
Abstract
Background:
For acute ischemic stroke patients, shorter time to thrombolytic (tissue plasminogen activator [tPA]) is associated with improved outcomes.
Introduction:
Telestroke increases tPA use at spoke hospitals, yet its effect on door-to-needle (DTN) times for tPA administration is unknown. We hypothesize that spoke hospitals with more frequent contact to a hub hospital will have shorter DTN times than those with less frequent contact.
Materials and Methods:
We identified 375 patients treated with tPA by conventional or telestroke methods in an academic hub-and-spoke telestroke network for whom date and time data were available. Strength of the spoke–hub connection was the primary predictor variable, defined as the number of all telestroke consults (tPA and non-tPA) done at each spoke hospital during the year of the patient's presentation. Patient-level regression analyses examined the relationship between DTN time and spoke–hub connection during the year of the patient's presentation, controlling for temporal trends and clustering within hospitals.
Results:
Sixteen spoke hospitals contributed data on 375 tPA-treated patients from 2006–2015. Hospitals treated a median of 13.5 patients with tPA per year; median hospital-level DTN was 78.8 min (interquartile range [IQR] 71.3–85). Median number of telestroke consults per year was 34 (range 3–137). Among all 375 patients, median DTN was 76 min (IQR 60–97). Strength of spoke–hub connection was significantly associated with faster DTN time for patients (1.3 min gain per 10 additional consults, p = 0.048).
Conclusions:
More frequent contact between a telestroke spoke and its hub was associated with faster tPA delivery for patients, even after accounting for secular trends in DTN improvements.
Introduction
Background and Importance
Stroke affects greater than 6.8 million Americans, and the majority of stroke survivors experience diminished quality of life and work-limiting disabilities. 1,2 Tissue plasminogen activator (tPA) reduces long-term disability from acute ischemic stroke (AIS) when delivered within 3–4.5 h of symptom onset, and faster time to treatment is associated with increased likelihood of good outcome for patients. 3 –5 Yet many eligible patients do not receive the treatment. 6 Among patients that are treated, there is substantial variation in door-to-needle (DTN) times for tPA treatment, with many patients treated outside of the guideline-recommended 60 min window. 7 –9
Telestroke has been associated with improved thrombolysis rates in neurologically underserved community hospitals. 10 –14 Yet, its impact on DTN times for tPA delivery is not well described. Telestroke may introduce delays, for example through technological difficulties or additional physician evaluations. Alternatively, with repeated spoke–hub contact and increased opportunities for knowledge transmission, telestroke may lead to improved DTN times through improved decision making or more efficient processing.
Goals of this Investigation
We aimed to describe DTN performance among spoke hospitals connected by telestroke to a single academic hub to determine whether the strength of a spoke hospital's connection to the hub hospital was associated with patients' DTN time for tPA delivery. We hypothesized that DTN times would be faster for AIS patients presenting to spokes with more frequent interaction with the hub (i.e., stronger connection).
Materials and Methods
Study Design, Setting, and Selection of Participants
Within the Partners Telestroke Network, Massachusetts General Hospital (MGH) supported 16 spoke hospitals in Massachusetts, Maine, and New Hampshire. Spokes were of varying size and ownership, and participated in the network for varying periods of time during the 2006–2015 study period. Hospitals contributed data on all tPA-treated AIS patients–this included AIS patients with and without telestroke consultations. This study was considered exempt by the Institutional Review Board.
Each spoke hospital contributed data on all AIS patients treated with tPA at their hospital during a given period. The duration of data contributed varied between hospitals because of differing duration of participation in the network and unique methods for data capture. During the study period, 14 hospitals joined the network, and 1 hospital left the network. The hospital that left the network cited new corporate reorganization or affiliation as the reason for their departure [personal communication]. Data included date and time stamps for hospital arrival and tPA treatment. We excluded patients with missing or implausible DTN times (>270 min) (4% of sample, n = 16).
We also extracted data from our network's telestroke consultation logs. All telestroke consults are entered in the network database by the consulted hub neurologist using an online web-based portal. Data are stored centrally on a secure server at MGH.
Measurements
Our primary predictor was the strength of the spoke–MGH connection. This was defined as the number of telestroke consults completed at the spoke during the year of the patient's presentation (all consultations regardless of tPA recommendation). We extracted this from the telestroke consultation logs.
Outcome and Analysis
The primary outcome was patient DTN time. We used descriptive statistics to characterize patients' DTN times and hospital characteristics. We used unadjusted linear regression to examine the relationship between DTN time and year of presentation. We used patient-level linear regression analysis to examine whether the primary predictor (strength of the spoke–MGH connection during the year of the patient's presentation) was associated with patients' DTN time. We included year of presentation to take into account temporal trends, and we accounted for clustering of cases by hospital. We made posterior predictions of the average marginal effects of the primary predictor on DTN, holding other variables constant. We generated a figure based on predicted DTN times by strength of spoke–hub connection, with bars indicating 95% confidence interval around predicted values. All analyses were completed in StataSE 14.2 (College Station, TX).
