
Abstract
Introduction:
Extracorporeal membrane oxygenation (ECMO) is an invaluable rescue technique for critically ill children with imminent or present cardiopulmonary collapse. However, medical team expertise to optimize results and decrease complications is scarce. Telemedicine can be used to enhance the delivery of quality interventions.
Materials and Methods:
This is a retrospective review of pediatric patients assisted with ECMO in the cardiac intensive care unit (CICU) at Fundación Cardiovascular de Colombia from July 2011 to June 2015 (telemedicine) compared with similar patients from a previous period (pretelemedicine). Collected information included demographic data, cardiac diagnosis, risk adjustment for congenital heart surgery (RACHS-1), hospital mortality, CICU and hospital length of stay (LOS), ECMO type, and ECMO run hours as well as specific telemedicine information.
Results:
Fifty-seven patients in the pretelemedicine and 109 in the telemedicine periods were included in the analysis. Forty-nine teleconsulted patients received 218 teleconsultations, with a recommendation for diagnostic or interventional catheterization in 38 patients (77.5%). A surgical procedure for significant residual lesions was recommended in 30 patients (61.2%). Patients in the telemedicine period were older (4.7 months vs. 1.6 months, p = 0.006), more likely to receive operating room ECMO (43.1% vs. 24.6%, p = 0.02), and had a higher proportion of patients with two-ventricle physiology (73.4% vs. 54.4%, p = 0.013). Hospital survival was higher during the telemedicine period (54.1% vs. 29.8%, p = 0.002), with a longer hospital LOS (67 days vs. 28 days, p < 0.001).
Conclusion:
The implementation of telemedicine-assisted interventions in a pediatric ECMO program delivered valuable diagnostic and therapeutic advice, was associated with significant changes in selection criteria and model of care, and an increased hospital survival.
Introduction
Mechanical cardiopulmonary support with extracorporeal membrane oxygenation (ECMO) is an invaluable tool during medical care of critically ill children with imminent or present cardiopulmonary collapse due to systemic, pulmonary, or cardiac disease. 1 –3 Historically, hospital survival for pediatric patients treated with ECMO has shown a significant improvement, 4,5 but significant expertise is needed to maximize results and decrease complications. 6,7 Furthermore, associated financial costs remain substantial. 8
Many hospitals in developing countries have an unmet need to develop their own ECMO programs and increase their level of proficiency. Indeed, a very small proportion of worldwide-reported ECMO runs come from developing countries. In Latin America, there has been a sharp increase in reported centers providing ECMO within the region in the past 10 years. 9 However, they face challenges in advancing such programs due to an overall scarcity of specialized physicians and ECMO teams as well as their relative lack of financial resources, notwithstanding efforts to simplify ECMO circuits, as well as their process of care and surveillance. 10,11 As has been reported before, the ECMO program at Fundación Cardiovascular de Colombia (FCV) shared similar problems. First of all, the restrictions to hire specialized nursing and the high patients/nurse ratio. Second, the limited availability of ECMO equipment and disposables and the necessity to reduce the cost of the circuit, among others. Hence, novel approaches are needed to leverage scarcely available expertise and optimize outcomes in such programs.
Telemedicine has demonstrated to be an excellent tool to deliver a wide array of health-related services, and may enable a faster improvement in the performance of remote ECMO teams with the resultant reduction of costs for patients, their families, and health system as a whole. 12,13 In this line of thought, during the past decade there has been a steady increase in published reports in the critical care environment, showing a decrease in mortality and better quality of life for adult patients associated with the systematic implementation of telemedicine interventions in the intensive care unit (Tele-ICU). 14 We have previously reported our initial experience with Telemedicine-assisted Pediatric Cardiac Critical Care in the international setting, and specifically our telemedicine work with FCV where we observed a significant decrease in cardiac intensive care unit (CICU) and hospital length of stay (LOS) for cardiovascular patients during the first 10 months of our program inception. 15 –17 We present here our experience with multiple interventions to improve outcomes in the ECMO program at FCV, including those assisted with telemedicine. To our knowledge, this is the first reported experience of the systematic use of telemedicine in an international pediatric ECMO program.
