
Abstract
Background:
Emergency department (ED)-based telemedicine has been implemented in many rural hospitals to provide specialty care and expertise to patients with critical time-sensitive conditions.
Introduction:
The purpose of this study was to measure the impact of ED-based telemedicine on timeliness of care in participating rural hospitals.
Materials and Methods:
Matched cohort study of patients seen in 1 of 14 rural hospitals in a large Midwestern telemedicine network. Telemedicine cases were matched 2:1 with controls based on age, diagnosis, and hospital. The primary outcome was door-to-provider time, and secondary outcomes included ED length-of-stay (LOS) and time-to-transfer in those transferred to other hospitals.
Results:
Of 127,928 qualifying ED encounters, 2,857 consulted telemedicine and were matched with nontelemedicine controls. Door-to-provider time was shorter in telemedicine patients by 6.0 min (95% confidence interval [CI] 4.3–7.8 min). The first provider seeing the patient was a telemedicine provider in 41.7% of telemedicine encounters, and in these cases, telemedicine was 14.7 min earlier than local providers. ED LOS was 22.1 min shorter (95% CI 3.1–41.2) among transferred patients, but total ED LOS was longer (40.2 min, 95% CI 30.8–49.6 min) for all telemedicine patients.
Conclusions:
Telemedicine decreases ED door-to-provider time, most commonly because the telemedicine provider was the first provider seeing a patient. Among transferred patients, ED LOS at the first hospital was shorter in patients who had telemedicine consulted. Future work will focus on the clinical impact of more timely rural ED care.
Introduction
Providing rapid, high-quality emergency care for patients with time-sensitive conditions drove the development of dedicated emergency departments (EDs) in the late 1960s. 1 Since that time, many conditions have been shown to benefit from rapid diagnostics and treatment interventions, including trauma, myocardial infarction, stroke, and sepsis. 2 –7 Increasingly, patients with these conditions have also shown to fare better in high-volume hospitals that manage these conditions frequently, leading to the development of elaborate transfer networks to drive regionalization initiatives. 8 –14
Providing rapid high-quality care has been difficult in some rural hospitals, however. Staffing challenges, the infrequency with which time-sensitive conditions are managed, and resource limitations all make timely care hard to achieve. Furthermore, many remote and frontier hospitals may not have a provider in the hospital around-the-clock, leading to delays while a provider covering the ED drives to the hospital. 15 –17 Telemedicine has been seen as one potential solution to improve both the timeliness and quality of rural emergency care, and many rural hospitals have subscribed to telemedicine networks to augment the emergency care that they already provide. 18 –20
The objective of this study was to measure the impact of ED-based telemedicine services on door-to-provider time in a single telemedicine network in the upper Midwest. Secondary objectives were to estimate the effect on ED length-of-stay (LOS) and time-to-transfer. We hypothesized that telemedicine would decrease the time-to-provider, especially in the most rural hospitals without in-house emergency providers. We also expected that telemedicine use would decrease the time-to-transfer in patients requiring interhospital transfer, likely through coordinating transfer with the receiving facility and transferring ambulance services.
Materials and Methods
Study Design, Setting, and Population
This study was an observational cohort study of all ED patients treated in a network of critical access hospitals subscribing to telemedicine services from a single ED-based telemedicine provider (Avera eCARE, Sioux Falls, SD) from 2007 to 2015. Because telemedicine services were implemented on different dates for each hospital, the data set included only hospitals with data available for periods before implementation and after implementation. Critical access hospitals are federally qualified as rural hospitals with 25 beds or fewer that are located remotely from other hospitals and from which 24-h emergency services are required under a set of Medicare Conditions of Participation for Hospitals. 21 Hospitals selected for inclusion in this study included 14 hospitals in Iowa, Kansas, Nebraska, North Dakota, and South Dakota that comprise a subset of the entire network of hospitals with data available in an electronic medical record for the study period, and for whom data sharing agreements already existed for clinical operations. The primary exposure of interest was use of telemedicine. This study was approved under waiver of informed consent by the local institutional review board and is reported according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 22
Records were excluded for missing times of care or if the hospital had no data available for patients before telemedicine implementation. Because missing data elements were different for each analysis, the sample size is slightly different. Telemedicine use was defined retrospectively as an ED encounter that was also present in the telemedicine call log, matched on name, date and time of encounter, and facility. Telemedicine availability was defined as an ED encounter at a hospital with active telemedicine service on the date of the encounter. Records with an ED encounter in the month of telemedicine implementation were excluded because assigning whether telemedicine was available on the date of encounter was challenging during the implementation period.