Results
Hospital Characteristics
Sixteen hospitals contributed data on 375 tPA-treated patients between 2006 and 2015 (Table 1). Participation ranged from 3 to 14 years, and available data varied by hospital (range 1–9 years). Hospitals treated a median of 13.5 patients with tPA per year (interquartile range [IQR] 9–28) with median hospital-level DTN time of 78.8 min (IQR 71.3–85). Median number of telestroke consults per year was 34 (range 3–137). The network is illustrated in Figure 1.
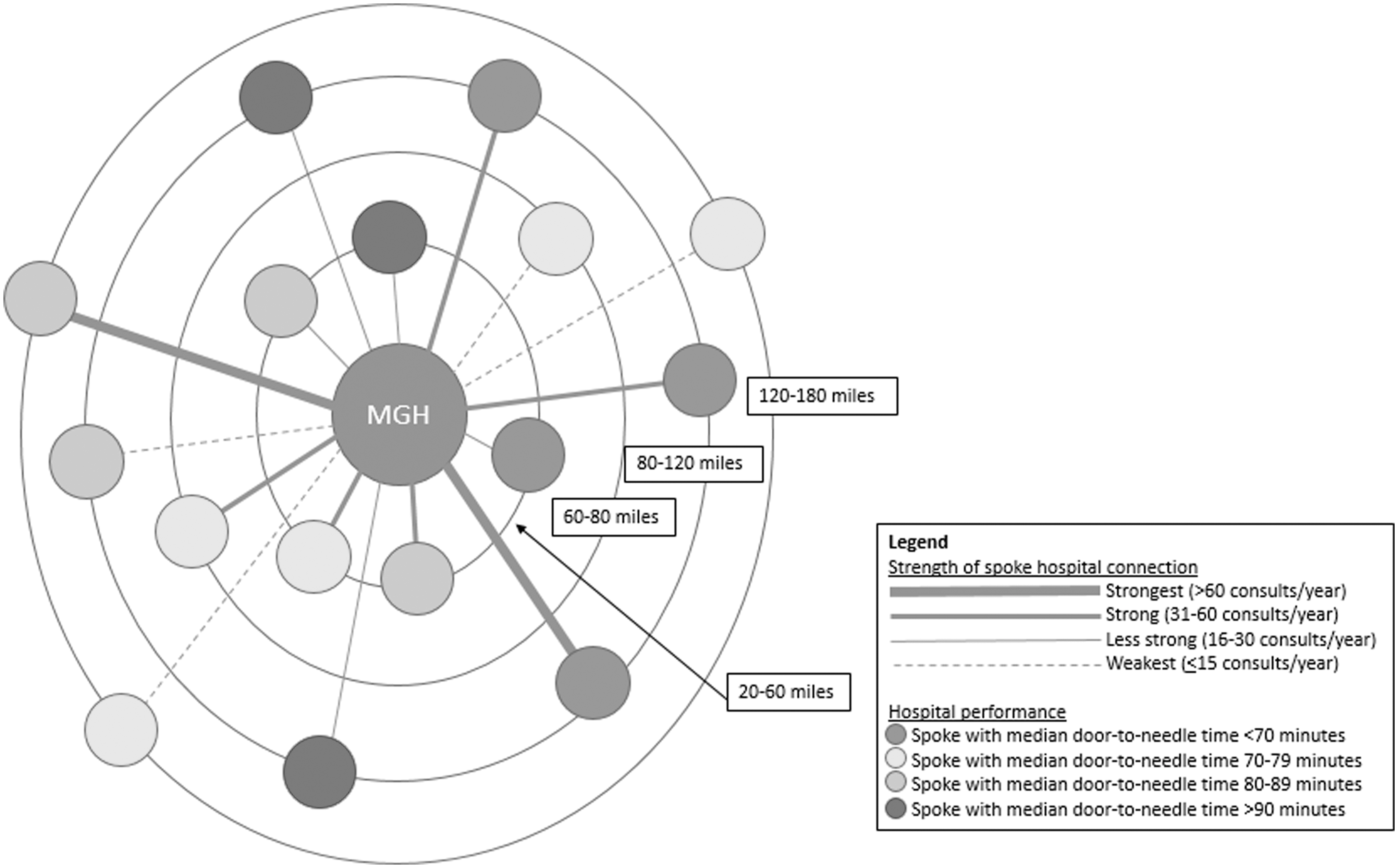
MGH Telestroke Network. The distance from MGH to each spoke hospital is represented by the ring on which the spoke hospital sits. The strength of the connection between MGH and each spoke hospital is represented by the weight of the line connecting the hospitals. The performance on tPA delivery for acute ischemic stroke patients at the spoke hospital is represented by the color of the spoke hospital (see Legend). MGH, Massachusetts General Hospital; tPA, tissue plasminogen activator.
