
Abstract
Background:
A change in healthcare systems is needed, due to the increased prevalence of chronic diseases. Patient empowerment improves results in terms of patient quality of life (QoL) and satisfaction.
Introduction:
We have developed a telehealth program Control Telehealth Claudication Intermittent (CONTECI) for patients with peripheral arterial disease (PAD), aimed at enhancing patient satisfaction and QoL, while improving health system efficiency.
Materials and Methods:
We conducted a randomized clinical trial of patients with PAD, at the intermittent claudication stage. Study subjects were randomized into either (1) an intervention arm (IA), which utilized our CONTECI program for promoting patient self-management, or (2) a control arm (CA), utilizing the familiar system of in-person patient visits. All patients were followed up at 1 year.
Results:
The trial included 150 patients, 75 in each arm. Complications were diagnosed more quickly in the IA (7.85 days standard deviation (SD) 9.95 vs. 53.89 days SD 41.56; p = 0.016) compared with the CA. Rest pain decreased (1.4% vs. 8.4%; p = 0.05) in the IA group, as did the number of scheduled visits—decreased by 95.95%—and the number of emergency visits (p = 0.017). QoL scores in IA patients improved from baseline (67.87 vs. 72.25; p = 0.047), as did patient satisfaction (67.36 vs. 76.78; p = 0.03).
Discussion:
Telemedicine can improve health results and aid communication and visit scheduling. Our e-Health programs are financially viable.
Conclusions:
Self-management using the CONTECI telehealth program is feasible for patients with PAD. The program promotes patient expertise, encourages proactivity, increases QoL and satisfaction with disease control, and improves health resource use, with no evidence of clinical inferiority to conventional practices.
Introduction
The worldwide prevalence of chronic diseases is rapidly increasing; among such diseases, atherosclerosis is one of the most prevalent. The World Health Organization (WHO) 1 has shown that, in 2001, chronic diseases contributed to ∼60% (56.5 million) of the world's total reported deaths and accounted for ∼46% of the global disease burden. Chronic diseases have a high impact on quality of life (QoL) for both patients and families. Various studies highlight the importance of patient empowerment and the creation of expert patients. 2,3 An “expert patient” is defined as a person who lives with a long-term health condition, yet who is able to exert positive control over his or her health, by virtue of an understanding of and ability to manage the condition, and so improves his or her QoL. Becoming an expert patient is empowering for a person with a chronic condition. 4
Recent data show that in Spain, 77.6% of homes have Internet access, and 97.1% have one or more mobile phones. Existing studies—Renewing Health and TEMPis, for example—have demonstrated the possibilities telehealth offers for patient empowerment and for improving care quality and health systems. 5 –9
Peripheral arterial disease (PAD) is a manifestation of atherosclerosis. In developed countries, atherosclerosis affects between 3% and 10% of the population, and as many as one in five persons aged 65 years and older. Approximately 40% of subjects with PAD are in the clinical stage of intermittent claudication. Atherosclerosis reduces life expectancy by 8–12 years in patients older than 60 years. 10,11 In 2004, it was the primary cause of death worldwide, according to the WHO. Good control of the disease's risk factors decreases mortality. Therefore, patients need to be proactive, such as making changes in their own lifestyles. The natural history of PAD is stable over long periods; however, patients may experience complications that can necessitate amputation. Intermittent claudication is not a symptom of critical limb ischemia; however, when a patient has reached this stage, it is important to educate the person and promote lifestyle changes to limit disease progression. In addition, early detection of developing complications could save endangered limbs. Thus, it is essential that patients are able to recognize complications and take action if any should appear. Another problem is that visits to a healthcare provider are often not properly scheduled; what would normally be considered regular visits—every 6 months—are not sufficient where there are emerging complications.
We created a telehealth program called Control Telehealth Claudication Intermittent (CONTECI), which presents patients with a dynamic series of questions and answers. The program's purpose is to help improve patient education, empowerment, and self-management. The program also enables patients to contact their medical teams by e-mail. The aim of this study was to assess the efficacy of CONTECI as a monitoring tool for PAD patients at the intermittent claudication stage, in terms of clinical aspects, patient satisfaction, and QoL, as well as the program's value with regard to efficient use of health resources.
