
Abstract
Introduction
Treatment with vitamin K antagonist (VKA) is used for anticoagulation to either treat a thrombus or reduce the risk of developing a thrombus as in atrial fibrillation or mechanical heart valves. Although new oral anticoagulants are becoming more commonly prescribed, treatment with VKA, warfarin in particular, is still widespread and needs to be monitored. The traditional way of monitoring warfarin treatment for anticoagulation is by patient visits to the nearest hospital or general practitioner where a blood sample is taken and international normalized ratio (INR) is measured in a laboratory or point-of-care testing (POCT) system. The patient is given the result and the next daily warfarin scheme 3–4 weeks ahead (conventional management, CM).
Another treatment modality (patient self-testing [PST]) makes use of the patients using a POCT system at home and transferring the INR by phone or electronic means to a healthcare employee who decides on the next dosage and time for the next sample. Allowing patients to select their own dosage and time for the next sample is called patient self-management (PSM). Changing treatment modality from CM to PST and further to PSM could lead to fewer healthcare expenses and increased treatment quality through patient involvement; however, the decreased surveillance poses a potential problem in detecting the patients who are not able to take care of their own treatment.
As shown by McCahon et al., 1 online self-reporting of INR results in good data quality demonstrating a 99% agreement between self-reported INR results and source INR data and that online registries are feasible. Online reporting of INR and dosage would, therefore, be a way to surveil the quality of the treatment.
We have previously described the use of internet-based home management of anticoagulation based on PST using the CoaguChek XS system, reporting the INR value online to the physician who responds within a few hours, enabling the patient to access the reply online and print out the dosage scheme. We showed an increase in time in therapeutic range (TTR) from 72% to 79% using this system. 2 At the same time, the patients in a questionnaire reported 98% satisfaction (unpublished data) with this facility, allowing them to travel freely and having no need to go to the hospital or the general practitioner.
Patients using this system gained a deeper insight and understanding of the correlation between INR, dosage, and daily life style and interfering factors. Many patients expressed a wish to manage their dosing themselves and change to PSM.
Most previous studies comparing PST versus PSM found that PSM has a higher TTR than PST as reported in a review by Pozzi et al. 3 What distinguishes this study from previous studies is that the patients already have the experience in PST and, further they are used to having a real-time telecommunication to their anticoagulation clinic enabling the clinic to monitor the safety and quality of the treatment and also support on-demand and guide the patients if problems arise. Furthermore, the system will automatically raise an alarm and warn patients if quality limits are surpassed.
To ascertain how PSM could work in an online system, we performed this randomized controlled trial to investigate whether patients reached the same treatment quality as with treatment managed by healthcare employees.
Materials and Methods
Patients
Before the study started, a total of 302 patients were monitored using PST through telemedicine in our anticoagulation clinic. All these patients were considered for this study and all who fit the inclusion criteria but not the exclusion criteria were asked to participate in a randomized controlled trial before introducing PSM as a possibility in our clinic.
Inclusion criteria were: PST for a minimum of 6 months Accepts study participation and randomization Must be able to participate for the entire duration of the study Performs 1 month of PSM training Therapeutic INR range 2–3.
Exclusion criteria were: History of poor compliance or failure to report INR weekly.
Education
All patients who passed the criteria were invited to participate in patient education, which was held as a group seminar with up to 30 participants and lasted 2 h. The education material was produced locally in form of a presentation focusing on knowledge on VKAs and interacting factors; how to report dosage using the software CSO/AC; what kind of responses they could expect from the clinic; how to behave in case of fever, alcohol consumption, and change in medication other than warfarin. Several examples including INR–time plots were presented and questions were answered. Also all patients were informed to contact the clinic in case of any questions. After the seminar, the patients were invited to join the study. All who accepted participation gave written informed consent and were randomized into two groups. No specific examination was performed to ascertain the comprehension level of each patient, but all patients' actions were surveilled for 1 month after which patient actions were surveilled if certain criteria were met.
Randomization
All patients who accepted participation in this study were randomized into two groups. Randomization was performed using (
Intervention
Self-testing and medical decision on dosing versus self-testing and self-administered dosing (PST vs. PSM).