ED-Based Telemedicine Service
The telemedicine network evaluated in this report is a 146-hospital ED-based network organized in a hub-and-spoke model. The hub, located in Sioux Falls, SD, provides dedicated 24-h real-time high-definition video telemedicine connectivity, predominantly to facilities in the upper Midwest. Telemedicine consultation is requested by rural providers by pressing a button on the wall, and connects a rural ED to a board-certified emergency physician and experienced ED nurse in the hub facility. Hub staff are available to help with nursing documentation, arrange interhospital transfer, and provide medical advice as requested by rural hospital staff. Rural providers and nurses are trained on the use of telemedicine equipment at the time of hospital implementation, and consultation can be requested for any patient complaint, although the network has focused quality improvement activities on trauma, cardiac, and stroke care.
Key Outcomes and Definitions
The primary outcome was time-to-provider, defined as the time interval from ED registration to contact by a licensed independent practitioner (either a physician or an advanced practice provider). This provider could be either a local provider or a telemedicine provider—whoever was available first. Local provider contact was defined as a provider personally physically assessing a patient as recorded in the electronic medical record (which was felt to accurately reflect contact in low-volume rural hospitals), and telemedicine contact was defined as the earliest time that a functional telemedicine video conference connection was established with the hub staff and rural ED. Secondary outcomes included ED LOS, time-to-transfer, and proportion of patients transferred. ED LOS was defined as the time interval from ED registration until ED discharge and was stratified by transfer status. Interhospital transfer was defined as moving a patient from the treating ED to another acute care hospital, usually by ambulance or helicopter, and was assessed using the administrative ED discharge disposition of “Transfer.” “Nontransfers” were defined as an ED discharge disposition of routine discharge, admitted to local inpatient facility, died, or other (e.g., discharged to skilled nursing).
Patient diagnoses were grouped using the Clinical Classification Software (CCS) categorization on primary diagnosis code (International Classification of Diseases, 9th edition, ICD-9), available from the Health Care Utilization Project (HCUP) funded by the Agency for Healthcare Research and Quality (AHRQ). 12 The CCS algorithm groups ICD-9 codes into a four-level hierarchical schema to designate increasing levels of specificity, with level 1 categories being most general (e.g., cardiovascular) and level 4 codes being most specific (e.g., myocardial infarction).
Data Management
Patients were excluded if the ED LOS exceeded 24 h or if the door-to-provider time was less than 60 min (note that negative door-to-provider times were recorded when telemedicine was activated based on ambulance reports before patient arrival) or greater than 12 h, to eliminate patients with times that were likely recorded incorrectly. All negative door-to-provider times were defaulted to zero time, since the magnitude of negative time was irrelevant in the interpretation of the final analysis.
Data Analysis
Univariate comparisons were used to identify demographic and care-associated factors that were associated with telemedicine availability and use. Continuous variables were compared by the Wilcoxon rank-sum test, since the data were not normally distributed. Categorical variables were compared with chi-square tests.
The primary outcome was analyzed using a matched cohort, matched on diagnosis category, age category, and presenting hospital. Cases were matched 2:1 with controls to account for the low consultation rate and to limit the effect of endogeneity. Variables included in the matching algorithm were selected a priori based on theory alone. Because of large perceived differences in urgency of care and diagnostic strategy based on chief complaint and diagnosis, the CCS diagnosis group was included as a categorical matching variable. Once the CCS algorithm was applied, many ICD-9 codes did not map to level 3 or level 4 CCS categories, so level 2 CCS categories were used in the algorithm. Age was also included as a categorical covariate, stratified into age categories (<65, 65–74, 75–84, 85+), similarly because the diagnostic strategy was thought to vary based on age. Both of these predictors were also associated with telemedicine use in univariate comparisons. Inclusion of hospital was done to control for immeasurable confounders that relate to efficiency and institutional practice variation.
The primary analysis was conducted using conditional linear regression, to adjust for matching in the final cohort selection. Because time-to-provider was right-skewed, the residual error terms in linear modeling were not normally distributed, violating an assumption of linear regression. We determined a priori that time data would be log transformed for analysis, as previously reported in similar analyses. 20 If relationships were significant in both the linear and log-transformed models, we report the results of linear models, because of the ease of interpreting linear coefficients.