Materials and Methods
This e-health study was a pragmatic, parallel, randomized controlled trial, analyzed by the intention-to-treat approach, with a parallel control arm (CA) and an intervention arm (IA). It was a pilot study. The study population consisted of patients with stage II PAD, according to the Fontaine classification: intermittent claudication symptoms.
10,11
The study was registered with
Inclusion criteria were intermittent claudication confirmed by a vascular surgery specialist according to clinical, physical, and hemodynamic criteria, aged 18 years or older, signed informed consent, access to the Internet by the patient or a relative, and fluency in the Catalan and/or Spanish language.
Exclusion criteria were serious psychiatric disorder or cognitive impairment before consideration for the study, previous patent arterial surgery, severe chronic obstructive pulmonary disease (GOLD stage III/IV), severe congestive heart failure (NYHA class III/IV), and active malignant disease with expected survival of less than 1 year.
Patients in the Vascular Surgery Outpatient Unit of Mataro Hospital who met the criteria and provided their informed consent were enrolled and randomized. Included patients were randomized into either the IA or CA group, using sealed envelopes with details of the arm to which each coded patient was assigned. CA patients were monitored according to the standard protocol applied in the vascular surgery outpatient unit, which consisted of visits every 6 months. In case of complications or doubts, CA patients were required to go to an emergency room (ER) or primary care clinic. IA patients used the CONTECI program for self-management. Every 3 months they completed the program's dynamic questionnaire and, depending on the results, were advised to continue as before or to request a visit. Patients requested additional visits by e-mail, with a visit usually arranged for within 72 working hours of the request. Patients in both groups attended an initial visit and an end-of-study visit. The follow-up period was 12 months.
CONTECI—a dynamic program to guide and educate patients, which runs on a free platform—issues questions and, based on their responses, helps patients perform self-checks (see Appendix). It asks new questions and offers advice depending on the responses to previous questions (e.g., “Do you have an ulcer?” or “It is important to stop smoking.”). The program is accessed from a computer or mobile device (smartphone or tablet). To comply with Spanish data protection laws, patients were coded so that their questionnaires contained no information that revealed their identities, except to the researchers.
To estimate the sample size, the primary endpoint was established as patient satisfaction with disease control. For an alpha risk of 0.05 and a beta risk below 0.2 in a bilateral comparison, 74 subjects were required for both the IA and CA groups, to detect a difference of 10 or more units on the satisfaction scale. The standard deviation was set at 20 U. The estimated loss to follow-up was 15%.
The study was approved by the ethics committee on April 23, 2014, under code number CEIC 18/14. All participants provided written informed consent. All patients received medical treatment according to the standard protocol (antiplatelets and statins); some patients received pentoxifylline, cilostazol, or naftidrofuryl oxalate.
Satisfaction and QoL were assessed at the beginning and at the end of the study. Satisfaction—the primary endpoint—was evaluated using an analog 0–100 scale; QoL was assessed using the EuroQoL-5D instrument. 12
At 6 and 12 months, clinical data and healthcare resource use were evaluated. Clinical data assessed were walking distance, number of patients whose Fontaine classification had changed to stage III (rest pain) or stage IV (appearance of an ulcer), and number of surgical interventions. 8 –10 Walking distance was evaluated in three ways: (1) categorically in terms of four categories (<150, 151–500, 501–1,000, and >1,000 m); (2) subjectively in terms of improvement over the previous year (yes/no); and (3) subjectively categorically (walking more, less, or the same as at the time of the previous test). Healthcare resource use was evaluated in terms of ER visits for PAD, primary care visits for PAD, and phone calls made and e-mails exchanged by the patient or healthcare personnel. Visits to the vascular surgery outpatient unit were classified into three categories: scheduled checkups for the disease, study visits (baseline, 6, and 12 months), and additional visits due to a complication or specific request. Total monitoring visits were defined as the sum of scheduled visits plus additional visits.
Other endpoints assessed were adherence to prescribed drugs, exercise, and smoking. Drug adherence was assessed at baseline, 6, and 12 months using the Morisky-Green (M-G) test. 13
Exercise, defined as 30 min of walking or more strenuous activity, was assessed: walking more, less, or the same as at the time of the previous test or visit. It was assessed based on the patient's answers.
Smoking was assessed in two ways: quitting (yes/no) and whether cigarette consumption had increased or decreased.
Demographic information collected included age, sex, education, Internet access, cardiovascular risk factor, and Charlson comorbidity index. 14,15 This information was used to assess potential study dropouts.
