
Abstract
Background:
The increasing number of diabetes mellitus (DM) m-health applications (apps) reveals a panorama of different approaches to the subject, demonstrating dynamism and heterogeneity. Available applications have various functions, capabilities, and data collection techniques.
Objective:
We systematically reviewed the literature to identify and analyze studies regarding the diversity of applications aimed at DM monitoring and treatment. We aimed to investigate app functionalities, the basis for their design, and how they were tested.
Materials and Methods:
We conducted a systematic literature review in Association for Computing Machinery (ACM), Institute of Electrical and Electronics Engineers (IEEE), ScienceDirect, Springer, and Medical Literature Analysis and Retrieval System Online (MEDLINE) databases. The search considered studies published until April 2017, without language restrictions.
Results:
After removal of duplicates, 679 studies were screened and assessed for eligibility, when 39 studies met the inclusion criteria. We present tables summarizing the functionalities, features, fundamental techniques, and methods.
Conclusions:
There is a variety of approaches used in the DM apps, with comprehensive, customizable, and adjusted functionalities for different purposes. Most apps are digital logbooks for collecting data on various daily tasks from DM treatment. The researchers are interested in guidelines of medical organizations, evaluations from health professionals and patients, and other methods to verify accuracy and reliability.
Introduction
The metabolic disorder diabetes mellitus (DM) is characterized by symptoms such as hyperglycemia and disturbances in the synthesis of carbohydrates, proteins, and fats, due to failure in the secretion and action of insulin. 1 Negligence in the disease's treatment is a high-risk factor and is associated with the manifestation of microvascular complications such as retinopathy, nephropathy, and neuropathy; along with macrovascular diseases, such as peripheral arterial disease, carotid disease, coronary artery disease, 2 and its chronic pathologies. The common practice of monitoring glucose fluctuation and adopting tasks to manage the use of insulin, medications, and healthy diet and physical activity habits is effective in mitigating these complications. 3
Population aging, urbanization, and increasing prevalence of obesity and sedentary lifestyle have resulted in an increase in the number of DM patients worldwide, 3 currently estimated at 415 million adults, projecting 642 million for 2040. 4 Simultaneously, the popularization of information and communication technology enabled access growth to mobile devices, such as smartphones and tablets, are used by its resources in the management of various tasks in everyday life, 5 especially those related to health.
The m-health concept covers the evolution of e-health systems from traditional telemedicine platforms to mobile and wireless configurations. 6 Currently, m-health represents the focus of various applications (apps) for mobile device operating systems such as Android and iOS. 7 There is a broad range of mobile device applications utilizing one or more functionalities in the routine treatment of DM. Among these functionalities, there are some tasks like elaborating diaries and glycemic indexes, plotting drug interaction graphs, calculating and recording insulin doses, carbohydrate counting, and the monitoring of physical activities. 8
Although the functionalities of m-health apps are diverse in DM management, they seem to favor digitally collecting, storing, and interpreting data. Mobile devices can be an effective strategy for many healthcare providers and organizations that are looking for cost-effective ways of providing high-quality healthcare to patients. 9 Results of studies show the positive effect of using m-health solutions on the HbA1c (Glycated Hemoglobin) laboratory test indices, the main indicator of DM treatment. 10 In addition, compared to usual care of DM treatment, m-health solutions present improvements in adherence to medication and glycemic measurements. 11
The increasing number of m-health DM apps reveals a panorama of different approaches to the subject; however, it is characterized by limited data studied and established. 12 Besides demonstrating dynamism and heterogeneity, the apps differ in functionalities and capabilities, 12 with different data collection techniques, user engagement, usability, and intervention methods. In these circumstances, guidelines proposed by institutes of health and diabetes organizations, such as the American Diabetes Association, 13 are often taken as guides for app development. Nonetheless, these authorities' documents predominantly contain medical literature, procedures, and components for the disease treatment, with minor specifications about the involvement of computational solutions, its implications, and how these solutions should be developed.
