
Abstract
Introduction:
E-health software tools have been deployed in managing knee conditions. Reporting of patient and practitioner satisfaction in studies regarding e-health usage is not widely explored. The objective of this review was to identify studies describing patient and practitioner satisfaction with software use concerning knee pain.
Materials and Methods:
A computerized search was undertaken: four electronic databases were searched from January 2007 until January 2017. Keywords were decision dashboard, clinical decision, Web-based resource, evidence support, and knee. Full texts were scanned for effect of size reporting and satisfaction scales from participants and practitioners. Binary regression was run; impact factor and sample size were predictors with indicators for satisfaction and effect size reporting as dependent variables.
Results:
Seventy-seven articles were retrieved; 37 studies were included in final analysis. Ten studies reported patient satisfaction ratings (27.8%): a single study reported both patient and practitioner satisfaction (2.8%). Randomized control trials were the most common design (35%) and knee osteoarthritis the most prevalent condition (38%). Electronic patient-reported outcome measures and Web-based training were the most common interventions. No significant dependency was found within the regression models (p > 0.05).
Discussion and Conclusions:
The proportion of reporting of patient satisfaction was low; practitioner satisfaction was poorly represented. There may be implications for the suitability of administering e-health, a medium for capturing further meta-evidence needs to be established and used as best practice for implicated studies in future. This is the first review of its kind to address patient and practitioner satisfaction with knee e-health.
Introduction
The scope for technology-assisted healthcare is far reaching; there are combinations of software, hardware, and electronic applications across a range of platforms, which come together under the banner of e-health. 1 The growth of Web-based resources and software in healthcare has made major leaps forward since the advent of Web 2.0 with the expectation that traditional methods of accessing and delivering health services will irrevocably change. 2 E-health encompasses technologies such as clinical decision support systems (CDSS), decision dashboards, management systems, feedback systems, telehealth, information, or Web-based resources such as electronic patient-reported outcomes and educational packages. 3 Technology-driven clinical encounters are becoming accepted as a common experience within a healthcare setting but satisfactory patient engagement in the process may be lacking. 4
CDSS have been used to augment primary healthcare since the wider availability of computing technology from the 1970s and, particularly, the impact of desk-top computing in the 1990s. 5 CDSS are computer systems designed to enhance clinical reasoning and can be differentiated as computer-based comprehensive clinical support systems, expert systems, or evidence-adaptive CDSS. 6 They are designed to assist practitioners dealing with individual patients at the time of a clinical encounter by providing dynamic access to epidemiology and expert knowledge data. 7 If used in an appropriate setting, CDSS are proposed to have the potential to change medical education and practice but dependency on currency and quality of information is vital. 8 In the time since Bates et al.'s 9 article on effective clinical decision support, the issues of deploying evidence-based practice in musculoskeletal (MSK) medicine prevail. Bates et al.'s 9 10 technology commandments that include speedy data retrieval, anticipation of needs, real-time delivery, and a natural fit into the mode of practice do not guarantee practitioner compliance with support systems. This may be more heavily influenced by audit requirements, punitive fear of reprisal for eschewing established guidelines, and monetary incentive. 10
Decision aids are used in a variety of conditions and have been seen to improve people's knowledge regarding options, facilitating rationalization around conflicting advice and patients feeling uninformed or confused about their personal values and choices. 11 The effectiveness of evidence delivery systems and benefit to practitioner performance has been established but influence on patient-reported outcome measures (PROMs) is equivocal. 12 It has been determined that software tools assist in a qualified management approach for patients in a number of clinical scenarios with adaptation to shifts in the evidence base. 6
These tools exist to support a range of conditions and healthcare scenarios such as respiratory disease, diabetes, depression, and anxiety. 13 –17 Within any support system, four key attributes should be present: automatic provision of decision support as part of clinician or patient workflow, provision of recommendations rather than just assessments, provision of decision support at the time, and location of decision-making with a computer-based platform. 18 In this framework of structure and conditions, there appears to be a place for physical therapy 19 ; it is not clear how practitioners feel that software tools complement clinical skills and management processes in terms of MSK medicine of the knee. In the light of equivocal evidence that entry level practitioners may not be fully equipped to deal with demands of the knee patient population, engagement with support tools is warranted. 20