Both telemedicine availability and telemedicine use were included as exposures of interest in the final model. In our previous work, we have shown that telemedicine availability and telemedicine use function as independent variables, partly because the rate of telemedicine consultation is low across all diagnostic groups. We also have observed that care changes in fixed-effects modeling when telemedicine is implemented, perhaps due to hospital relationships, changes in care processes, or a clinician learning effect. 20 This strategy allowed the research team to elucidate the effect of telemedicine availability independent of use to understand how the telemedicine relationship changed care efficiency, even without telemedicine activation. Secondary outcomes of ED LOS and time-to transfer were modeled using a similar modeling approach.
Because all available data were used in the analysis, no sample size calculation was conducted a priori. All hypotheses are tested using two-tailed tests with α < 0.05 used to define statistical significance, and analyses were conducted using SAS version 9.4 (SAS Institute, Cary, NC). All authors had full access to the analytic data set and independently controlled the decision to publish.
Results
Between November 2007 and August 2015, 164,884 unique patient visits were seen in participating EDs, of which 127,928 were included in the final cohort for analysis (22% excluded for missing time or pretelemedicine implementation data) and 2,857 (3.5% of telemedicine-available encounters) consulted telemedicine (Fig. 1). Among all patients in the cohort, the most prevalent diagnosis categories were