reduce cannabis use and increase intention to abstain among young adults attending adult education centers. These results are similar to those reported by Tossmann et al., 12 who also noted a positive impact following their Web-based intervention program. They, too, observed a greater decrease in cannabis use among young participants who completed a 50-day Web-based intervention program based on the principles of self-regulation and self-control, compared with a control group.
The high baseline intention level in our sample suggests that the participants recruited were already motivated not to use cannabis and wished to reduce their consumption. In this regard, a randomized controlled trial by Rooke et al. 4 demonstrated the effectiveness of a self-guided Web-based cannabis treatment program among 225 individuals who wanted to cease or reduce cannabis use. These researchers concluded that Web-based interventions could be an effective means of treating uncomplicated cannabis use.
A number of elements might have contributed to the impact of the intervention. The IM framework was useful in that it allowed linking knowledge of target communities with theoretical and empirical knowledge. This is a potential success factor in interventions mentioned in the literature. 8,13 The consultations held with young people to validate our methodological choices were a determining factor in the planning process, as was the focus on theoretical application parameters for the methods. As a result of this process of intervention development, the intervention comprised multiple elements of success. Among these, the tailoring strategy allowed personalizing the intervention according to frequency of cannabis use in the past month and intention to abstain. In addition, the educational messages targeted predictors of intention, including positive attitude and perception of control. Lastly, we believe that the use of an actor in the video clips who resembled the targeted group added credibility to the message. In sum, the educational messages and the reinforcement messages, tailoring to behavioral outcomes (frequency of cannabis use in the past month), and the overall online environment (look and feel, visual quality, graphics, videos) were all positive contributors.
The results of this study must be interpreted with caution given the bias introduced by the use of an assessment-only control group. In addition, the participants in the control group were not blinded to their condition assignment. As stated by Higgins et al., 14 when participants and youth workers have knowledge of the allocated intervention in a study, this introduces a performance bias. Moreover, despite the randomization process, the experimental and control groups differed at baseline on the proportion of cannabis users. Other limitations must be taken into account as well. For instance, the use of a self-administered questionnaire and a self-report behavioral measure could have introduced another bias. Studies of health-related behaviors are frequently subject to social desirability and memory biases. Indeed, it can be difficult for study participants to admit to a behavior that is not socially desirable, such as using cannabis, or to remember accurately the frequency of this behavior in the past month or year. However, it should be pointed out that our questionnaire had previously been tested for internal consistency of measured variables and temporal stability.
Notwithstanding these limitations, the Web-based intervention we developed demonstrated the potential to reduce cannabis use among young adults in adult education centers. Our intervention also had an impact on the intention of young adults to abstain from cannabis in the coming month. It is interesting to note that merely acting on their intention can have a potential impact on their cannabis use behavior. Furthermore, although the study did not allow us to compare the efficacy of different intervention methods, we have reason to believe, like Bartholomew et al., 8 who suggested that, attention paid to target behavior determinants, the theoretical foundations of methods, the strategies used in the intervention, and the participation of target group individuals in developing the intervention, all contributed to its success. In sum, this study adds to our knowledge of Web-based strategies that address cannabis use.
Conclusions
In conclusion, our results lend support to the efficacy of our Web-based tailored intervention on cannabis use. We believe that information technology holds tremendous promise for interventions intended to prevent and reduce cannabis use among young people. In the context of our study—adult education centers—interventions delivered online can overcome implementation barriers and offer a number of benefits over traditional school-based prevention programs. 15 In this regard, the systematic review by Lustria et al. 16 supported the notion that Web-delivered interventions made it easier to implement tailored programs across wider populations and thus increased access to the benefits of tailoring in spite of geographical and temporal barriers. Online programs are more feasible for two reasons: They do not require professionals for delivery and teachers typically require little training. 17 In addition, given that Internet interventions consist of preprogrammed content, they can often be implemented with a higher degree of fidelity, as teachers cannot tamper with core program components. 18,19
Footnotes
Acknowledgments
The authors would like to thank all those who participated in this study and, more particularly, the administrators and service providers of the adult education centers. Our thanks also go to the graphic and Web site designers at Akufen. This work was supported by a grant from the Drug Strategy Community Initiatives Fund (DSCIF) of Health Canada (grant No. 6558-05-2009/6190167).
Disclosure Statement
No competing financial interests exist.