Although mobile apps are available in repositories like Google Play Store and Apple App Store, scientific literature contains reliable studies thoroughly detailed. Moreover, m-health apps developed in these studies provide a vast knowledge base on research and do not suffer from distortions of commercial influence. Therefore, this article systematically reviewed the literature to identify and analyze studies regarding the availability and diversity of apps aimed at DM monitoring and treatment. The study aims to investigate application features and functionalities, the basis for their design, and how they were tested to support patients' safety and reliability assurance.
Materials and Methods
This research presents a systematic literature review (SLR), performed between March and July 2017. An SLR is a secondary study, which uses a protocol with explicit methodology in an impartial and auditable way to identify, analyze, and interpret all the available evidence related to a specific research question. 14 We included studies like clinical trials, observational study, case reports, development of technological products, and others from health sciences and computer science.
This research had three key questions as follows: (1) What m-health apps support diabetes mellitus? (2) What features do they have? (3) What was the basis for their design and how were they tested?
Search Terms, Databases, and Criteria
The search string was idealized with keywords aligned according to the study context intended in the search, as it follows: (A1 OR A2 OR A3 OR A4) AND (B1 OR B2 OR B3 OR B4) AND (C1 OR C2 OR C3).
Table 1 shows the expression constructed with the search terms. The first column specifies synonyms for the disease nomenclature; the second column lists software applications; and the third column addresses mobile devices. Synonyms related to DM were extracted from the DeCS structured vocabulary service. 15
Search Terms
The search expression remained unmodified for all databases, considering the specifications of each search engine. The filter was applied to keywords, title, and abstract. The research considered all primary studies published until April 2017, the period when database research ceased. There were no restrictions regarding publication period. No language restrictions were applied to expand the search and make it more comprehensive.
The study used multidisciplinary bases, from Computer Science and Health Sciences: • Association for Computing Machinery (ACM); • Institute of Electrical and Electronics Engineers (IEEE); • Medical Literature Analysis and Retrieval System Online (MEDLINE); • ScienceDirect; • Springer International Publisher Science, Technology, Medicine (Springer).
Eligibility criteria for result inclusion in the final analysis are described below: • EC1. Use mobile devices allowing user interaction; • EC2. Address at least one task for monitoring a variant of DM (ICD-10 groups E10-14 or O24); • EC3. Discuss at least one app function characteristics; • EC4. Explain how app functions were tested/supported by health science.
Study Selection Process
The study selection process was systematically structured in three stages as follows: Stage 1. Identification: search expression executed in all databases previously described, according to the specifications of each search engine; Stage 2. Screening: publication title and abstract reviewed as a preliminary examination to determine if they contained information relevant to the key questions, also resulting in the exclusion of duplicate articles; Stage 3. Eligibility: studies evaluated with a full reading to settle their adequacy to the eligibility criteria, culminating in the SLR composed by the included studies.
Two researchers simultaneously and independently performed the selection process. Evaluations with identical results were maintained, while divergent evaluations underwent a new analysis conducted jointly by the two researchers to reach the final decision.
Results
Selection Process Analysis
From March to April 2017, the SLR identified 735 articles in the surveyed databases, based on the search strategy adopted. At first, 56 studies were removed for being duplicates, and 524 were excluded for not presenting affinity with the key questions in their titles and abstracts. With an appraisal of the full-text articles against the eligibility criteria, 116 studies were excluded, resulting in 39 articles included in this study (Fig. 1).