circulatory diseases (29%) and injuries or poisoning (25%), and 2,010 (24%) were transferred. After matching, 8,694 (4,716 records in earliest door-to-provider cohort and 5,385 records in the ED LOS cohort) unique records remained, and significant differences in demographics and diagnostic categories existed by telemedicine use (Table 1).
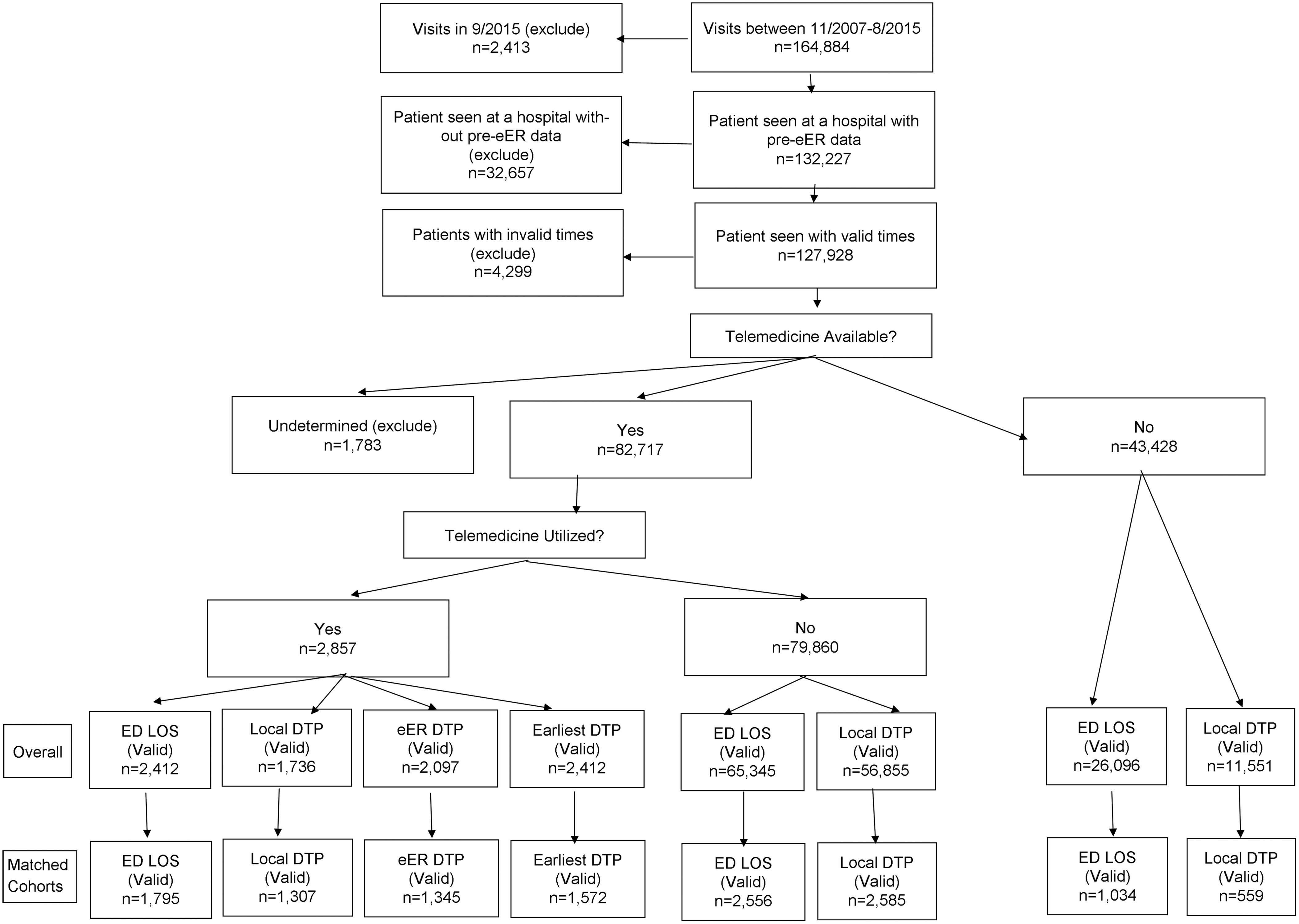
Flow diagram of study records.
Demographic and Emergency Department Care Characteristics of Patients, Stratified by Telemedicine Availability and Use
To protect the confidentiality of individual cases, counts that are 5 or fewer have been suppressed.
CCS, Clinical Classification Software; DTP, door-to-provider; ED, emergency department; LOS, length-of-stay.
Time-to-Provider
Overall, the door-to-provider time in the matched cohort was 7.0 min (IQR 1–18) in cases that used telemedicine versus 15.0 min (IQR 7–28) in those where telemedicine was not consulted (Table 1). Of the telemedicine consulting cases, 41.7% had the earliest provider recorded as the telemedicine provider and of these, the telemedicine physician was available a mean of 14.7 min sooner than the local provider. In regression modeling, the log-transformed model showed that door-to-provider time was shorter when telemedicine was activated, but not when telemedicine was available and not activated. Using a conditional linear model, door-to-provider time was 6.0 min faster (95% confidence interval [CI] 4.3–7.8 min) when telemedicine was consulted (Table 2). The effect size was heterogeneous across the hospitals included in the analysis, as the overall median door-to-provider time varied by hospital (Fig. 2).