Patient Care
As a general rule, all patients measure INR once a week. Every weekday, one consultant checked CSO/AC for PST patients INRs and issued a warfarin dose to the patient, just as normal routine PST patients. The PSM patients were instructed to measure INR once weekly and at the same time note their next weekly dosage of warfarin; in case of any questions or problems they should phone or write a message in the CSO/AC. The PSM patients should then log in later to see a possible response from the healthcare worker. In the run-in period, the healthcare employee would check all INRs and dosages and write to/call the patient in case of unacceptable dosage. In the study period, the PSM patients would continue as in the run-in period. The healthcare employee, however, would only go through the patients if certain criteria were fulfilled, indicating no action from the patient or unacceptable treatment/large changes in dosage: INR <1.8 INR >4.5 Change in warfarin/week >1.25 mg Missing INR or dosage.
In these cases, the clinician would either contact the patient, change the dosage and write to the patient, or accept the dosage and write to the patient with advice. This constitutes an interaction in terms of outcome in this study.
Blood Analysis
Since all patients were used to PST, they all were introduced to sampling their own capillary blood for INR measurement. Once every year, each CoaguChek XS is controlled by patients sampling their capillary blood themselves and having a venous blood sample drawn for laboratory analysis. During the study period, patients produced their own INR results using the CoaguChek XS system (Roche Diagnostics, Indianapolis, IN).
Software
The CSO/AC (IntraMed A/S, Værløse, Denmark) is thoroughly described by Christensen et al. in 2011. 2 In short, the software system makes it possible for clinicians to manage treatment with VKAs for a large number of patients online. It is also possible for patients to login using the national common secure logon system for self-service in Denmark “NemID.” Patients can login and note the INR result from their CoaguChek XS. The physician can then see the result and note the new dosage to the patient. Finally, the patient receives the new dosage and date for the next INR measurement. The CSO/AC software system for management of VKA treatment is used by a single hospital in the United States, the majority of hospitals in Denmark, and as an internet-based tablet solution by nurses for home care.
