
Abstract
Introduction
Many Americans encounter severe barriers to accessing necessary healthcare services. 1,2 Beyond barriers related to cost and insurance status, there are many reasons that patients cannot access their regular provider or other healthcare when needed. These barriers can include lack of available appointment times, care needs occurring at off hours, and providers that are located too far away or are difficult to access. 1 In addition, nearly 20% of respondents in a recent survey stated they would not be able to access the best healthcare in the state if they became seriously ill. 1
Telehealth is a promising approach to improving healthcare access and quality. 2 –4 Telehealth utilizes health information and telecommunications technology to provide patient care, where the provider and patient can be separated by distance or time. 5 Telehealth can include real-time video visits, remote patient monitoring, and asynchronous communication or sharing of still images for diagnosis and treatment. 6 These technologies are promoted as a convenient way to increase access to specialty and primary care to patients while reducing barriers such as travel time and transportation costs to the academic or specialty setting. 2
Coverage for telehealthcare has expanded over the last two decades. Medicare began reimbursing for telehealth services in 1997, 7 yet reimbursement remains one of the biggest barriers to provider adoption of telehealth. 8 –11 Forty-eight states and the District of Columbia's Medicaid programs now cover at least some telehealth services. However, the regulations and reimbursement for telehealth varies considerably by state. 2,12 In many cases, reimbursement only covers real-time video visits. Telehealth services, such as home monitoring of chronic disease, are covered by 22 state Medicaid programs, and asynchronous communication and store-and-forward of diagnostic information are reimbursable in 13 state Medicaid programs. 2,6,12 In addition, 26 state employee health plans provide some telehealth coverage. 6
Adopting reimbursement policy interventions may be one approach to improving access to telehealth services. According to a 2015 survey, 55% of nontelehealth providers and 43% of telehealth providers cited reimbursement by insurers as a barrier to using telehealth. 9 Studies have signaled that reimbursement legislation can promote the adoption of telehealth technology. Under Medicare legislation, telehealth visits have annually increased by 28% per year since 2004. 10 Prior research has shown an increase in telehealth utilization related to reimbursement changes regardless of payer type. A study of six states in the Great Lakes region found that reimbursement policy changes for Medicaid coincided with significant increases in Medicare beneficiary telehealth visits. 7 Another study of Medicare beneficiaries found increased utilization of telehealth services for those living in states that passed private insurance telehealth parity legislation. It is believed that reimbursement changes for one payer type may indirectly increase utilization of telehealth services for other patient populations as providers are not rationing the use of telehealth services based on payer type. Additionally, as the number and types of reimbursable telehealth services increase, there are additional incentives to build telehealth infrastructure. 7
While the evidence suggests improved reimbursement has increased access to telehealth for Medicare beneficiaries, over half of Americans are covered through private insurance. 13 Since 1995, states have been enacting telehealth parity legislation, with the number more than doubling in the last 4 years (Table 1). 8 To date, 34 states and the District of Columbia have enacted parity legislation. In addition, two states proposed or are pending legislation for 2018. 8 While there is variability among states, in general, telehealth parity laws require private insurance companies to provide some level of reimbursement coverage for telehealth services. Not all of the states' laws require the reimbursement rate to be equivalent to in-person services. 8
Telehealth Private Insurance Coverage Legislation
ATA. 8
The purpose of this article is to describe the trends in telehealth utilization from 2010 to 2015 for privately insured patients. We examine the change over time in the utilization of outpatient telehealth visits between states enacting parity legislation and those who do not. To our knowledge, this is the first study to examine the effect of parity legislation on private insurance claims.
Methods
We use a quasiexperimental study design to examine outpatient telehealth visits in parity states and a comparison group of nonparity states. This study utilizes data from the 2010–2015 Truven® MarketScan Commercial Claims dataset, a nationally representative sample of patient-level claims data on utilization, expenditures, and prescription drugs. The dataset includes a convenience sample of private insurance claims from ∼100 payers (e.g., large employers, health plans, and government organizations).