The use of software tools in knee MSK medicine is expected to increase alongside delivery of physical therapy through e-measures such as telehealth. 21 A number of Web-based rehabilitation tools are available that effectively provide an inventory of exercises. 22 These provide no reliable indication of the evidence supporting when to use the exercise and how challenging progression should be, especially in an aging population. 23 There may be an abdication of responsibility with such applications but ultimately the practitioners' base knowledge has to provide the concomitant guidance to the patients in deploying these tools. 24 Deployment in the field of MSK rehabilitation has been seen to have some success in return to work, but further studies are needed to explore effective outcomes. 25 The satisfaction with the use of clinical software in the field of knee pain and rehabilitation is not fully understood, and the extent of the impact on the patient has yet to be established. 5,26 Patient satisfaction may be overlooked in the drive to embrace technological change in the clinical encounter. In a recent Cochrane review exploring a range of decision aids, satisfaction was explored in respect of decision outcome; only 17.4% measured satisfaction with the outcome and a single study from the 115 reviewed described higher satisfaction related to the use of the decision instrument itself. 11 The reporting of patient and practitioner satisfaction in published studies regarding e-health for rehabilitation of the knee is not widely explored.
Aims and Objectives
Aim
To review how practitioners and patients satisfaction with the use of software systems in clinical support in knee rehabilitation is reported in relevant studies.
Objective
Systematically identify relevant studies describing patient and practitioner experiences of software use within knee pain and rehabilitation studies to answer the research question: “What is the proportion of studies reporting patient and practitioner satisfaction with software support tools used in the management of knee pain and is this related to sample size, effect size, and journal impact factor?”
Methods
Design: Systematic Review
Procedure
This study comprised a systematic literature search with data extraction and regression analysis.
Systematic literature search
The review investigated quantitative studies exploring user experience of e-health for a range of knee-related conditions. A systematic search for identifying and extracting studies was undertaken by the primary author and reported using a PRISMA flow diagram. Four electronic databases were searched from January 2007 until January 2017 (Cochrane, Medline, Science Direct, and Google Scholar). The keywords were decision dashboard, clinical decision, Web-based resource, evidence support, and knee.
The full search string used was: Search ((((((((decision dashboard) or clinical decision) or Web-based resource) or Internet) or software) and knee))) Filters: published in the last 10 years, humans, English, adult: 19+ years.
Criteria for Selecting Studies
The eligibility criteria were identified through the sample, phenomenon of interest, design, evaluation, research 27 type framework. The sample (S): adult rehabilitation patients: for the purpose of this study, rehabilitation patients are defined as those going through an enabling process that helps them to reach and/or maintain their optimal physical knee function. The phenomena of interest: to be included articles had to have considered the use of software tools with patients undergoing knee pain management or physical rehabilitation. Design (D): all types of designs were used including experimental and cohort designs, reviews and purely qualitative studies were excluded. Evaluation (E): the analysis of rating of satisfaction in relation to e-health measures applied to the knee. Research type (R): quantitative and mixed-method approaches, including randomized control trials (RCTs), nonrandomized, quasi-experimental studies, cohort studies, and single case studies/reports.
Mendeley desktop version 1.17.8 (Mendeley Ltd, London, UK) was used to store and organize retrieved studies. Data were extracted from the articles into a Microsoft Excel version 14 (Microsoft Corporation, Redmond, WA) spreadsheet table. The categories extracted were authors, year of publication, article title, journal, intervention type, design type, population, age (range), sample size, outcome measures, effect size reported, patient satisfaction reported, practitioner satisfaction reported, and journal impact factor. Satisfaction had to be reported with regard to the experience of using the intervention under investigation and not the knee-associated outcome. An independent researcher extracted data from a randomly selected 10% of the main sample of studies that was used for process validation.
Inclusion criteria
Any studies involving knee pain management or knee rehabilitation that employed software technology in the form of decision aids (patient or practitioner), patient compliance monitoring, outcome reporting, progressive goal setting, and exercise management were included. Knee and hip pain studies, where combined populations of sufferers were reported, were also reviewed.