Data were analyzed following the intention-to-treat principle. The groups were compared using the chi-square test for categorical variables, the Student's t test for continuous variables following a normal distribution, and the Mann-Whitney U test for continuous variables following a non-normal distribution. Variables were compared at baseline, 6, and 12 months. For paired variables, the tests used were the McNemar test for the categorical variables, the Student's t test for continuous variables following a normal distribution, and the Wilcoxon test for continuous variables following a non-normal distribution.
Results
A total of 150 patients were recruited, 75 randomized to the IA and 75 to the CA. A total of 12 patients (6 in each group) dropped out: 5 deaths, 1 terminal disease, and 6 voluntary withdrawals (4 CA and 2 IA). At baseline, 77.4% of patients had a Charlson comorbidity index score of 3 or higher (high comorbidity). Table 1 summarizes the demographic characteristics of both groups at the study's onset; no differences between groups were observed. We observed no difference in drug treatment between the two groups.
Patient Demographic Characteristics
CA, control arm; IA, intervention arm.
Satisfaction and Qo L
Satisfaction in the IA improved significantly between baseline and the 12-month assessment (67.36 vs. 76.78; p = 0.03). No significant differences in satisfaction were found between the two arms, IA and CA, at 12 months (76.78 vs. 70.75; p = 0.16). QoL also improved between the baseline and 12-month visits (p = 0.047). No significant differences were found in QoL between the two arms, IA and CA, at 12 months (72.25 vs. 67.24; p = 0.195) (Fig. 1).
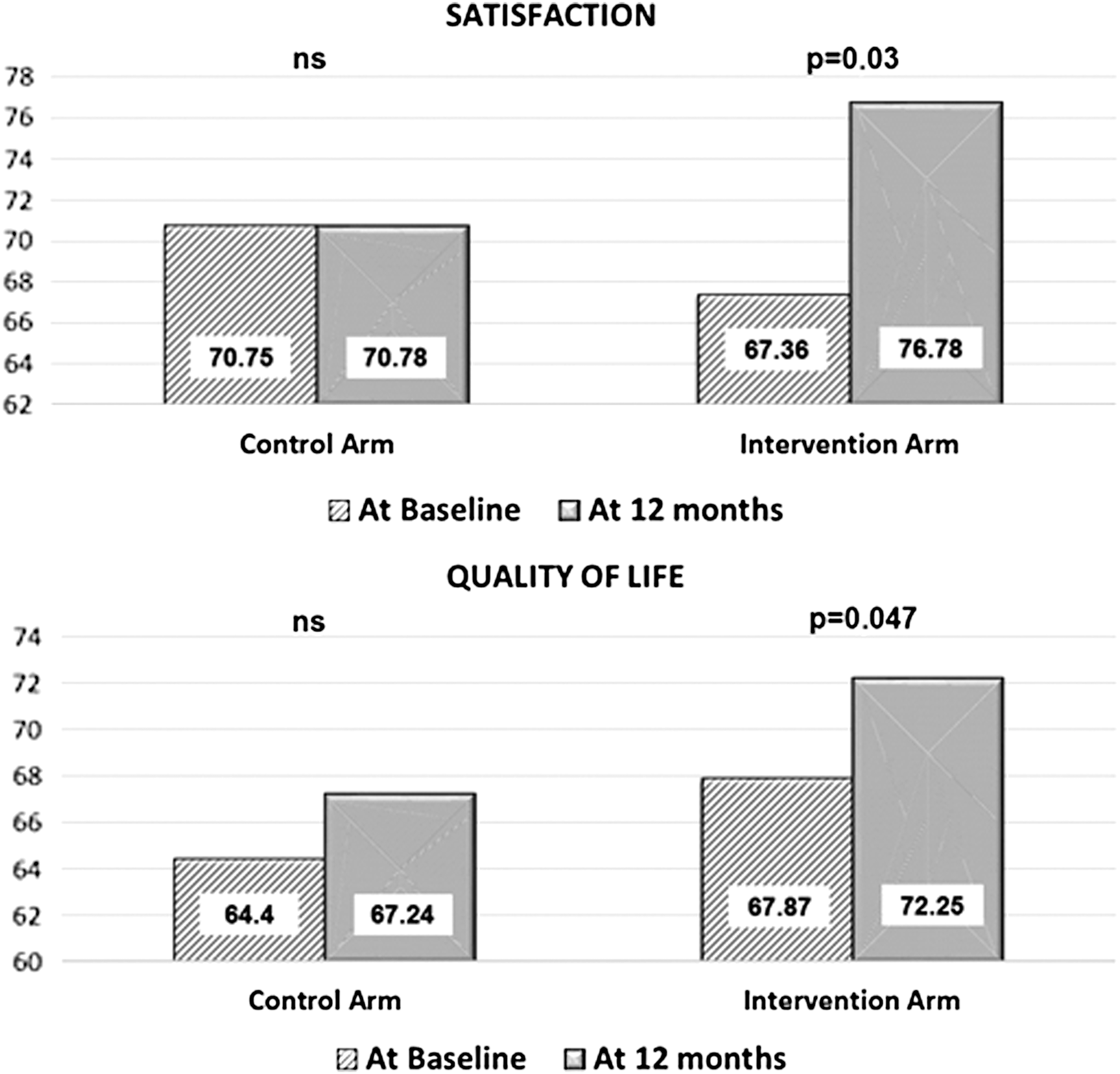
Satisfaction and QoL at baseline and 12 months. QoL, quality of life.