Intervention Outcomes
TTR; number of INR events <1.8 and >4.5 and number of interactions by a healthcare professional.
Statistics
Sample size was determined at 31 in each group at power 80% and a hypothetical increase in TTR of 5% in the PSM group.
We used the statistical tests of Fisher's exact test, Kruskal–Wallis test, and chi–squared test, and a p-value of 0.05 was used as threshold. The statistical package Stata v.14 (StataCorp LLC, College Station, TX) was used.
Ethics and Data
This study was approved by The Regional Committees on Health Research Ethics for Southern Denmark project number S20133011, and all patients gave written informed consent to participate in the study.
Results
Owing to inclusion and exclusion criteria, 302 patients were reduced to 159 patients who were invited to participate in the study. A total of 106 patients accepted to participate in an education seminar after which 87 patients accepted study participation and were randomized to a PSM study group (n = 44) or a PST control group (n = 43) as shown in Figure 1. There were more men (79.3%) than women (20.7%) in the study and the same difference was seen in all patients invited to participate in the study (women: 20.1%). Average age in the study was 69.4 years and we found no difference in age across the two study groups.
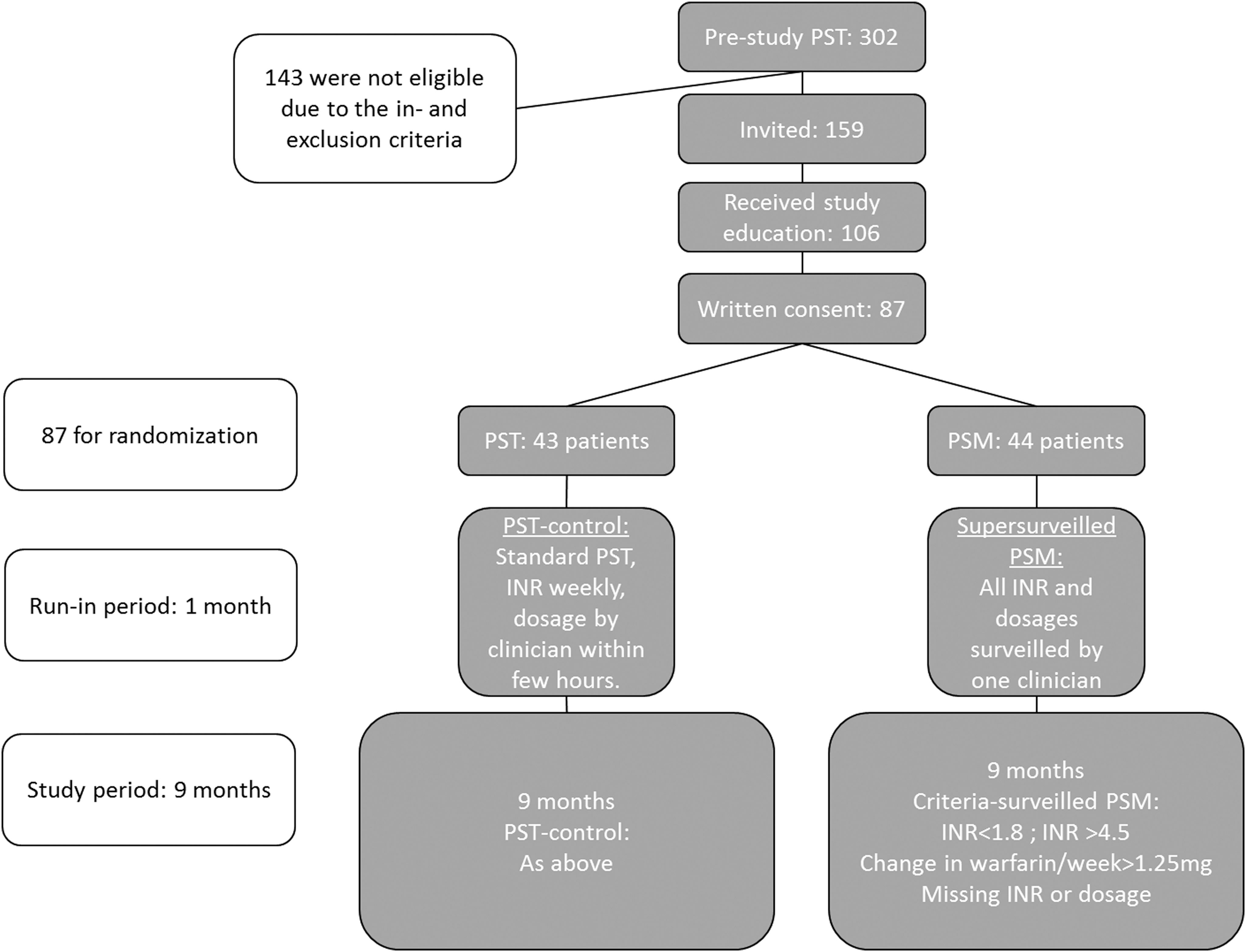
Patient flow from total initial cohort to finished study period. The figure shows which criteria were applied in each group in both run-in period and the study period. PSM, patient self-management; PST, patient self-testing.
Three patients (3.4%) left the study, one patient was changed to a new oral anticoagulant (NOAC), one patient was excluded due to patient preference, and one patient was excluded due to initiation of examination for Alzheimer's disease. A total of 84 patients completed the study. Figure 2 shows the fraction of samples in therapeutic range and average INR for the run-in period as well as for each week in the study period. No difference in average INR or fraction of INR in therapeutic range was observed in the two study groups.
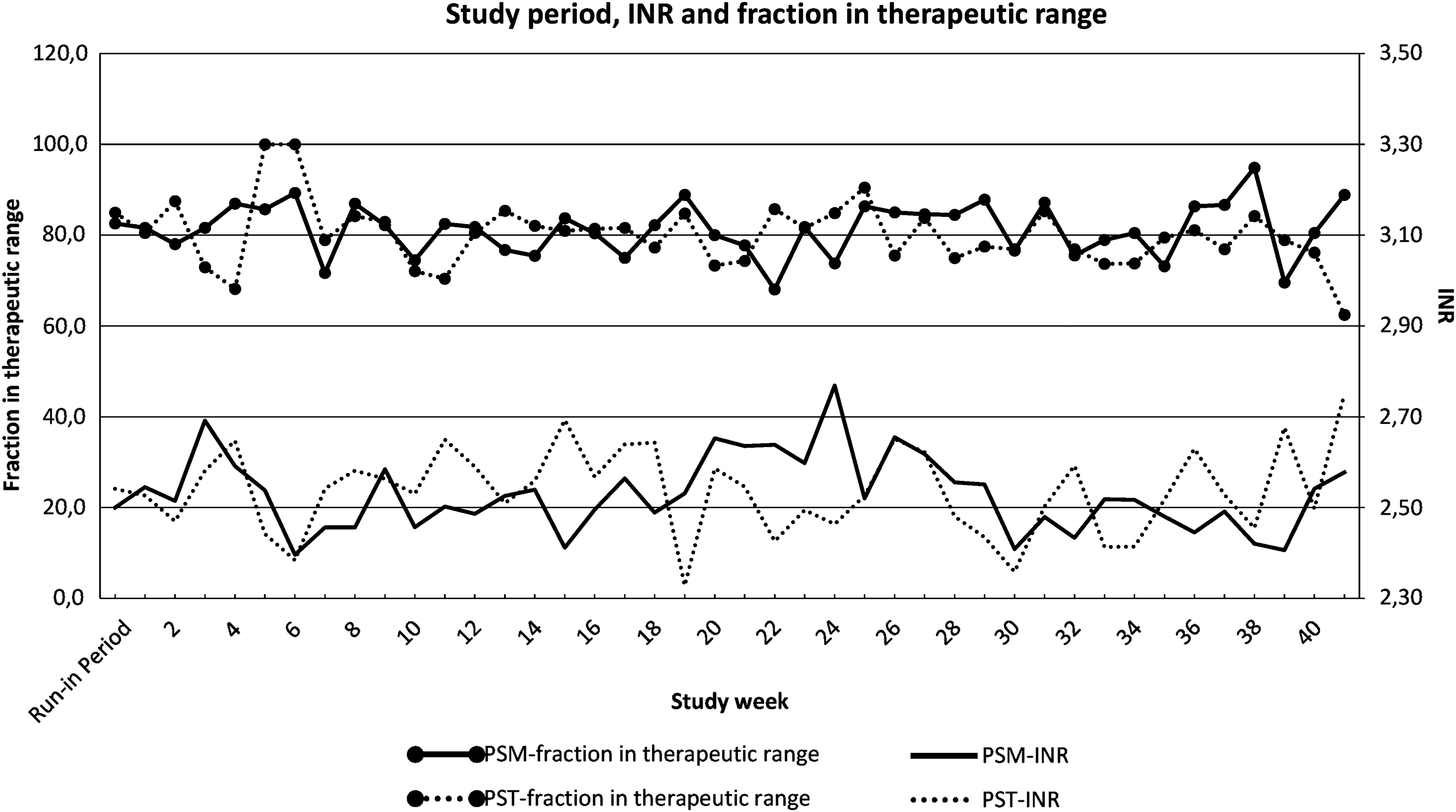
