
Abstract
Background:
Coordination between physicians and allied professionals is essential to the effective delivery of care services and is associated with positive patient outcomes. As information technology can radically transform how professionals collaborate, both researchers and healthcare accreditation bodies are devoting a growing interest to the means of achieving better coordination.
Introduction:
The primary aim of this study is to explain the extent to which and how coordination practices between pathologists, technologists, and surgeons are transformed when telepathology is being implemented.
Materials and Methods:
An interpretive case study was conducted. A total of 60 semistructured interviews with key participants were conducted, in addition to several days of direct observation of telepathology-based intraoperative consultations (IOCs).
Results:
Three major kinds of transformation of coordination practices were observed. First, the telepathology system itself constrains and disrupts coordination routines, such as the presentation of slides. Second, anticipating IOC, proactively performed by the laboratory personnel in traditional settings, requires more formal requests in a telepathology context. Third, local technologists become more autonomous in performing complex macroscopy manipulations and managing the laboratory tasks traditionally performed by pathologists.
Conclusions:
Successful coordination of work in a telepathology-based IOC context requires that significant transformations be anticipated and accounted for. Project managers need to formalize new work processes, support the transformations in professional roles, and mitigate the major hindrances that small material changes may have on work routines.
Introduction
As telemedicine technologies keep maturing, challenges are shifting from technical feasibility to organizational challenges, such as changing workflows 1 and communication issues. 2,3 It is widely recognized that effective coordination between physicians and allied professionals is essential to the effective delivery of care services and is associated with positive patient outcomes. Both academic researchers and healthcare accreditation bodies are devoting attention to the means of achieving better coordination. 4 The coordination of care unfolds in an uncertain and complex environment, where activities and human interactions are more determinant than formal decision-making structures. 5
Although prior research provides us with some insights into how various forms of telemedicine transform the fabric of clinical work in general, 6 –8 there still lacks a clear account of how telemedicine specifically transforms coordination practices. This study attempts to fill this gap. To achieve our main objective, we analyzed the changes in coordination practices as perceived by three occupational groups (pathologists, surgeons, and technologists) during telepathology-based intraoperative consultations (IOCs). Our qualitative study attempts to answer the following research question: To what extent and how does telepathology alter coordination practices in the particular context of IOCs?
The remaining of this article is structured as follows. In the next section, we present the research methods and setting. This is followed by a presentation of the coordination practices used in traditional and telepathology settings at three stages of IOCs. We conclude by discussing the main implications of our work for research and practice as well as its methodological limitations.
Materials and Methods
As already mentioned, the particular kind of telemedicine that was investigated in this study is telepathology. Telepathology research has a long history, and provides advanced insights into the applications, accuracy, and the possible technical configurations of telepathology solutions. 9,10 Telepathology is increasingly being implemented for a variety of applications in cytology and other forms of pathology. 11,12 Beyond the technical and clinical issues that have been the focus of prior investigations, much remains to be discovered about the organizational implications of implementing telepathology in a laboratory. 2 In this article, we focus on a specific usage of telepathology, namely, IOCs, whereby the whole process of extracting, preparing, and diagnosing a specimen is performed during the timeframe of a surgery. Typically, the goal of an IOC is to inform the surgeons whether a cancerous tumor has been fully removed and the surgery can be terminated, or if not, how they should pursue it. An IOC is a highly collaborative process going from planning the surgery and extracting the specimen in the operating room to providing a diagnosis to the surgeon under stringent time constraints. With telepathology, instead of being examined through a microscope, the slide is scanned, and pathologists perform a diagnosis at a distance, using high-resolution computer screens to interpret virtual slides. 13 Telepathology is the only way to perform IOCs when there is no pathologist on site. It involves minimally a surgery team, a technologist in the local laboratory, and a distant pathologist.