Studies were excluded if interventions focused on purely nonsoftware-based interventions such as advisory, paper-based patient information sheets, verbal educational practice offering guidance only, and technology-assisted surgery. Studies involving technology-assisted interpretation of imaging for clinicians and patient-independent evaluation, purely cost-effectiveness, or epidemiological designs were also excluded.
Theses, protocols, conference proceedings, and nonpeer reviewed articles were excluded because they lacked sufficient quality and detail. Articles not written in the English language were excluded because translation facilities were unavailable and articles were selected from 2007 onward to only include the most recent literature. Samples were limited to adults to allow for autonomous patient engagement rather than experience filtered through a parent, guardian, or carer.
Statistical Analysis
Summary statistics for the study characteristics were calculated using Microsoft Excel. Full texts were scanned for inclusion of effect size reporting and satisfaction scales from participants and practitioners related to the use of the intervention. A binary value of Y or N was recorded and the proportions of these values allowed for dichotomous grouping that was used to determine whether a difference in impact factor score existed between groups that reported satisfaction and those that did not. A binary regression was run with impact factor and sample size allotted as predictors in the model with indicators for satisfaction and effect size reporting as dependent variables. Effect size, sample size, and journal impact factor were selected as indicative of reporting quality. 28 Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated with a significance threshold set at 5%. Analyse-it version 3.76 (Analyse-it Software, Ltd., Leeds, UK) was used to calculate all binary regression statistics.
Results
Seventy-seven studies were retrieved after title and abstract screening from a total of 743 initial returns. After application of inclusion and exclusion criteria, a total of 37 studies were included in the final analysis. The process of exclusion is detailed in Figure 1.
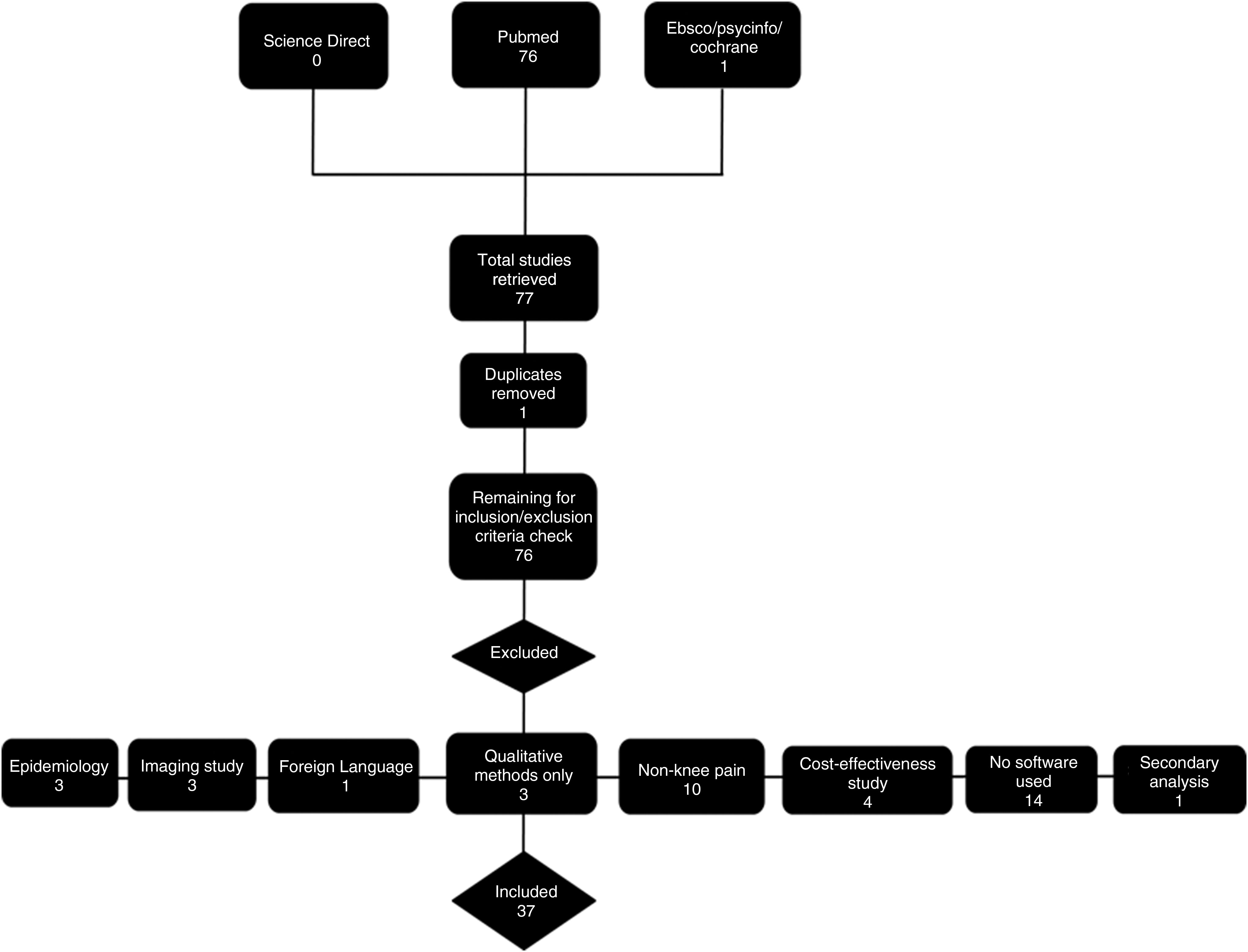
PRISMA flowchart depicting the extraction and selection of study retrieval.