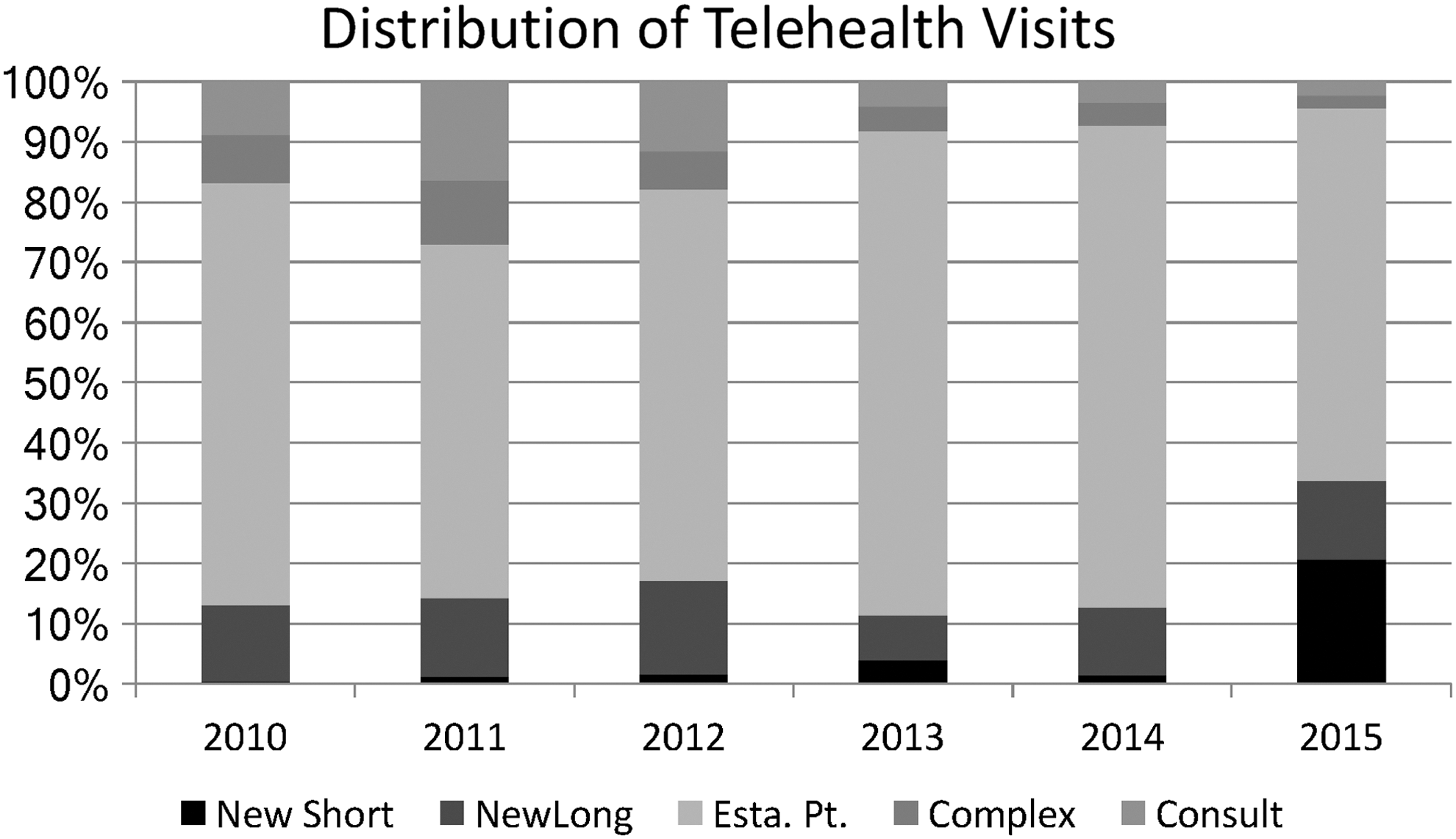
Our outcome of interest is the occurrence of a patient-level telehealth claim. For this purpose of our research, we define a telehealth visit as one using the telehealth billing GT modifier on the Current Procedural Terminology (CPT) code. For each outpatient claim, we coded as telehealth = 1 if the GT modifier occurred and 0 for in-person visits. For this study, we examined trends in outpatient visits and consultations for new patients (CPT codes 99201–99205), established patients (99211–99215), and consultations (99241–99245). We selected these 13 CPT codes because we wanted to be able to examine service mix, and these 13 codes accounted for 68.7% of the 126 different CPT codes used in billing for telehealth services in our data set. We grouped the codes into categories by assumed type of visit to visually show differences in visit type over time (Fig. 1). Visits with CPT code 99201 were labeled as “New Short” and accounts for new patient visits lasting <10 min; 99202–99205 = “New Long” includes new patient visits lasting 20–60 min; 99211–99214 = “Established Patient” visits; 99215 = “Complex”; and 99241–99245 = “Consult.” Each claim was coded as parity = 1 if the claim was in a parity state in the year that service was provided and 0 if the encounter was in a state without parity legislation. The data sample is not necessarily representative of the claims in any particular state. Therefore, we report telehealth claims that are aggregated to the parity or nonparity groupings. A state could be counted as nonparity in initial years and switch to parity status in the year legislation was enacted. Due to the large and unequal volume of nontelehealth visits in the dataset, we matched a 1% sample of nontelehealth claims based on visit types. The entire sample for this study includes over 7.5 million outpatient claims.
Distribution of telehealth visits.
We assessed the frequency of telehealth claims in parity and nonparity states as well as examined the patient characteristics across six time periods (2010–2015). Finally, we examined the effect of year and parity-state status on the likelihood of having an outpatient telehealth claim using logistic regression and a state-level fixed effect. States that enacted parity legislation after 2015 were treated as nonparity states due to the lack of claims data postlegislation. Data were analyzed in STATA 14 and SAS 9.4 software systems. The study was a determined nonhuman subjects research.