Materials and Methods
On-Site Interventions at FCV
A detailed description of the ECMO program at FCV has been previously published. 10 Critical care and cardiothoracic surgery staff from FCV attended the extracorporeal life support organization course. There were reciprocal visits to each hospital from physicians and ECMO specialists, including an on-site audit conducted by a Children's Hospital of Pittsburgh (CHP) physician in August, 2012. After analysis and recommendations were provided, a structural reorganization was done to the ECMO program at FCV, including the appointment of a medical director, the workflow system of nursing staff and ECMO specialists, and model of care. Finally, a cardiovascular surgeon trained in congenital heart surgery and ECMO at CHP was incorporated to the FCV team in August 2013.
Telemedicine-Assisted Interventions
A description of the initial setup of our telemedicine program has been previously published. 15 In brief, Tele-ICU physicians from CHP performed daily physician-to-physician teleconsultations at the request of the FCV team, with a review of diagnostic approach and perioperative treatment, telementoring (real-time echocardiography, bedside electrophysiology, mechanical ventilatory support, pharmacological therapy, or ECMO weaning/adjustments). A systematic approach was followed during teleconsultations, focusing in the following: (1) an earlier cannulation criteria to avoid cardiopulmonary collapse and organ failure; (2) technical aspects of ECMO including circuit problems, the adequacy of systemic/pulmonary support and anticoagulation; (3) an aggressive diagnostic strategy including cardiac catheterization and angiography whenever needed; (4) as early as possible decannulation based on those mentioned, including necessary medical, surgical, or interventional therapy needed before decannulation; (5) a consensus was sought between the Tele-ICU and FCV teams for a comprehensive diagnosis of cardiovascular and multisystem problems as well as an exit strategy; and (6) finally, a conflict resolution procedure (so-called red-phone solution) was installed to ensure appropriate decision-making whenever significant discrepant opinions remained unresolved at the end of teleconsultations, at the discretion of the teleconsulting physician. Namely, further discussion was prompted between higher hierarchy physicians from both institutions, with the medical team at FCV having a final say. A core curriculum with 64 h of lectures was provided by CHP staff to the CICU nursing staff at FCV (tele-education). In the past 2 years, we included a more proactive approach, with daily virtual rounds, including access to patient remote monitoring, room cameras, electronic medical records, and imaging studies. Patients on ECMO or with a high risk for cannulation were identified, remotely reviewed in advance, and discussed during teleconsultations with the FCV team in the same manner.
Patient Selection
This was a retrospective preintervention and postintervention study. After approval by the institutional review boards of both institutions, we reviewed clinical (FCV) and telemedicine (CHP) databases for pediatric patients admitted to the CICU at FCV and cannulated on ECMO between January 1, 2007, and December 31, 2010 (pretelemedicine period), as well as those from July 1, 2011, to June 30, 2015 (telemedicine period). We excluded patients between January 1, 2011, and June 30, 2011, as this was a “transition period” while starting-up the telemedicine program with some patients being informally teleconsulted during numerous technical tests between the two hospitals.
Missing information was retrieved from the respective patient electronic medical record. Data transfer between the two institutions was performed through secure encrypted messaging, and coinvestigators at CHP merged the clinical and telemedicine databases. Primary outcome was hospital survival with CICU and hospital LOS as secondary outcomes.
Data Collection
Collected data included descriptive demographics, cardiac diagnosis, diagnostic category, hospital mortality, CICU and hospital LOS, ECMO type, and ECMO run hours. Specific telemedicine information included number of teleconsultations, activities during teleconsultations, and provided recommendations. Diagnostic categories included myocarditis/cardiomyopathy, congenital heart disease, and miscellaneous. Surgical procedures were classified by risk adjustment for congenital heart surgery (RACHS-1). This classification allows for discrimination in mortality risk per surgical complexity, with 1 being the group with the lowest and 6 the one with the highest anticipated mortality. 18 Cardiovascular physiology was classified as univentricular (with only one functional ventricular chamber supporting both pulmonary and systemic circulation) versus two-ventricle physiology (namely hearts with two functional ventricles and in-series, separated pulmonary and systemic circulation). ECMO type was classified as indication for failure to separate from cardiopulmonary bypass in the operating room (OR-ECMO), ECMO cannulation during refractory cardiopulmonary resuscitation (e-CPR), and ECMO cannulation due to low cardiac output syndrome (LCOS-ECMO).