Hospital Characteristics
Medical Center 7 contributed 1 year of data, therefore no IQR is reported, and no test for significance was completed for improvement over time.
Medical Center 8 contributed less than 2 full years of data, therefore no IQR is reported, and no test for significance was completed for improvement over time.
DTN, door-to-needle; IQR, interquartile range; tPA, tissue plasminogen activator.
Relationship Between Strength Of Spoke–MGH Connection and Patient DTN Times
Median patient-level DTN was 76 min (IQR 60–97) and improved over time (2 min faster per year, p = 0.02). After controlling for year of patient presentation, and clustering within hospitals, stronger spoke–hub connection was associated with faster patient DTN time (1.3 min faster per 10 additional spoke consults during year of patient's presentation, p = 0.048), (Fig. 2).
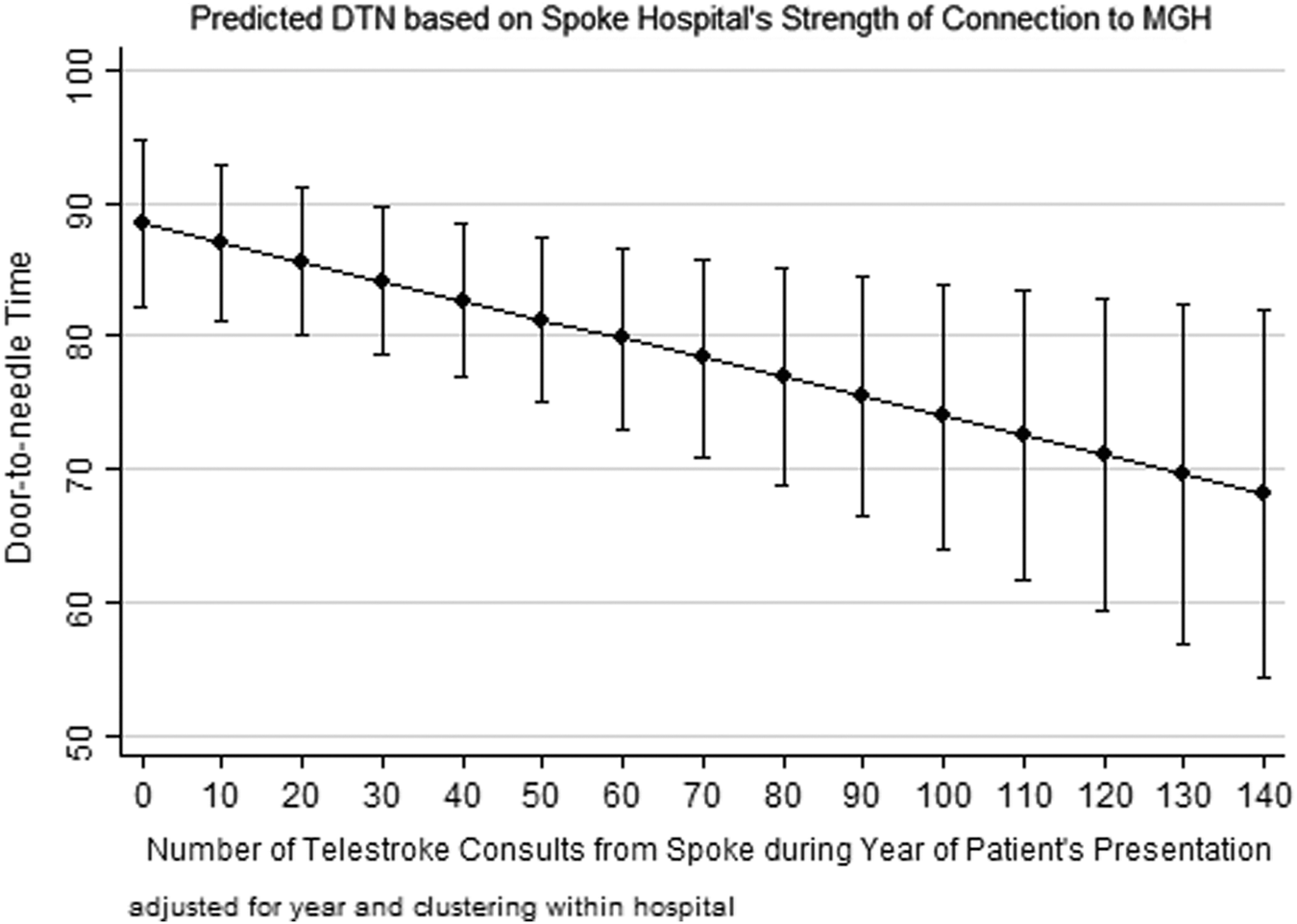
Predicted DTN based on strength of spoke–hub connection. DTN time for tPA treatment. Range: 3–137 consults per year. Predicted DTN by strength of spoke–hub connection. Predicted values based on model, holding other predictors constant. Scale bars indicate 95% confidence interval around predicted values. DTN, door-to-needle.