Clinical Features
No differences were found in any of the variables between the two groups at 6 months. Table 2, which summarizes clinical features at 12 months, shows that fewer IA patients progressed to Fontaine stage III (IA 1.4% vs. CA 8.4%; p = 0.05). When patients experienced a complication, IA patients visited sooner than CA patients (7.85 days vs. 53.89 days; p = 0.016).
Clinical Results at 12 Months
Treatment Adherence
At 6 months, adherence to treatment improved in IA patients compared with CA patients (83.8 vs. 69.0; p = 0.031), but this improvement was not maintained at 12 months (p = 0.317). No differences were found regarding smoking or walking (Table 3).
Treatment Adherence
M-G, Morisky-Green test.
Health Resource Use
Table 4 summarizes resource use data. Visits associated with PAD control by IA patients were reduced by 95.95% (p < 0.000), due to the decrease in scheduled visits. Additional, nonscheduled vascular surgery unit and primary care visits were the same in both arms. There were fewer ER visits by IA patients than by CA patients (0.19 vs. 0.017; p = 0.017).
Resource Use Over 12 Months
PAD, peripheral arterial disease; SD, standard deviation.
Discussion
To our knowledge, this is the first program to explore an application of telehealth to promote patient expertise and self-management in PAD. The CONTECI program can be valuable for patients with PAD. Our study found an improvement of patient expertise, QoL, and satisfaction; use of health resources was also lower in IA patients, compared to baseline. These results are in line with findings of previous studies which have demonstrated that developing self-management and patient empowerment increases disease acceptance and improves treatment patient adherence as well as QoL. 2,3,16,17 Why is it important to promote patient expertise? Chronic diseases last much longer than acute diseases, and the practical challenges of monitoring growing numbers of patients with chronic diseases 24 h a day, 365 days a year over many years are insurmountable. Chronic diseases have social, physical, and psychological causes, lead to QoL deterioration, and affect patients, relatives, friends, and the community. There are real costs to patients and their families due to absence from work, drug-related expenses, psychological problems, and so on. Since healthcare resources are limited, new solutions are needed to improve QoL, satisfaction, and resource efficiency. 16,18 –20 Different models have emerged in which information, patient empowerment, and use of telehealth are cornerstones (Kaiser Permanente HealthConnect™; Veterans Health Administration, Whole System Demonstrator British National Health Service, etc.). Studies have shown reductions of 45% in mortality, 20% in emergency hospitalization, and 15% in emergency visits, and increased survival at 4 years. 21 –32
Our model aims to be an innovative system in outpatient monitoring, through promoting patient expertise, and by bringing doctor and patient together (while avoiding a paternalistic system). The doctor and the patient are seen as a team; working together, they can improve QoL. It is necessary to teach patients to recognize complications so they can ask for help, thereby making them responsible for health self-management and promoting changes in lifestyle to better control risk factors. This program provides increased frequency of contact with the patient. Because it is available 24 h a day, 365 days a year, and there is no limit on its use, the program allows for intensifying patient education regarding the activities and challenges of self-treatment: exercise, diet, and so on. For this reason, although patients in the control group are visited at the usual 6-month intervals, patients in the intervention group are contacted every 3 months. This more-frequent contact is one of the benefits of telemedicine. Our study results showed that complications were detected in IA patients (telehealth) earlier than in CA patients. The CONTECI program includes a tool for improving patient knowledge, helping them to identify deteriorations or complications and guiding them toward self-management and improved decision-making. It is known that the sooner a heart attack or stroke is detected, the more patient tissue is saved (“time is tissue”). For patients with PAD, early detection of complications may save a limb. The WHO actively promotes patient involvement by structuring therapeutic education in different activities aimed at helping patients and their families acquire disease-related knowledge and skills; this promotes health self-management, improves QoL, enhances treatment adherence, alleviates anxiety, and reduces complications and the number of emergent situations. 33 –38 In our study's IA arm, more ulcers were detected due to patient education, and the shorter time between complication detection and treatment reduced the number of surgeries required. Similarly, dynamic scheduling of visits prompted by the CONTECI questionnaire results improved the healthcare provider response times.