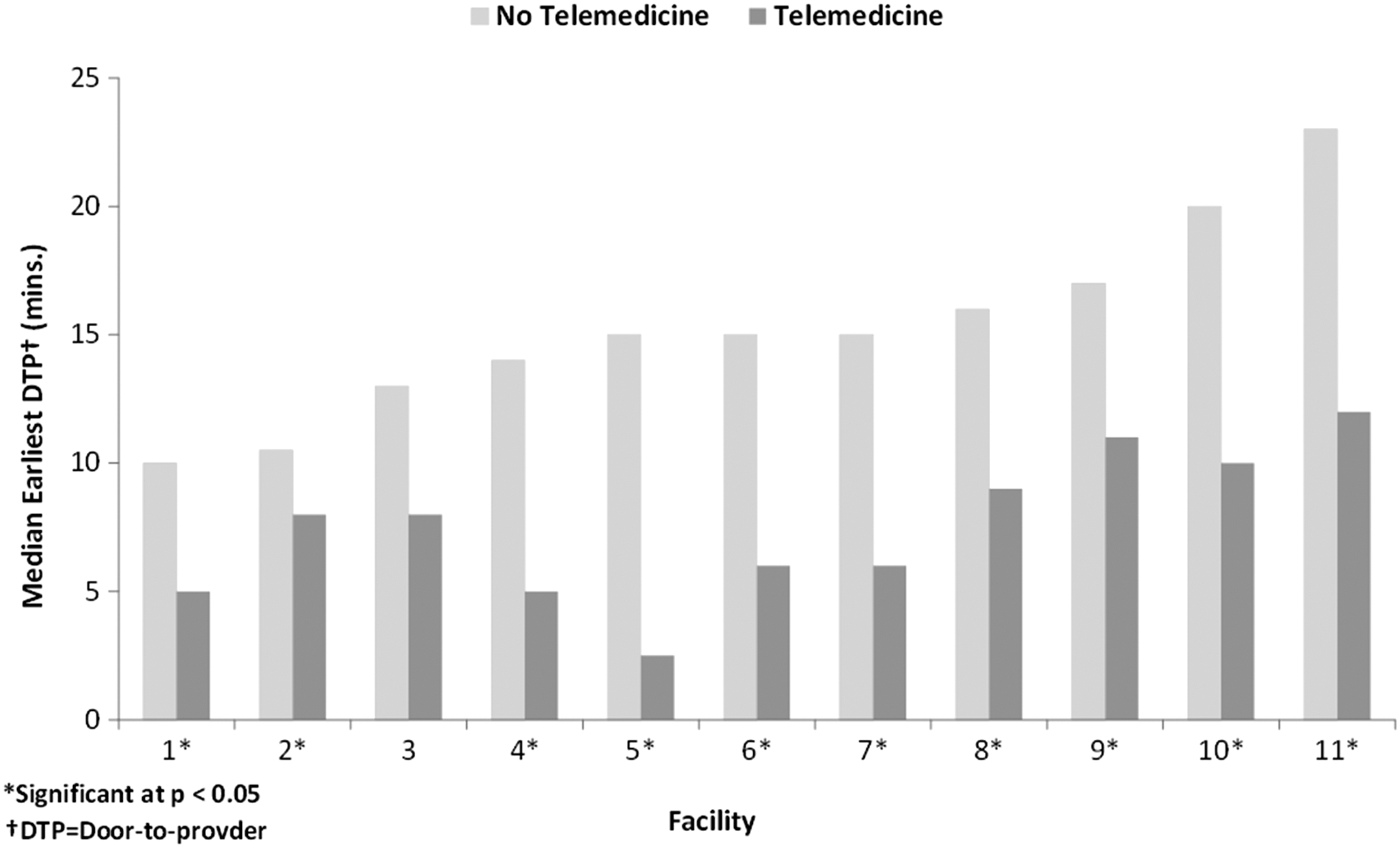
Variation in door-to-provider time by facility. Dark gray bars show the median hospital-specific door-to-provider time in cases where telemedicine is consulted, and light gray bars show the median hospital-specific door-to-provider time in cases where telemedicine was not consulted. Hospitals are arranged in the order of their non-telemedicine door-to-provider time.
Association of Telemedicine with Earliest Door-To-Provider Time and Emergency Department Length-Of-Stay
Controlling for age and primary diagnosis group CCS, and clustering on hospital.
A constant of 61 was added to all DTP and LOS times to allow for log transformation of zeros.
CI, confidence interval.
ED Length-of-Stay
The ED LOS in the matched cohort was higher in patients where telemedicine was utilized than in those where telemedicine was not utilized (median 115 vs. 89 min, p < 0.0001). In regression modeling, the log-transformed overall LOS was longer, so a linear model was constructed and showed that the overall LOS was about 40.2 min longer (95% CI 30.8–49.6 min) in patients where telemedicine was used. When stratified by transfer status, however, transferred patients receiving telemedicine before transfer had a 22.1 min shorter ED LOS (p = 0.023), while nontransferred patients had an 80.2 min longer ED LOS (p < 0.0001). Furthermore, the differences in LOS differed significantly by CCS diagnosis groups, and the differences between transfers and nontransfers differed by CCS as well (Fig. 3). ED LOS was unrelated to the timeliness of consultation or the duration of the telemedicine encounter.