The 37 studies analyzed can be viewed in Table 1 with their related characteristics; a key for the categories of intervention type, design type, and outcome measures can be found in Tables 2 –4. Ten studies reported patient satisfaction ratings (27.8%), whereas only a single study reported both patient and practitioner satisfaction (2.8%). Of the 10 studies reporting patient satisfaction, 2 captured data through a 10 cm analog line, 29,30 2 captured data through a multi-item (17–18) questionnaire of 5-point Likert scales, 31,32 1 reported through a single 7-point scale, 33 1 reported using an ordinal Acceptability Scale with a satisfaction component, 34 3 introduced satisfaction results in the discussion with no prior analytical strategy described, 35 –37 and 1 study reported satisfaction using the Healthcare Satisfaction Questionnaire for patients and a technical quality subjective appreciation questionnaire for practitioners. 38 Independent extraction demonstrated 100% agreement on the presence of reporting on these satisfaction measures.
Study Characteristics and Reporting Indicators
WOMAC, Western Ontario and McMaster Universities Arthritis Index.
Intervention Types with Identifiers
Study Types with Identifiers
Population of Interest with Identifiers
Summary Statistics
The following tables summarize the interventions, design types, and populations under investigation in the reviewed studies.
Electronic PROMs and Web-based training initiatives were the most common intervention investigated. RCTs were the most reported study design and the most common knee populations of interest were knee OA (with and without hip OA) (37.84%). The age range of study participants encompassed 18–96-year olds (mean 59.95 ± 16.71) and an equal representation of gender was seen. The most common knee outcome measures (14% each) were range of motion and the Western Ontario and McMaster Universities Arthritis Index, and the variety of outcome measures can be viewed in Figure 2.

Word cloud representing reported outcome measures.
Regression Analysis
The ORs demonstrate that there was no significant prediction within the models (p > 0.05) with regard to journal impact factor or sample size influencing the reporting of effect size, patient satisfaction, or practitioner satisfaction. Table 5 provides the details of ORs and CIs for the associated models.
Results of Regression Models for Effect Size, Patient, and Practitioner Satisfaction
CI, confidence interval.
Discussion
This study aimed to explore the proportion of studies reporting patient and practitioner satisfaction with software support tools used in the management of knee pain. The proportion of reporting of patient satisfaction was relatively low, with just over a quarter capturing this engagement; the practitioner satisfaction was poorly represented with a single study reporting this item. There was no statistical significance seen with regard to association of reporting satisfaction and effect size, with the size of sample or journal impact factor as indicators of article quality.