The telepathology project under investigation is that of a regional healthcare network located in Quebec, Canada. At the time of the study, it was one of the largest telepathology networks in the world, covering a territory the size of Germany, but inhabited by only 2 million people unequally spread between a dense urban center with a university hospital and barely populated remote regions served by small regional hospitals with or without a pathologist. For these hospitals, IOCs were a key motivation for adopting and using telepathology. 14
A total of 48 pathologists and 17 sites are included in the project. Although 33 of the 48 pathologists are located at the university hospital, the project has no central site responsible for providing pathology expertise throughout the network. Table 1 provides a summary of the nine hospitals where data were collected. The technology was gradually deployed across the network in early 2011, and between January 2011 and March 2015, 1,843 slides were scanned for IOC purposes.
Profile of the 12 Hospitals Visited
IOC, intraoperative consultation.
Data collection for this research project took place during 12 site visits between 2012 and 2015. A total of 60 semistructured interviews were conducted with 51 respondents located in 14 sites. During these interviews, our main goal was to compare traditional versus telepathology-based coordination practices, as all respondents had experienced both forms of IOC (Appendix). The sampling strategy was a mix of snowball and maximum variation, 15 and interviews were conducted until theoretical saturation was reached. 16 Furthermore, researchers spent several days in hospital laboratories, observing clinicians and technologists coordinate during IOCs.
All interviews were tape-recorded, with additional notes being taken when necessary. The average length of each interview was ∼45 min, producing more than 44 h of interviews. We used a conventional approach to content analysis in this study. This type of design is recommended when existing theory or literature on a phenomenon is limited. 17 By gaining direct information from participants without imposing preconceived categories or theoretical perspectives, 17 knowledge is generated based on participants' unique perspectives and grounded in the actual data. We thus immersed ourselves in the data to identify coordination practices and allow new insights to emerge.
Results
In this section, we describe how telepathology has materially transformed the laboratory environment and then, in line with our initial research question, we explain and illustrate how various coordination practices were transformed after the introduction of telepathology.
The Material Transformation of the Laboratory Environment
Telepathology introduces substantial material changes to the laboratory environment. In the pathologist's office, a high-definition screen dedicated to videoconference is installed. In the laboratory, space is cleared to accommodate three new devices: a macroscopy workstation, a scanner, and its associated computer station. The macroscopy workstation allows technologists to describe and manipulate large specimens before preparing the slides under videoconference-based supervision by distant pathologists (Fig. 1). Local laboratory technologists are, for their part, responsible for keeping the telepathology material operational.

A telemacroscopy station.
The laboratory environment revolves around the manipulation of physical artifacts: specimens, tools to manipulate them, and chemical components to alter their properties. It is deemed “contaminated” by its contact with biological specimens. The slide itself is produced by physical manipulations in the laboratory, but it is “fixed”: it has lost its contaminating property, so that the scanner can be installed inside the laboratory or in any room nearby.
In traditional settings, the pathologist's office is typically across the hall from the laboratory where technologists work. Pathologists and technologists work in close collaboration and communication is frequent. The pathologist office is uncontaminated and dominated by two contrasting devices: a computer and a microscope. The microscope is used to interpret the slides, as it remains faster to operate for local routine slides. 2 The computer is used for other tasks, such as updating patient records.
Digital slides can be accessed instantaneously from any authorized screen in the network, by multiple people at the same time, and they do not degrade over time. This enhances the contrast between the technologist's physical manipulations in the laboratory and the pathologist's symbolic work of interpreting images.
The Transformation of Coordination Practices During IOCs
An IOC usually involves four main steps, namely, planning the examination, manipulating the specimen, preparing the slides, as well as performing the diagnosis and communicating it to the surgeon (Table 2). In this section, we describe and illustrate how telepathology has transformed coordination practices at each step of the IOC. Figure 2 summarizes this process.

Microscope-based IOC process. IOC, intraoperative consultation.
Coordination Practices in Traditional Versus Telepathology-Based Intraoperative Consultations
Coordination in traditional settings
The first step consists of planning the IOC. In traditional settings, planning is generally performed in the laboratory as IOC requests can generally be deduced from operating room schedules. For instance, if the schedule contains a lobectomy, the surgeon will likely require an IOC. Surgeons fill surgery requests to book operating rooms but not IOC. The operating room schedule is accessed and interpreted by technologists or laboratory secretaries (Coordination Practice A in Table 2) who infer IOC cases and plan further action without confirmation from the surgery team.