Results
We examined 7,478,472 in-person and 36,663 telehealth outpatient claims occurring between 2010 and 2015. The number of private insurance telehealth outpatient claims in the sample set, has more than tripled between 2010 (3,023) and 2015 (11,890) (Table 2). To examine this growth in context of the total volume of outpatient healthcare, we compared the annual rate of telehealth claims per 10,000 outpatient visits. Between 2010 and 2015, there was a substantial increase in the rate of telehealth claims. However, the overall utilization of telehealth by privately insured patients is still limited, with fewer than 1.5 claims per 10,000 outpatient visits in any time period. Overtime, the percentage of male privately insured telehealth utilizers is lower compared with females (Table 2). In addition, the type of telehealth visit is changing. While telehealth visits with established patients remain the most common, the percentage of new short telehealth visits lasting <10 min has increased from <1% in 2010 to 20% of the privately insured claims within the 5-year timeframe (Fig. 1).
Outpatient Telehealth Demographic Characteristics 2010–2015 (All States)
n = 36,663.
Overall, the utilization of telehealth is increasing over time (Table 3). With the exception of 2011, the number of private telehealth claims increased annually over the prior year between 2010 and 2015. In logistic regression analysis, the odds of having an outpatient telehealth claim increased by 46.4% by year (confidence interval [CI] 1.453-1.476) across all states (Table 4). In addition, those states with parity laws saw significant increases in the number of outpatient telehealth visits. Controlling for year, the odds of receiving a telehealth visit in a parity state were 29.8% greater than in nonparity states (CI 1.246–1.351).
Utilization of Telehealth Visits in Parity and Nonparity States by Year
Logistic Regression Results: Odds of Telehealth Claim in Parity States
N = 7,515,135.