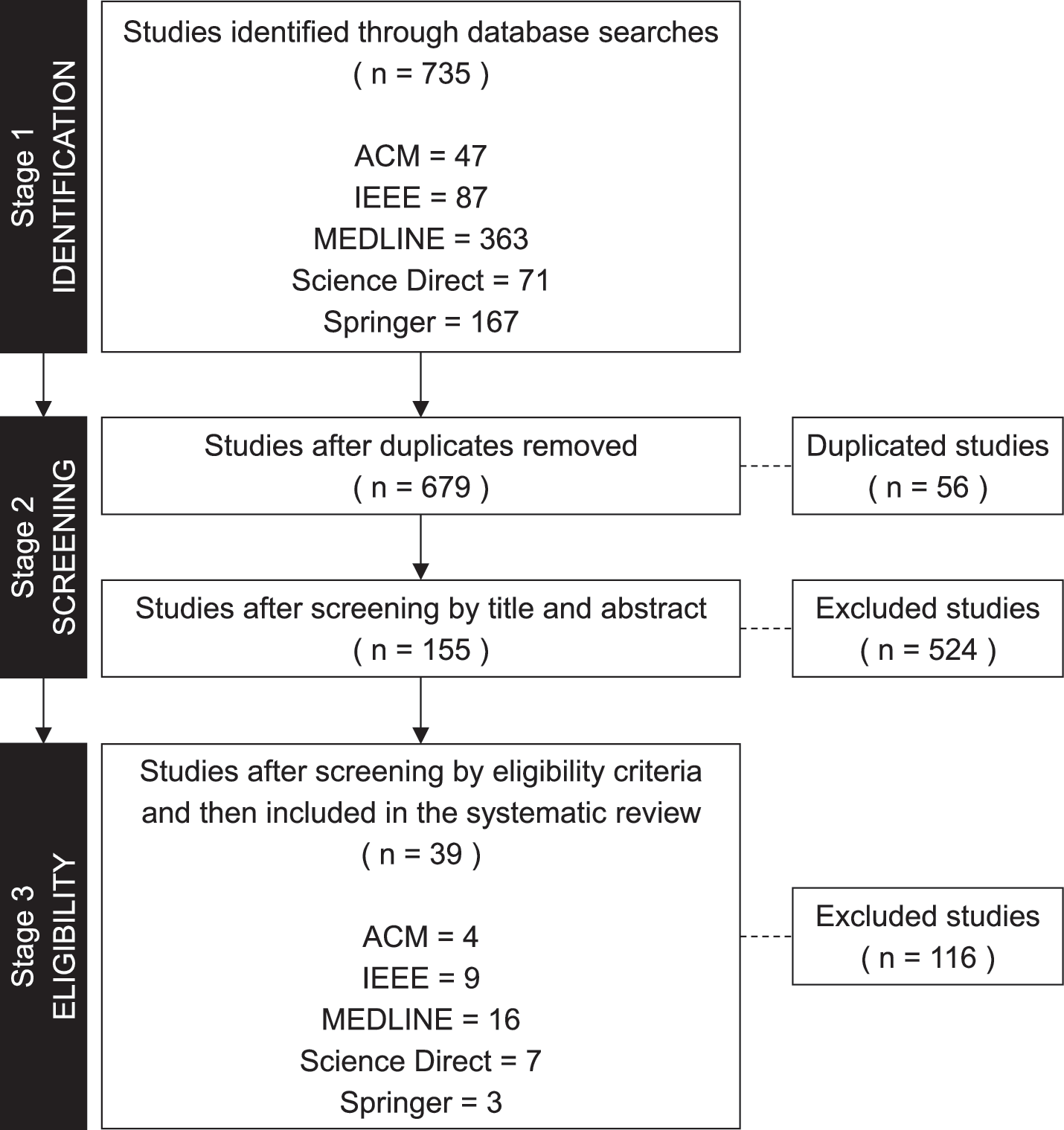
Flow diagram of selection process for included studies. ACM, Association for Computing Machinery; IEEE, Institute of Electrical and Electronics Engineers.
By year of publication, 17.9% of studies (n = 7) were published between 2009 and 2013; 15.4% (n = 6) in 2014; 28.2% (n = 11) in 2015; 28.2% (n = 11) in 2016; and 10.3% (n = 4) until April 2017. The oldest study was published in 2009, and since no date filter was applied in the selection process, results show that the researched topic is highly visible in present day. There is a significant growth of interest in the area, as publication number increased since 2013.
After the selection process, studies from different databases were included in the SLR. Of the included studies, 10.3% (n = 4) were from ACM; 23.1% (n = 9) were from IEEE; 41% (n = 16) were from MEDLINE; 17.9% (n = 7) were from ScienceDirect; and 7.7% (n = 3) of the studies were from Springer. This statistics denotes the importance of including studies from different databases to produce a broad, comprehensive, and impartial scientific study. In this scenario, it is important to understand Computer Science as an applied field of study.