The day before, we receive the operating schedule. It is the list of all the surgeries planned for the day after, with the name of all patients, and the surgeons who will perform them. According to the type of surgeries to be performed, we can determine which ones will require an IOC. A technologist.
Surgeons may phone the laboratory to warn staff, but generally they do not need to formally request pathology support. In simple cases, technologists may not even inform the pathologists, who receive the slides in their office, ready to be read, without prior notice. On the day of the surgery, an operating room nurse signals the start of the surgery (C). Typically, the operating room nurse phones the laboratory. This is done well before the surgeon extracts a specimen and has it transferred to the laboratory.
Simple specimens (e.g., brain specimens) can be manipulated by technologists without any supervision, before handing the slides to the pathologist. In contrast, complex specimens (e.g., large specimens such as intestine sections) need to be handled, oriented, and colored to produce blocks of tissue, a process called macroscopy. The technologist receiving the specimen determines whether an expert intervention (D) by a pathologist is required for the macroscopy. If that is the case, then the technologist stages the specimen on a macroscopy workstation, and calls the pathologist, who comes to the laboratory, manipulates, orients, and describes the specimen, sometimes clarifying doubts over the phone with the surgeon.
Once a glass slide is prepared, it is ready to be examined by the pathologist through a microscope. IOC slides are part of the continuous daily load of routine slides coming from the laboratory to the pathologist office. Pathologists sometimes remain in the laboratory, in which case the technologist directly hands the slides. But in general, the pathologists are in their office, and physical slides (IOC and routine cases) are carried to the pathologist by the technologist. To make this transfer clearer, less time consuming, and less disruptive, technologists organize batches of slides, for multiple patients, into folders (F). Technologists and pathologists have organized over time those folders to coordinate their work. All the slides from a patient are gathered on the same page, and within a page, slides are ordered in the logical order in which they should be viewed, such as the area they were extracted from. Color stickers on the folder edge denote the nature of the cases or their urgency. Technologists generally hand the folders over to pathologists following a routine schedule.
We used to carry the (IOC slides) to (the pathologist) office. He was at his desk doing microscopy and other routine daily cases. We brought the slides and told him: ‘This is your IOC.’ Therefore, he dropped his business and started immediately (working on the IOC) and communicated directly with the operating room to provide the results. A technologist.
Pathologists then examine the slides using a microscope (H). Then, they produce a diagnosis and communicate it by phone to the surgeon waiting in the operating room (J). A direct verbal exchange with the surgeon (or exceptionally a resident) is critical (J), as even nurses present in the operating room cannot relay the diagnosis. The surgeon may then make an informed decision regarding the surgery or request additional IOC.
Coordination in telepathology-based settings
Telepathology-based IOC coordination is significantly different at each stage of the process. Figure 3 represents the process. At the planning stage, surgeons must actively request an IOC. They must make a formal IOC service request at least 1 day in advance (B).