Statistical Methods
Continuous variables are summarized as median (range), categorical variables are summarized as n (%). Differences between groups are tested using Wilcoxon–Mann–Whitney tests for continuous variables and chi-squared tests for categorical variables (or Fisher's exact tests for small cell sizes). All statistical analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC).
Results
During the study period, 170 patients in total were placed on ECMO. Four patients had also been placed under ventricular-assist device and, therefore, were excluded, leaving a total of 166 patients included for analysis, 57 in the pretelemedicine period, and 109 in the telemedicine period. All 57 patients in the pretelemedicine period were cardiovascular cases, with 101 (92.7%) in the telemedicine period (p = 0.032). Patients with two-ventricle physiology made up a larger portion of the study group in the telemedicine period (73.4%) than in the pretelemedicine period (54.4%) (Fig. 1). ECMO type distribution was different between study periods (p = 0.020). Specifically, patients in the telemedicine period were more likely to receive OR-ECMO (43.1% vs. 24.6%) (Fig. 2) and less likely to receive e-CPR (11.9% vs. 24.6%). Patients were older during the telemedicine period (4.7 months vs. 1.6 months, p = 0.006), but there were no significant differences in weight or length. Patients during the telemedicine period did tend to have longer ECMO runs (120 h vs. 81 h, p = 0.042). There were no significant differences in RACHS-1 distribution between study periods. LOS in the CICU (41 days vs. 20 days, p < 0.001) and in the hospital (67 days vs. 28 days, p < 0.001) was significantly longer in the telemedicine study period. A summary of relevant descriptive patient information is presented in Table 1.
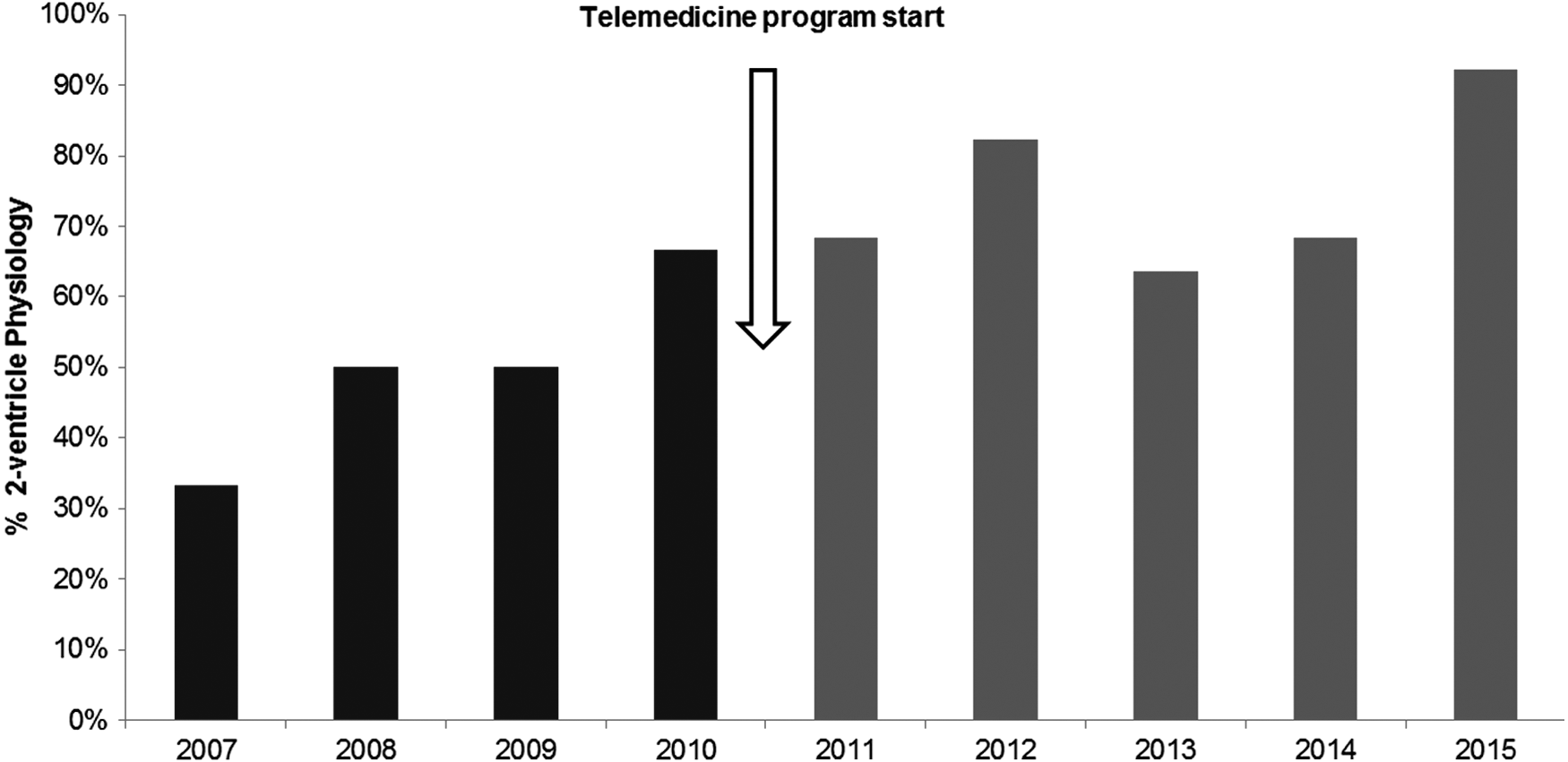
Cannulated patients with two-ventricle physiology, by year.
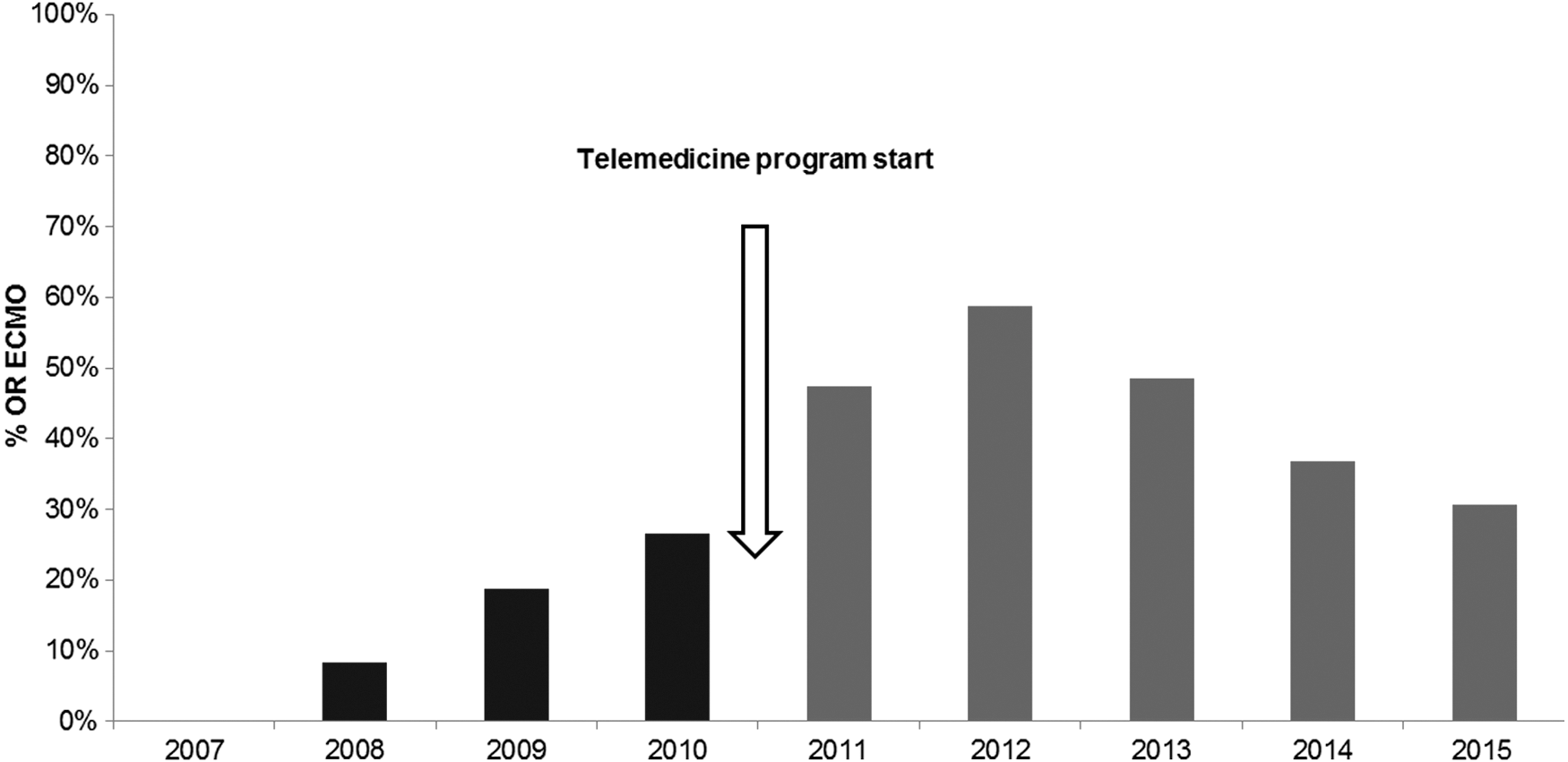
Patients cannulated in the OR-ECMO, by year. OR-ECMO, operating room-extracorporeal membrane oxygenation.
Descriptive Characteristics of Study Population
Fisher's exact test.
Chi-squared test.
Wilcoxon–Mann–Whitney test.
CICU, cardiac intensive care unit; DCM, dilated cardiomyopathy; ECMO, extracorporeal membrane oxygenation; e-CPR, ECMO cannulation during refractory cardiopulmonary resuscitation; LCOS ECMO, cannulation due to low cardiac output syndrome; OR-ECMO, cannulation in the operating room; LOS, length of stay; RACHS-1, risk adjustment for congenital heart surgery.
Hospital survival was significantly improved in the telemedicine period (54.1% vs. 29.8%, p = 0.002) (Fig. 3). When compared within the different RACHS-1 categories, there was a trend that did not reach significance for improved survival in the telemedicine period among all strata, except for patients in category 2 (Table 2). When stratifying by cardiovascular physiology, survival was improved in the telemedicine era versus pretelemedicine in both single-ventricle physiology (31% vs. 11.5%, p = 0.081) and two-ventricle physiology (62.5% vs. 45.2%, p = 0.097), although values did not reach significance. Furthermore, patients with two-ventricle physiology exhibited a significant survival advantage as compared with patients with single-ventricle physiology, overall and within each study group (Table 2). CICU and hospital LOS tended to be longer in the telemedicine period within all stratum (Table 3). Pairwise analysis within each period for year-to-year variations in hospital survival, type of ECMO cannulation, or cardiovascular physiology did not show statistical significance.