Discussion
In this analysis of an academic hub-and-spoke telestroke network, we found that spoke hospitals with higher intensity of connection to the hub hospital had better performance on AIS patient care delivery. That is, the more frequently a spoke hospital interacted with the hub hospital during the year of a patient's presentation, the faster the patient's predicted DTN time for tPA delivery. Importantly, this analysis included all tPA-treated patients presenting to spoke hospitals whether a telestroke consultation was acquired or not. We believe this reflects that much hospital performance improvement is in changing practice patterns rather than by individual case-by-case interventions.
Telestroke utilization has been tied to improved tPA delivery and to improved AIS patient outcomes. 10 –15 Likewise, in hepatitis C management, the Veterans Affairs Extension for Community Health Outcomes (ECHO) program has led to improved initiation of hepatitis C treatment among veterans 16 ; and in diabetes management, the Endo ECHO program evaluation will assess whether the telemedicine program improves outcomes for patients with complex diabetes. 17 However, we are not aware of any prior studies evaluating whether the intensity of a hospital's participation in a telemedicine network is correlated with improved performance or care delivery. Due to the relative paucity of randomized trials in the field, convincing evidence of benefit in telehealth applications is somewhat lacking. We sought to pursue this study in an effort to inform a randomized trial or large observational study with better adjustment for confounders. Follow-up work should examine this question in other telestroke networks and delivery models. If replicated, it will be important to study the nature of telestroke interactions between hub and spoke hospitals to better understand transmission of performance improvement between connected hospitals.
This study is limited as a retrospective, single-network study with a limited number of subjects; our findings may not be generalizable to other telestroke networks. Additionally, due to the nature of the blinded data, we were not able to determine which tPA-treated patients did or did not have a telestroke consultation. However, our hypothesis was that increased spoke–hub connection would lead to change on a system level rather than an individual level, and that all patients treated with tPA would benefit from a stronger spoke–hub connection, regardless whether telestroke was utilized for that particular patient encounter. Therefore, our inability to identify which patients did and did not have telestroke consultation does not impact the interpretation of our results. Finally, there may be other important confounders, such as spoke hospitals' stroke volume, which we were unable to include in our model. We view these results as hypothesis generating, and if confirmed, open an important avenue for future quality improvement work.
Conclusions
In our academic hub-and-spoke telestroke network, door-to-needle times for tPA delivery were faster for stroke patients presenting to spoke hospitals with stronger relationships to the hub hospital. This suggests that hub and spoke telestroke interactions may be a vehicle for knowledge transmission and performance improvement between connected hospitals.
Footnotes
Acknowledgments
The authors would like to thank the staff at the following hospitals for their study participation, data contribution, and ongoing collaboration: Bridgton Hospital, Central Maine Medical Center, Cooley Dickinson Hospital, Concord Hospital, Elliot Hospital, Exeter Hospital, Franklin Regional Hospital, Lakes Region General Hospital, Martha's Vineyard Hospital, Mercy Hospital, Nantucket Cottage Hospital, Rumford Hospital, Southern New Hampshire Medical Center, Carney Hospital, Wentworth Douglas Hospital, and York Hospital.
Financial support
Ms. Moreno's effort on this work was supported through the Massachusetts General Hospital Center for Diversity and Inclusion Summer Research Training Program (mentor Dr. K.S.Z.). Dr. K.S.Z. reports funding from AHRQ (K08HS024561) and the American Heart Association (16MCPRP27260221).
Author Contributions
K.S.Z. and L.H.S. conceived the study. K.A.S., A.V., C.W., and N.R. collected and managed the data. A.M., K.S.Z., and L.H.S. analyzed the data and all authors contributed to interpretation of results. A.M. drafted the article and all authors contributed substantially to its revision. K.S.Z. takes responsibility for the article as a whole.
Disclosure Statement
A.M., K.A.S., C.W., A.V., N.R., and K.S.Z. have no competing financial interests. L.H.S. has no direct conflicts of interest. L.H.S. reports being the principal investigator of an investigator-initiated study of extended-window intravenous thrombolysis funded by the National Institute of Neurological Disorders and Stroke (