Shows fraction of samples in therapeutic range for each week at the top and average INR at the bottom. The run-in period is shown to the far left. INR, international normalized ratio.
Basic characteristics as well as results concerning TTR and outcomes are given in Table 1. No statistical differences were observed between the two groups in terms of fraction of samples in therapeutic range or values seriously out of therapeutic range (INR <1.8; INR >4.5).
Basic Characteristics
INR, international normalized ratio; PSM, patient self-management; PST, patient self-testing; SD, standard deviation; TTR, time in therapeutic range.
The average number of interactions performed by healthcare professionals per month for each group showed a highly significant difference (p < 0.00001) between the two study groups as given in Table 2.
Data Summary of Study Results and the Anticoagulation Clinic
CM, conventional management.
To investigate the change in workload for healthcare professionals due to a change in the method used to manage patients in VKA treatment, we compared the number of interactions needed as given in Table 2. Using our anticoagulation clinic as an example, VKA treatment using CM requires 1.6 blood samples on average per month equals 1.6 healthcare professional interactions per month. Changing to PST with a standard of one blood sample per week, the number of blood samples and hence, interactions, increase to 4.2 per month. Changing from PST to PSM requires the same number of blood samples but decreases the number of healthcare interactions to 1.1 per month because only the criteria-sorted instances require an interaction.
All patients were encouraged to inform the clinic should any changes happen in bleeding tendency or treatment hereof. No bleeding occurred in either group. No patients died during the study period.
Discussion
In this randomized controlled trial, we show that patients using PSM reached the same treatment quality as with treatment managed by healthcare employees.
Approximately half of the patients using PST were eligible for PSM using our criteria. This fraction is highly dependent on the criteria for patients in an anticoagulation clinic and the criteria for using PST in the first place. Two-thirds of the patients invited to participate in an education seminar accepted this. More than 80% accepted to participate in the study.