Key Question 1: What M-Health Apps Support DM?
Although operating system specification is a technical attribute, the landscape identified in the literature may not reflect the scenario seen in commercial repositories, like Google Play Store and Apple App Store, where the public usually browse and download apps. Considering an operating system, apps available exclusively for Android were 56.4%; exclusively for iOS were 18%; available in both Android and iOS were 7.7%; Windows Mobile represented 5.1%; while other 12.8% of the studies did not specify operating system.
In addition to m-health, 11 studies report integration with a Web page. Web versions are dashboards where patients and health professionals have access to treatment information. Pages can optimally display data entered detailing treatment performance, with corresponding averages charts and trend lines. The interaction between health professional and patient occurs for remote performance monitoring, in which health professionals can update treatment tasks and exchange messages with their patients as an intervention method.
Complementing the literature view, a search on the Google Play Store, Apple App Store, and Microsoft Windows Store was performed. We did this to investigate the perpetuity of apps from the evaluated studies on commercial repositories. Our goal was to map an overview of the solutions presented in the literature and the ones available to the public at the same time. The search was performed with app names reported in the studies and names found in screenshot figures. Search result similarities found (Table 2, Commercial Application) in app repositories were compared to the content found in the reviewed studies (e.g., screenshots, country of origin, authors, or institution) to facilitate identification. There are few initiatives aimed at making the solutions developed in scientific research available for end users. A reliable survey of apps repositories requires more research, capable of dealing with the fast changes within app context, along with possible commercial influences on app content.
Summary of Features and Functionalities
FAQs, frequently asked questions; DM, diabetes mellitus.
Key Question 2: What Features Do They Have?
In Table 2, we summarize features and functionalities identified in the 39 articles included in this SLR. The categorization was created according to an interpretation of DM management tasks specified by American Association of Diabetes Educators (AADE) 16 and Brazilian Diabetes Society (SBD). 3 Additional correlated functionalities are also presented to further comprehend their involvement in the disease treatment and its frequency in the apps described by the reviewed studies.
Table 2 details functions related to glycemic fluctuation and use of insulin and other medications, along with functionalities related to maintenance of adequate life habits as nutritional control, sleeping record, and practice of physical activities and sports. Table 2 also shows distinct functionalities aimed at monitoring other DM essential indicators and casual comorbidities. Additional functionalities include approaches to reduce the risk of forgetting tasks, evaluation, and individualized treatment recommendations, view of educational content, patients and medical staff remote interaction, and app integration with devices for automatic data retrieval, such as blood glucose meters, blood pressure meters, pedometers, and other sensors.
All apps had two or more features. The apps addressed DM treatment tasks differently, but all had the same purpose, which was daily self-monitoring. Not all apps had features for registration of every essential task of DM treatment, such as blood glucose, food intake, medication, and physical activity. Even essential to DM monitoring, blood glucose recording was not possible in all the apps (available only in 89.7%, n = 35). In these cases, the focus of the apps was exclusively diet, physical activity, and sports. All apps allowed manual data entry, but only 30.8% (n = 12) had integration with some electronic device to automate data collection.
While most of the apps were simple digital logbooks, few (28.2%, n = 11) were able to automate some tasks, such as carbohydrate counting or insulin dose calculation. Less than half (n = 18, 46.2%) of the apps used the recorded data to make personalized recommendations to patients, which could serve as a user engagement factor. Few apps had enough features to suit all AADE 7 Self-Care Behaviors. 16 However, a full appraisal of apps' compliance with AADE precepts requires further research.
Key Question 3: What was the Basis for Their Design and How Were They Tested?
Authors used various methods and techniques to obtain an app capable of supporting security and reliability to users. They based their apps on guidelines and recommendations from health organizations, made clinical trials, and used evaluations from health professionals and patients. We summarize in Table 3 resources used in the applications' design, which helped in the study development. Table 3 also details methods used to verify acceptance, accuracy, and reliability of the apps. These methods aided in evaluations and tests performed with the purpose of inferring criticisms about effects, quality, accuracy, suitability, usability, and other aspects of the developed apps.