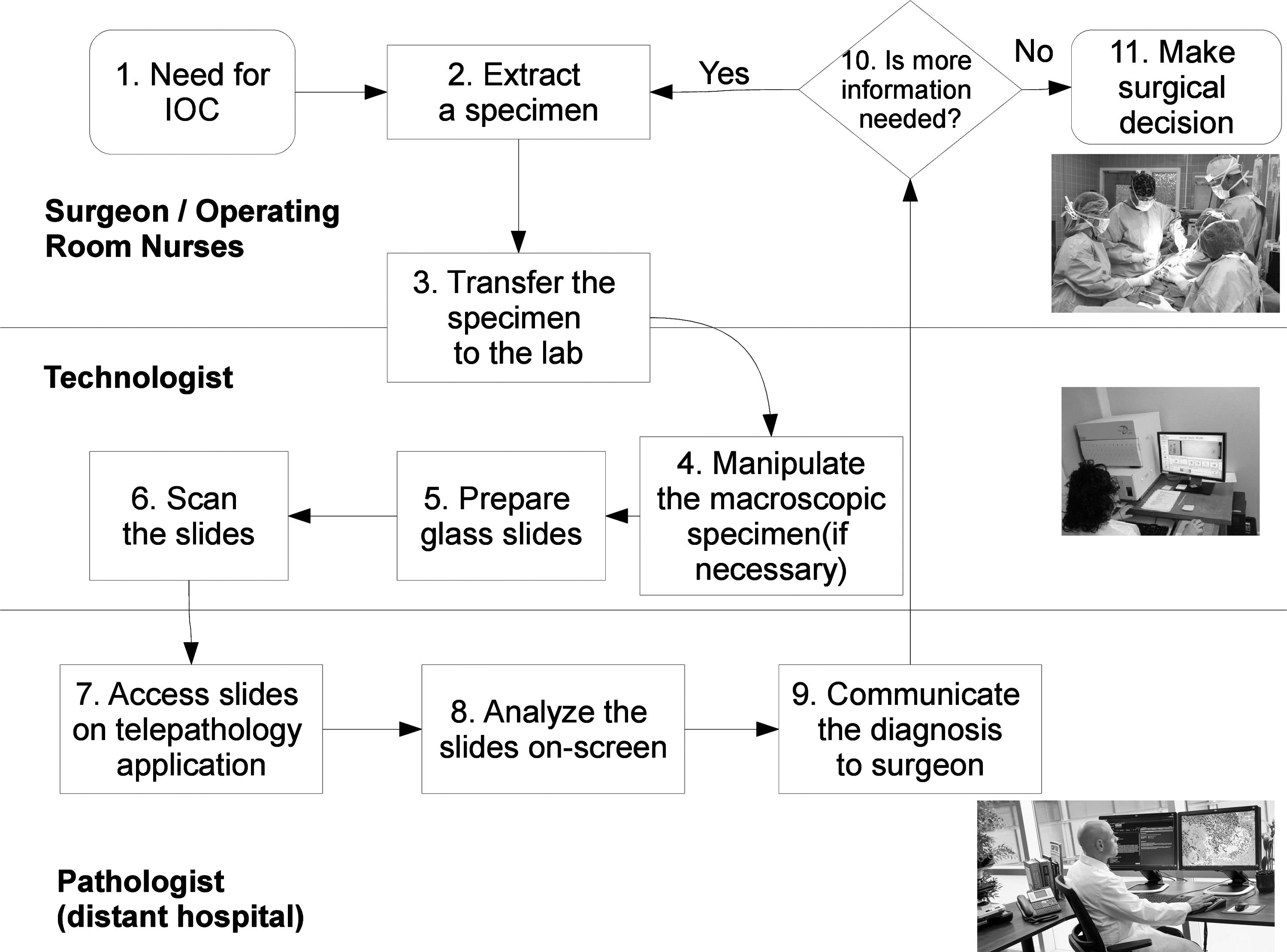
Telepathology-based IOC process.
We ask (the surgeons), as part of our clinical protocols, to indicate the cases for which they believe they will need an IOC. The on-duty pathologist receives the list of IOC cases the day before to be able to plan his work. A pathologist.
At the macroscopy stage, the pathologist uses the telepathology system to support technologists while performing macroscopy. They view the specimen, talk to the technologist handling it, and can even draw indications over a specimen image (E). Still, the system has its constraints: a local technologist needs to physically handle the specimen and the pathologists are unable to palpate the specimen, which is sometimes necessary to identify a cancerous node. As one pathologist puts it, “technologists become our hands.”
The physical absence of the pathologist creates an ambiguity as to who should physically manipulate complex cases. Technologists are expected to perform macroscopy, with surgeon supervision for complex macroscopy cases. But technologists are already present in the laboratory, are more available than surgeons busy in the operating room, have experience with macroscopy in general, and are familiar with the pathologists. This leads them to take an extended role in macroscopy under distant pathologist supervision.