In this study, the QoL of IA patients improved from baseline (p = 0.047). This can be attributed to the involvement of the patient, and the CONTECI program lifestyle recommendations for a healthier life and improved risk factor control. The study also found IA patients to be more satisfied (p = 0.03). This may be explained by their greater expertise and by improved communications with their doctors. Other studies have demonstrated that self-management improves satisfaction. 27,28 Higher patient satisfaction has also been shown to improve treatment adherence. 39 –41 Treatment adherence improved (in the IA group) in the first part of our study period, but this improvement was not maintained, probably due to lack of patient motivation. Apparently, when they begin using the CONTECI program, patients feel more controlled, and thus, they improve; after 6 months, however, the questionnaire becomes routine and motivation declines. To improve and maintain outcomes, motivating and changing initiatives must be developed. Dynamic actions are likely to be necessary to ensure ongoing lifestyle-change efforts by patients. Improved treatment adherence is likely to improve clinical outcomes—not only for PAD, but also for other manifestations of atherosclerosis such as myocardial infarction and cerebral ischemia. Gamification may also be a useful tool for increasing and maintaining patient engagement and participation.
Costs are another crucial issue with chronic disease, for patients as well as for healthcare systems. As mentioned above, chronic diseases account for 83% of healthcare expenditures and 91% of drug prescriptions. Given that healthcare resources are limited, 19,20 innovative solutions and new models are needed to improve health system efficiency. Results for CONTECI, designed to improve resource use related to PAD, show that the program reduced healthcare costs, mainly by decreasing visits by IA patients (p < 0.000). Further savings were realized due to fewer ER visits. Not unexpectedly, there was a small increase in the number of calls and e-mail exchanges between patients and providers. However, since complications are detected earlier as a result of greater patient expertise and better communication, hospital stays could be expected to be reduced in the long run, representing greater savings for the healthcare system and also for patients and their families.
Technological advances have made telehealth programs possible, as has been demonstrated by various studies. The major limitation remains, however, financial. In most studies—for instance, RENEWING HEALTH and iCor—the patient is supplied with the necessary equipment (iPads, pulse oximeters, smartphones, sphygmomanometers, etc.). This level of expenditure is not always possible. Our study was financially feasible because it relied on patients using their own devices; this also provided the advantage of patient prefamiliarity with the technology, reducing the need for additional training. The problem of equipment obsolescence (mobile phones, tablets, computers, etc.) is also solved when patients are responsible for their own equipment. This approach to telehealth is potentially applicable to other disorders in the fields of ophthalmology, endocrinology, orthopedics, and so on.
One limitation of our study was the selection of patients most likely to benefit from using a telehealth program. Further studies would need to define the best target patients. Although in our 12-month study period there was evidence of better clinical results (reduced time to detect complications and reduced number of surgeries), a longer follow-up would be required to show whether there was also a decrease in amputations. An increase of QoL was observed, however. The use of a better platform could also yield better results in further research. Comparison with other studies was not possible, because we found no other study on telehealth and PAD.
Our study demonstrates that self-management using telehealth is feasible for patients with PAD at the intermittent claudication stage. The innovative CONTECI program promotes patient expertise; it adds value because it is workable, efficient, and improves satisfaction and QoL, with no clinical inferiority to conventional management.
Footnotes
Acknowledgment
We wish to thank Russell Williams of
Disclosure Statement
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. No competing financial interests exist.