Summary of Fundamental Methods and Techniques
Discussion
Although functionality specifications simplify the explanation of app contents, apps with same features may not address a particular issue in the same manner. For a most useful understanding of the whole background, it is useful to recognize the existence of different approaches conceived by the authors and their study objectives. Such approaches reflect a myriad of possibilities by addressing a target audience under the many morphological, geographical, and social differences among thousands of people affected by DM.
Some authors consider geographic restrictions, such as Kasmeridis and Vassilakopoulos, 35 focusing on features for the Greek culture, while Alanzi et al. 41 idealized his app for people of Saudi Arabia. Khan and Khan, 45 also as Borrero et al., 30 focused their research on elderly, with large and concise elements in the app's graphical interface, to minimize adverse effects caused by human aging. Holtz et al. 53 created an m-health app to attend adolescents with DM accompanied by their parents. Jo and Park 44 and Garnweidner-Holme et al. 34 adjusted their apps for gestational DM, which requires additional care such as diet and body mass control in agreement with the woman's gestational age, highlighting disease factors that can impact on the fetus growth. Among characteristics with outstanding features, the app by Rhyner et al. 49 estimates carbohydrates automatically. The user takes photos of his or her food dish using the smartphone camera, and a computer vision module calculates carbohydrate content of the food dish. Tkachenko et al. 50 developed an app capable of analyzing blood glucose history measurements to predict episodes of nocturnal hypoglycemia.
Some apps' functionalities did not address the treatment tasks adequately, partially recording data or not displaying reports on the recorded data. In these cases, some apps' functionalities allowed the meal records, but without the detail of carbohydrates, calories, or protein; some apps would count carbohydrates but not record them in logs; and some apps allowed the registration of glucose, but did not display data graphs. However, most apps had additional features, such as custom assessments and recommendations, goal setting, and communication with medical staff and caregivers.
Some important tasks for DM treatment were poorly explored within the apps. Even with some features on educational content and DM training, studies have insufficiently clarified what kind of content was available. There were very few mentions about features of feet care and sensitivity of body members for preventing peripheral neuropathy. There was no mention of some functionality that addressed care with dental problems related to DM. There were no functionalities addressing issues such as water intake, urinary frequency, and an association with glycemic control to prevent nephropathy. Few studies explained functionalities that referred to DM training to prevent or treat comorbidities, such as dyslipidemia, hypertension, retinopathy, and so on.
The specific use of typical type 2 DM drugs, such as metformin and sulfonylureas, was not addressed in functionalities of the apps. The integration with insulin pumps was weakly present, considering the restrictions on specific hardware integration. Resources about use of insulin were simple records of doses and schedules, and only two studies mentioned issues such as storage instructions, handling, and needle exchange reminders. A feature that was not addressed by any study and is interesting to be developed in future apps is some logbook of insulin injection sites.
It is known that it is difficult to orchestrate many healthcare tasks and the large number of data that come up in the daily DM treatment. Developers of new and upcoming apps need to find ways to simplify the user's data logging process to avoid making it a tedious task for the user. Likewise, future apps need to be empowered to drive users' engagement and motivation over time, avoiding the abandonment of the apps' usage.
Multiple approaches can be seen in DM apps, indicating the context diversity, whereas affirm that particularities of people's needs influence their perception of technology and the design process elaborated by app developers in their solutions. The different approaches applied in the app designs lay their fundamentals on several possibilities. Literature research can be considered a technique to support applications' reliability to patients. Although inherent in scientific practice, literature research was reported in only one-third of the reviewed studies. Even with no explanation about the used strategy, other studies may have used it as well. Nevertheless, studies that researched the literature used combined techniques to ensure their findings.
Authors briefly explored guidelines of health organizations, since they are not sufficiently specific about the involvement of computational solutions. Research in commercial repositories was a technique underused for new DM app design. Authors elaborated a method to estimate which solution should be developed and to propose new improved approaches, aiming at identifying the most applied functionalities, gaps, problems, and public's acceptance. This technique had a commercial bias, seeking features already made available to the public, assembling them into a more comprehensive and extended app project.