Indicates with a 95% probability that the true odds ratio lies within the confidence interval (CI). 14
Discussion
In a large sample of privately insured patients, we found increased rates of telehealth utilization for claims occurring in states that have enacted telehealth parity legislation. Our findings suggest that telehealth parity legislation may facilitate utilization of telehealth services. To our knowledge, this is the first study to examine the impact of telehealth parity laws on private insurance claims. Our findings are consistent with the literature examining the impact of telehealth reimbursement policy on Medicare beneficiaries' utilization of telehealth services. 7,10
The finding that the odds of a telehealth visit is nearly 30% more likely to occur in a parity-state, highlights the potential impact of reimbursement legislation on healthcare utilization. There are many factors involved with implementing telehealth services, and no parity legislation has ever introduced a higher payment for telehealth services to incentivize adoption. The lack of telehealth parity legislation appears to have placed a disincentive on telehealth adoption and utilization in nonparity states. Failing to reimburse telehealth or reimbursing at lower rates compared with in-person care provides a disincentive for providers to adopt telehealth. 2
The lack of telehealth reimbursement may place a significant barrier to entry for many healthcare providers to explore the potential benefits of telehealth. While some critics of telehealth parity laws have raised concerns about increasing utilization and, in turn, the cost of healthcare, the results have shown that utilization is still relatively low in most states. Telehealth implementation and increasing utilization is a national trend, but considering that telehealth visits made up less than 1.5 per 10,000 private insurance claims reviewed, it appears that telehealth use is still limited, even in the states that have passed parity laws.
The findings of this study may be of policy interest given that obtaining timely healthcare services can be extremely challenging for patients who reside in rural or medically underserved communities. For those patients, in rural or remote communities, telehealth can drastically increase the opportunities to access care. 3 Expansion of telehealth parity legislation to the remainder of the states would likely remove one of the most significant restraints on telehealth utilization and facilitate additional care options for patients. In addition to differences between parity and nonparity states, we also observed a shift in the distribution of telehealth visit types. The utilization of short visits significantly increased between 2014 and 2015. It is possible that providers are perceiving efficiencies in telehealth and increasingly utilizing the shorter <10-min visits. However, further exploration should be done to better understand the recent changes in visit distribution.
There are several limitations to this study. The primary limitation is that we are reporting statistical differences in the use of telehealth by state. While we have accounted for the differences across the states that are predictors of telehealth utilization, this level of control does not allow us to capture variations within state policy approaches. Since not all parity legislation covers the same types of telehealth services, 11 future research should examine the impact of specific telehealth reimbursement policies on healthcare utilization in hospitals and other settings. This research should also include a focus on the type of telehealth service. To date, much of the legislation has focused on real-time video visits.
Future research should also examine healthcare expenditures and payment rate differences observed by state and by type of telehealth parity legislation. Given that there are vast differences in the types of coverage across parity states, yet we see an impact of parity legislation, it is quite possible that the major effect of parity legislation may be a change in provider perception of coverage.
The resulting increase of telehealth may be a Hawthorne effect but is nevertheless valuable. Another limitation is the possible miscoding or underreporting of telehealth claims, as our outcome variable relies on the inclusion of the GT modifier for telehealth claims. Due to billing compliance rules, we do not believe a miscoded claim would be any more likely to happen in one of our two comparison groups. Next, patients were not randomly selected into a parity or nonparity state and there may be additional factors contributing to the utilization of telehealth services across states. In addition, the dataset is a nationally representative sample and may not reflect the population structure at the state level. Finally, due to lack of more recent claims data we are unable to examine the impact of those states that have enacted parity legislation post 2015.
Conclusions
Utilization of telehealth services in the outpatient setting has significantly increased between 2010 and 2015. However, telehealth remains a small percentage of all outpatient private health insurance claims. Enactment of telehealth parity legislation is related to significant increases in the utilization of telehealth outpatient services. Further expansion of private telehealth insurance coverage may encourage increased utilization of telehealth services.
Footnotes
Disclosure Statement
No competing financial interests exist.