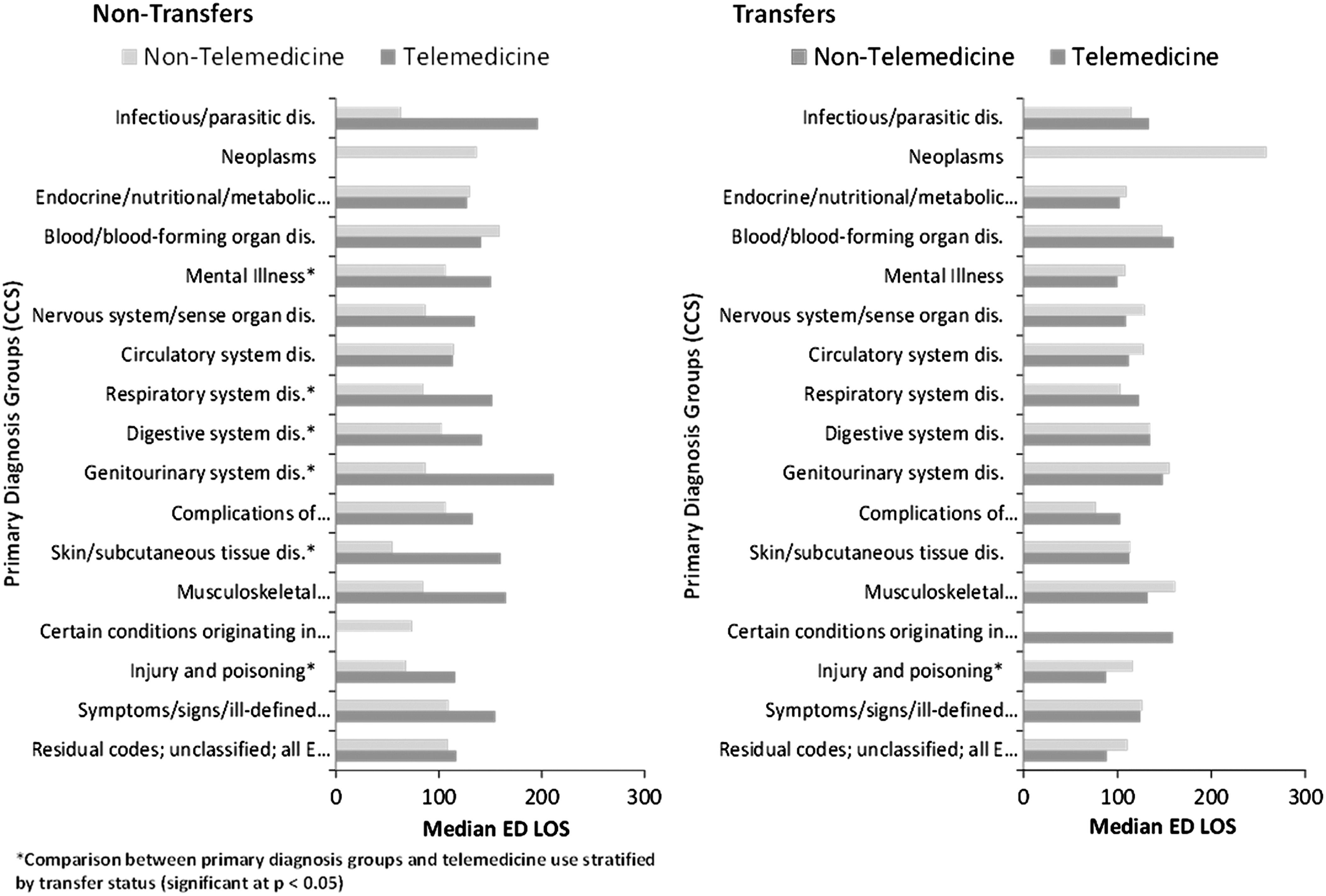
Median ED LOS stratified by CCS Level I diagnosis codes. Dark gray bars show the median nontransfer ED LOS, and light gray bars show the median ED LOS among transferred patients. CCS, Clinical Classification Software; ED, emergency department; LOS, length-of-stay.
Discussion
Although several prior studies have reported the effect of telemedicine on timeliness of emergency care, most have either focused on small diagnostic subgroups, limited telemedicine capabilities, or small-scale feasibility analyses with limited statistical power. 20,23 –27 This report is the first to establish the impact of telemedicine consultation on timeliness of care in a large cohort of patients treating in rural hospital EDs. Telemedicine is appealing as a strategy to augment local emergency services, but the aggregate impact of telemedicine on throughput and timeliness of recommendations across a range of diagnoses is unknown. Furthermore, quantifying the impact of telemedicine on heterogeneous hospitals is important to predicting how health systems might adapt in new telemedicine installations and which patients benefit most from the timely care that telemedicine provides. These questions continue to be relevant, especially in an era of changing legislative action with regard to telemedicine implementation, utilization, and reimbursement.