The involvement of patients as a resource used in the app design and development process was used less often than involving the patients in postdevelopment assessments. In the first case, the involvement of patients with observation, interviews, and questionnaires helped to understand users' needs and to collect requirements for the development of functionalities. With these techniques, the authors assimilated the differentiated audiences' particularities, such as regional characteristics, elderly limitations, and gestational DM.
Patient involvement in postdevelopment assessments was performed in more than half of the reviewed studies. User feedback allowed the authors to validate their solutions to identify success and failures in several aspects. Usability was the most recurrent factor among evaluations. Implications of using features like acceptance, engagement, user experience, and associated factors were also evaluated in most of the studies. Generally, studies reported user testing returned positive ratings. Projects which identified flaws during the development process mentioned that improvements and adjustments were made later in their apps.
Another important evaluation technique was the involvement of health professionals. In most studies, professionals were authors and coauthors. Thus, their participation might have contributed to the development of well-structured apps from the medical perspective. However, few studies explained how this involvement occurred. Reports mention that the professionals evaluated factors such as the app potential and the recommendations' accuracy. In specific cases, technical accuracy and performance experiments were executed to discover if apps produced the correct recommendations or accomplished safe predictions and calculations for users. Some apps have also been used in clinical trials on indicators in laboratory test results, to understand their influence on patients' lives. The involvement in these studies provided satisfactory and encouraging results on the positive potential of using apps in DM treatment and monitoring. However, studies that assess the motivation of users of a DM application over long periods, such as more than 6 months, are needed because most of the current studies use shorter periods to evaluate interventions with DM m-health apps.
Limitations
There are some limitations to this study. We used specific search terms, which may not have captured all the articles on the research topic. Apps available to the public may not be described in literature studies, thus, the features of the apps described in the literature may be different from the apps' features used by the public. We have included different studies from diverse backgrounds in computer science and health sciences. Not all studies were at the same progress level, some described app development, others user testing, and some studies detailed clinical trials of interventions. No quality appraisal was performed to differentiate sample size of the test populations, studies that performed tests with users, or whether the tests produced good results. Some studies had relatively small patient populations, and others did not focus on developing specific apps for a DM type, such as type 1 or type 2. We classified the apps according to what the authors described in their studies. Consequently, to get results that are more accurate, we would need to have access to the original apps to perform tests.
Conclusions
This systematic review identified 39 studies in the scientific literature highlighting the aspects of m-health app functionalities for DM, along with the characteristics of fundamental techniques. The answers provide a basis for future research related to proposing or developing new apps with a similar purpose.
Results show a variety of approaches used in the apps, with comprehensive, customizable, and adjusted functionalities for different contexts, patients, and their needs. The designing techniques confirm that the researchers are interested in guidelines of medical organizations, evaluations from health professionals and patients, and other methods used to verify accuracy and reliability. Some studies also demonstrate that intervention with m-health apps produces excellent effects.
Most apps are simple digital logbooks for collecting data on various tasks from DM treatment. However, some initiatives already use an entire set of stored data to generate customized reports containing information on patterns and similarities in some DM behaviors, including custom recommendations.
DM, in its variant forms, is a disease that demands extensive care of many factors related to patient's welfare and health. The main factors are glycemia, diet, insulin, medications, and physical activity. Extensive disease characteristics and clinical case particularities make it possible to use a wide range of approaches in the apps for DM.
Although the description of m-health applications in the scientific literature is richly detailed, the identified panorama may not reflect the same scenario in commercial repositories, where the public typically browses and downloads apps. To survey this scenario in future research, new and innovative approaches will be required to match the speed and evolution of new apps.
Footnotes
Acknowledgments
The authors would like to thank Hugo Roberto Kurtz Lisboa, MD, PhD, for his insight and feedback. The authors would also like to acknowledge Brazilian organizations CNPq, CAPES, and Fundaçāo Universidade de Passo Fundo.
Disclosure Statement
No competing financial interests exist.