Patient satisfaction is generally reported in other areas of healthcare, and with the adoption of e-health initiatives, this is regarded as a key criterion. 66 One proposed benefit of e-health may be the cost saving it makes to the delivery of care, which has been explored with telehealth and particularly remote outpatient scenarios. 67,68 Cost-effectiveness may offset the need for shared patient decision that is also an agenda in clinical engagement, and is reported to lead to improved outcomes and consequently satisfaction. 69 This review excluded studies conducted purely to assess cost-effectiveness, but one single study that includes a cost measure also reported patient satisfaction 37 ; the Web-based resource reportedly saved almost 50% on standard care with moderate-to-high satisfaction levels. 37 The study did not report explicitly how satisfaction ratings were achieved a priori suggesting the lack of attention to this measure.
Practitioner satisfaction may be implicit within the augmented reality of e-health but can be implicated in multidimensional models of practice that can account for variation between clinician and patient experience. 70 Study design may be the influence here, in that single case, validation or cohort studies may be delivered by the developer of the initiative in these reviewed articles. 31,39,41,52,64 This is akin to a pharmaceutical manufacturer not only paying for the research but also administering the drug to the patient, which implicates further bias. 71 The randomized trials within this review fared no better than lower quality designs in terms of reporting, although the single incidence of patient and practitioner satisfaction was an RCT of small sample size in a journal of low impact. 72
Study design may have the additional impact in terms of reporting of effect size and the related sample size. 28 Lower quality evidence will not support suitable statistical power to detect required effect; there may be an assumption that when an effect size is generated, it supports suitability as well as effectiveness of the outcome. 73 Despite recommendations to reliably report effect size in a range of study designs alongside RCTs, 74,75 only a quarter of the 12 trials in this review demonstrated this requirement. 32,48,54 The studies in this review looked to address function and perspective around knee pain and associated conditions and measures. Effect was explored with these outcomes in mind but the suitability of administering the intervention is not evidently reported and patient experience does not inform these effects. Patient satisfaction and treatment acceptance have been qualitatively described as being influenced by shared decision-making with practitioners. 76 Qualitative investigation may elicit the experiential viewpoint more readily than the satisfaction measures reported in this review, 22,77 whereas Rasch analysis may be a more sensitive statistical tool to use with satisfaction scales beyond reporting effect size. 26
Satisfaction is generally high with regard to physical therapy in Western culture 78 and it would be appropriate to contextualize satisfaction data on knee e-health as an ongoing process within MSK medicine. Patient experience has to be taken into account to demonstrate the satisfaction with using the measure itself alongside the measure's outcome: the so-called Fit between Individuals, Task and Technology. 79 The assumption that all technological change is an improvement on healthcare has to be better qualified and supported by meta-evidence of satisfaction. Exploration of satisfaction measures such as the After-Scenario Questionnaire, Post Study System Usability Questionnaire, and the Telehealth Usability Questionnaire 80 should be routinely included in e-health studies into knee-related pain management. The recent proposal of using the standardized Enlight measure 81 to rate e-health interventions is welcome, but further consideration of tempering usability criteria with satisfaction outcomes is warranted. This could facilitate therapists' understanding, critical clinical reasoning, and competencies to readily engage in patient and population-centered healthcare. 82
Limitations within this review are the heterogeneity of the studies in terms of design and intervention. Qualitative synthesis of thematic analysis may allow for a more refined understanding to overcome this, with the advent of sufficient published, experiential material. The reporting standards scrutinized may not have been deemed appropriate or a necessity by all study authors due to the novel interventions involved. The inclusivity adopted was determined by an attempt to define the scope of e-health initiatives within the context of knee pain sufferers; this is the first review of its kind to address patient and practitioner satisfaction in this population. Future studies engaging with the varied forms of e-health in the management of knee-related pain and interventions should look to apply the capture of satisfaction with all interested parties as standard best practice.
Conclusions
Patient and practitioner satisfaction with the use of e-health measures in the management and rehabilitation of knee pain is not routinely reported. This may have implications for the suitability of administering technology in this population; a medium for capturing this meta-evidence needs to be established and used as best practice for studies involving e-health and knee pain in the future. Reporting standards around the use of technology in clinical and domiciliary scenarios should be revisited in light of this review.
Footnotes
Disclosure Statement
No competing financial interests exist.