Telemedicine may impact timeliness of care through several pathways. First and most obvious, telemedicine can provide a rapid response capability in remote and frontier hospitals with no in-house emergency physician. In these cases, therapy can be ordered by telemedicine providers even before local providers arrive in the hospital. Second, telemedicine may provide surge capacity in busy rural EDs when a provider is caring for other competing patients. While many rural facilities do not often have full waiting rooms, local events may quickly overwhelm available resources. For instance, motor vehicle crashes with multiple victims may stretch a provider in a typically low-volume hospital to deliver simultaneous care to multiple critically injured patients. Finally, telemedicine providers may be able to help risk stratify patients during times of high volume—conducting triage in parallel with the local emergency provider to help allocate limited resources. In many cases, telemedicine providers can be activated based on ambulance reports and can help to organize the care team and prepare equipment to improve the ability for a timely response on patient arrival.
The most striking finding of our report is the decreased ED LOS in patients who are transferred to other hospitals. This finding is similar to a prior report of timeliness of transfer in trauma patients, but this report shows that the finding applies even in less selected patients. 20 In patients for whom telemedicine is activated, hub staff can arrange for interhospital transfer by talking with an accepting clinician, arranging for ambulance or helicopter evacuation, and other administrative tasks of transfer in parallel with the actual medical care that the local clinician is providing or before the local clinicians arrival. Hub nursing staff can also off-load charting responsibilities from local nursing staff, returning frontline medical staff to patient care. Both of these activities can significantly improve the efficiency of local staff, and we have found that this capability can achieve more rapid transfer among patients sent to tertiary centers.
However, is care timeliness the right outcome? For specific diseases (e.g., stroke, myocardial infarction, sepsis, and trauma), specific timely interventions have been shown to change long-term outcomes. 2 –7 For instance, starting appropriate antibiotics earlier for patients with pneumonia or sepsis can translate to lower in-hospital mortality, 28,29 and transferring myocardial infarction patients to a percutaneous coronary intervention-capable center quickly can improve disability-free survival. 10 For patients being transferred due to trauma or stroke intervention, reducing the rural LOS by 22 min may speed the availability of life-saving interventions available only in tertiary hospitals.
Does improving timeliness for transferred patients come at a cost, though? Although the LOS was shorter for transferred patients, it was longer for patients not transferred. This finding is interesting because it suggests that for patients who stay in local hospitals, consulting the telemedicine provider may add additional tasks that complicate and lengthen the ED encounter. 20 If these are patients who would have been transferred without telemedicine, additional time expenditure may simply reflect care previously received at tertiary centers. Additional tasks that improve the quality of care may be justified, but it may also be an unintended consequence of rural telemedicine use. In addition, some of this effect may be residual confounding from more complicated patients receiving telemedicine consultation.
Our study has several limitations. First, this study was conducted retrospectively using medical records data. While that method provided a large number of cases, it also limits our analysis to data contained in medical records. For instance, we are not able to adjust adequately for severity of illness or diagnostic strategies, which could be a significant confounder not adjusted in our matching algorithm or statistical models. Second, this analysis includes a wide variety of diagnoses. We have used our matching algorithm to limit the variation in our control group, but heterogeneous treatment effects are difficult to define with many diagnoses in many hospitals. Finally, patients who had telemedicine consulted remain different from those who did not. 30
In conclusion, telemedicine decreases the door-to-provider time in rural hospitals with telemedicine services by 6 min. ED LOS is also more than 20 min shorter among patients transferred to tertiary centers for ongoing care, but the LOS for nontransferred patients seems to be increased. Future work should focus on the impact of telemedicine-augmented emergency care on patient-centered quality of care, clinical outcomes, and provider retention in rural hospitals.
Footnotes
Acknowledgments
This project was supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) under grant G01RH27868 entitled Evidence-Based Tele-Emergency Network Grant Program and grant number 6 UICRH29074-01-01 entitled Telehealth-Focused Rural Health Research Center. This content and conclusions are those of the authors and should not be construed as the official position or policy of, nor should any endorsements be inferred by, the HRSA, HHS or the U.S. Government. The authors acknowledge Werner Berg, Katie Moore, Shiann Shipp, and Luke Mack for their help with data preparation, study planning, and analysis. This analysis was conducted by the Rural Telehealth Research Center at the University of Iowa.
Disclosure Statement
B.S., A.W., and A.B., are employed by the Avera eCARE, which provides emergency department-based telemedicine services. None of the other authors has any competing financial interests to report.