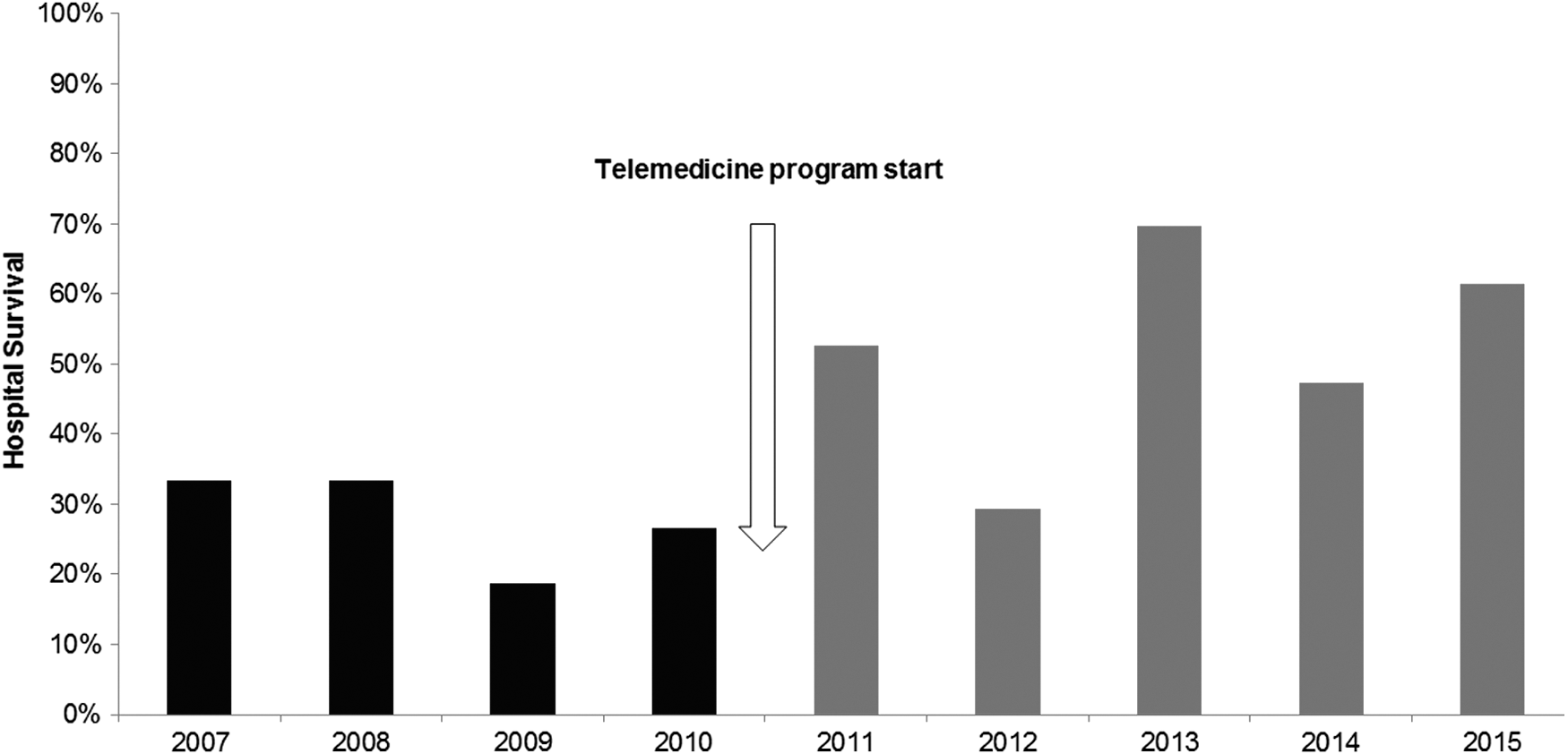
Hospital survival in patients on ECMO, by year.
Hospital Survival by RACHS-1, Cardiovascular Physiology, and Study Period
Chi-squared test
Fisher's exact tests.
Data are presented as n (%).
Length of Stay by RACHS-1 and Study Period
Data are presented as median (range); comparisons performed using Wilcoxon–Mann–Whitney tests.
Teleconsultations
A CICU physician from CHP participated in all the encounters, with other participant specialties including cardiovascular surgery and neonatology. Two hundred eighteen (n = 218) teleconsultations were provided to 49 patients. From those, a total of 64 real-time interventions were performed during 52 teleconsultations, with the most common being echo telementoring (46, 21.1%), followed by ECMO-related adjustments (12, 5.5%), pulmonary vasodilation test (3, 1.3%), inotropic support adjustment (2, 0.95%), and external pacing settings adjustment (1, 0.4%). Of note, among the 49 teleconsulted patients, 10 diagnostic changes were made with echo telementoring in 6 patients (12.2%). Also, a recommendation for diagnostic or interventional catheterization was made in 38 patients (77.5%), and cardiovascular surgery or surgical redo was suggested in 30 patients (61.2%). A summary of activities and recommendations provided during teleconsultations is presented in Table 4.
Teleconsultation Activities
Values presented as percentage from total teleconsultations.
Discussion
ECMO remains the last resource for the rescue of children with critical cardiopulmonary failure, including those with congenital or acquired heart disease. However, this technology is expensive, requires a highly skilled team, and significant effort must be exercised to improve proficiency during its use. Hence, hospitals implementing a new pediatric ECMO program would benefit from an expeditious increase in expertise and improvement in patient outcomes to justify such an expensive intervention. A telemedicine model can be used to leverage quality improvement interventions that may accelerate the learning curve in remote ECMO teams.