After the glass slides are prepared, technologists take them to the scanner room, log into the system, load the slides into the scanner, scan them, check the image quality, and upload the digital slides to the pathologists. The system then notifies the pathologist that digital slides are available. (G). Next, the pathologists must log into the telepathology system and select the case and the slides before consulting them. The case priority is managed either by the technologist tagging a slide “urgent” in the system or by phoning the pathologists to inform them of the online availability of the slides (C). Alternatively, the pathologist may keep an open phone line with the laboratory, simply muting their own microphone after macroscopy is over, to be aware of when the slide is ready.
The telepathology system automatically attaches the metadata (the information about the slide, such as patient name, time of collection, slide nature, or priority) to the digital slide. Pathologists click on an incoming case and view the digital slides displayed in the order dictated by the application, leading to an extra task of sorting them for viewing after the diagnosis (I).
When I receive glass slides, they are already sorted. The slides go from A to A1, B1 to B20, etc. and I look at them in order, I have the sequence of the examined case. When I receive (complex cases) by telepathology, often, they are not in order and I can't rearrange the pictures. A pathologist.
The final phone call to the operating room to communicate the diagnosis is like traditional contexts practices.
Discussion
Our findings suggest three major changes in how coordination practices are performed when using telepathology-based IOC. First, the tightly knit connection between pathologists, surgeons, and technologists working in the same hospital is not easily replicated at a distance. Whereas in traditional settings, pathologists and technologists monitor the operating room activity to anticipate IOC needs, in telepathology settings, formal requests need to be made in advance, even though technologists are locally present and familiar with the surgeons' practices. This finding suggests that the accountability for distant cases cannot be taken for granted. Healthcare managers must acknowledge the role of proximity in accountability, and the cultural and organizational barriers to moving to another model should not be underestimated.
Second, coordination between technologists and pathologists is also significantly transformed after the introduction of telepathology. Indeed, in traditional settings, technologists work under the close supervision of pathologists, who both trust and control them. When pathologists and technologists work at a distance, pathologists operate at arm's length, and technologists work more autonomously, including on some manipulation tasks traditionally the preserve of pathologists. This requires standardization of work practices and protocols across sites, additional technologist training, and a redefinition of the boundaries of the technologist's profession. These observations suggest that successful telepathology-based coordination is less about enabling proximity through elaborated communication systems than about managing the interdependence aspects of coordination, and more specifically building functional relationships between stakeholders, notably through the establishment of agreed-upon roles and work practices.
Third, the impact of the material constraints of telepathology on coordination should not be underestimated. Although communication technologies such as videoconference or email enable seamless distance communication, telepathology still constrains the interface through which digital slides are shared with pathologists, which may conflict or disrupt the familiar routines of slide folders sharing, or the manipulations of slides that pathologists need to ask technologists to perform. This finding suggests that existing routines should be given proper attention before implementation. They may not be transferable to a telemedicine context, but adjustments should target the key routines impaired in a telemedicine context.
These findings may be transferable to other kinds of telemedicine contexts involving coordination between distant healthcare institutions, such as teleradiology. It is also important to acknowledge some limitations to our study. These findings have been observed in the particular context of the Canadian public healthcare system, and the transformations need to be confirmed in contexts wherein the relationships between healthcare institutions are of a different nature, such as in the American healthcare system. Furthermore, the transformations we observed are highly contextual. They shall not be construed as deterministic consequences of the introduction of telepathology, but rather as emerging patterns.
Conclusions
To achieve the tremendous potential of telepathology, pathologists, technologists, and surgeons must adjust the way they coordinate their work, especially in time-pressed activities such as IOCs. Coordinating pathology work at a distance is not simply doing the same work using communication technologies. As shown in this study, telepathology requires a different set of coordination practices that need to be anticipated and properly implemented to ensure a successful deployment. More research is needed to validate our key findings and determine whether they can be generalized to other forms of telemedicine.
Footnotes
Acknowledgments
The authors would like to thank all the clinicians who participated in this study, in particular Dr. Bernard Têtu, clinical director of the telepathology project, for his invaluable insights. This study was financially supported by Canada Health Infoway (Grant No. 2069-002). The views expressed in this article are those of the authors' and not those of Canada Health Infoway
Disclosure Statement
No competing financial interests exist.