A total of three patients were excluded from the study during the study period due to acceptable reasons and the dropout rate is low (3.4%) during the 10 months study period compared with other studies of PSM, for example, 9.8% for 12 months as reported by Ward et al. 4 All patient dropouts were in the PSM group, but with the low number of dropouts in total, the difference between the groups is very low and acceptable.
The gender distribution was the same in the two groups although there were more men than women. This difference was also seen in the group invited to participate in the study, so there was no gender difference in terms of likelihood to participate in the study. A large gender difference in use of PSM in VKA treatment has previously been reported by Nagler et al. 5
The difference in gender could be due to several factors. In general, more men than women use VKA treatment (national use of VKA in Denmark in 2016 was 64% vs. 36% according to
The two groups performed equally in terms of fraction of INR in the therapeutic range as well as average INR.
Patients tend to want to stay in the lower end of the therapeutic range. During the education of the patients, they were specifically taught to be in the range and not try to end up in the lower range. The PSM group did not change in fraction of INR in the therapeutic range as well as average INR over time as might happen due to patient preferences toward the lower end of the therapeutic range.
We observed no statistical differences between the two groups in terms of fraction of samples in therapeutic range or values seriously out of therapeutic range (INR <1.8; INR >4.5). No deaths occurred in either group during the study. Patients were taught to report any change in bleeding tendency. No bleeding requiring hospital treatment was reported in either group during the study. Therefore, PSM seems safe compared with PST.
As given in Table 2, the TTR increases along with the change CM→PST→PSM while the number of interactions decrease, so the increase in the quality of the treatment is accompanied by a decrease in healthcare workload. The transition to PSM is, therefore, associated with fewer expenses to healthcare providers in terms of reduced time for dosing but also reduced number of blood samples (compared with CM) and, therefore, reduced requirements for capacity and waiting time in the outpatient clinic. The advantages to the patients will be larger awareness and understanding of their own treatment as well as a more flexible system, allowing for time away from the computer and the hospital. The number of healthcare interactions in PSM is depended on the criteria used, less strict criteria may prove equally safe, which would result in a further reduced number of healthcare interactions in PSM and even bigger advantage in using PSM.
The disadvantages are in terms of securing that patient treatment is of continued high quality. The criteria used in this study for daily treatment handling were efficient although the quality of monitoring is only as good as the data put into the system. 1 We used 1 month of super surveillance to teach and test the patients. A way to improve this could be to conduct an examination for the patients starting PSM to ensure their understanding as used by Jenner et al. 6 In our clinic, we conduct an outpatient visit in the hospital every year to ensure that the patient treatment is running smoothly, that all patient questions are answered, and that the CoaguChek is controlled against the laboratory standard INR. We would recommend conducting similar control also to detect serious mental illness as Alzheimer's disease. In this study, all patients were used to PST at inclusion to the study. In case PSM should be offered to patients just starting VKA treatment or patients used to CM, a thorough introduction to the POCT and the telemedicine solution should be utilized to ensure proper patient handling and results. In particular, extra care should be given to older patients not used to computers or online services, but also difficulties in terms of eyesight, finger dexterity, and mental state should be acknowledged.
With the introduction of newer anticoagulants, the use for warfarin is reducing, but as long as warfarin is used, monitoring is necessary and PSM is a good solution for patients who can manage this.
To our knowledge, this is the first study to perform a randomized controlled trial on the feasibility of using an online secure system to supervise patient care in VKA treatment.
Limitations of this study are, in part, due to the low number of patients allowing only for severe differences in outcome measurements. There are more men than women in the study cohort, but the number of participants do not allow for investigating any gender difference in performance in treatment as found by Nilsson et al. 7
Based on this randomized controlled trial, the PSM is now being offered as a general utility to patients at our hospital. With PSM set up like we have shown and with an examination after education, we believe that most patients in an anticoagulation clinic can be handled either by PSM, NOAC, or a small group of patients on CM/PST.
We conclude that patients accustomed to PST using telemedicine can easily be transferred to PSM using a computer support system with the same quality of treatment as measured in TTR and number of measurements outside critical limits. This can also result in reduced healthcare expenses due to a reduced number of interactions by healthcare employees and hence less time-consuming treatment monitoring.
Footnotes
Acknowledgment
We thank laboratory technician Hanne Leth Laursen for her help running the anticoagulation clinic.
Disclosure Statement
No competing financial interests exist.