In this study, we observed a significant increase in patient survival during the telemedicine period as compared with a historical cohort from the same institution. Other significant findings were an increase in the proportion of cannulated patients with two-ventricle physiology, and of those cannulated in the OR. Telemedicine period patients had also significantly longer ECMO runs as well as CICU and hospital LOS. In addition, although improved survival for these patients was consistent across all RACHS-1 categories (category 2 excepted), the statistical significance within individual strata did not reach significance likely due to the small sample sizes within each group. Likewise, year-to-year variations in hospital survival, patients receiving OR-ECMO, and those with two-ventricle physiology were not significant, and we are unable to establish whether they represent normal random occurrences or else they were associated with other unaccounted factors.
Alternative possible explanations can be offered for some of these findings. Changes in patient referral patterns between study periods could explain differences in age, distribution of diagnostic categories, and cardiovascular physiology, and cannot be completely ruled out. However, the magnitude of these differences in a relatively short time span makes it unlikely.
We believe these findings may be at least, in part, associated with a change in approach by the team at FCV. An increased proportion of older patients, those with noncardiovascular disease, and patients with two-ventricle physiology may point to changes in selection criteria by the remote ECMO team. In addition, an increased proportion of patients cannulated in the OR could be associated with a change in model of care, suggesting a shift to a more proactive and preventive strategy. Particularly, an increase in the proportion of two-ventricle patients receiving ECMO in the telemedicine period is an important finding, given this is one of the populations most benefited with this technique, as evidenced by the significant survival advantage exhibited by them in previous reports as well as in this study. 19 Finally, a significantly increased length of ECMO runs in the telemedicine period may be associated with an improved ability to sustain appropriate support for longer periods of time, which, in turn, may allow improved cardiopulmonary recovery and survival. Multiple interventions within the ECMO program at FCV may have contributed to this change in collective approach, including those assisted with telemedicine. Significantly longer ECMO runs as well as CICU and hospital LOS seemed to be driven by increased hospital survival.
As related with the teleconsulted patients, there are some important observations to be made. A small but significant number of teleconsultations resulted in diagnostic changes during echo telementoring. Even more important, most teleconsulted patients received a recommendation for a diagnostic or interventional catheterization, as well as additional surgical procedures. These findings suggest valuable diagnostic and therapeutic advice resulting from the remote interaction.
Study Limitations
Given the retrospective, single-center nature of this study as well as the distinct features of telemedicine interactions, we cannot assign causality between our findings and the use of telemedicine or concurrent, on-site interventions. Telemedicine can be defined as a “complex intervention” that, in turn, is implemented into a “complex system” (CICU), with a potential to exert influence in all patients within the system independently from their teleconsultation status. 20,21 Thus, within the context of available information, we are unable to establish the relative contribution of each one of these interventions to the result. In addition, other variables with the potential to alter outcomes (i.e., serum lactate, mixed venous O2 saturation, and other biochemical markers of organ perfusion) were not available for analysis.
In summary, the implementation of an international telemedicine pediatric ECMO program enabled the delivery of a wide range of remote interventions providing educational content, telementoring, and valuable diagnostic and therapeutic advice. When compared with a historical cohort, it was also associated with an increased proportion of noncardiovascular and two-ventricle patients, of those cannulated in the OR, and an increased hospital survival. These findings may reflect a change in patient selection criteria and model of care in the remote ECMO program. Further research is warranted to establish which telemedicine interventions are more effective to improve patient survival and functional status in a multicenter setting.
Footnotes
Acknowledgments
We are indebted to the staff of FCV as well as medical and nursing staff of the Heart Institute at CHP for their enthusiastic support of our telemedicine collaboration. We thank Anderson Bermon, MD, for initial interrogation of clinical and administrative databases at FCV. We are especially grateful to Sara Mendoza, MD, for her support as a cardiovascular surgeon, first as part of teleconsulting physician team from CHP, and later as cardiothoracic surgeon at FCV.
Disclosure Statement
No competing financial interests exist.