
Abstract
Background:
Emergency departments (EDs) have recognized an increasing number of patients presenting with mental health (MH) concerns. This trend imposes greater demands upon EDs already operating at capacity. Many ED providers do not feel they are optimally prepared to provide the necessary MH care. One consideration in response to this dilemma is to use advanced telemedicine technology for psychiatric consultation.
Introduction:
We examined a rural- and community-based health system operating 21 EDs, none of which has direct access to psychiatric consultation. Dedicated beds to MH range from zero (in EDs with only 3 beds) to 6 (in an ED with 38 beds).
Materials and Methods:
We conducted a needs assessment of this health system. This included a survey of emergency room providers with a 67% response rate and site visits to directly observe patient flow and communication with ED staff. A visioning workshop provided input from ED staff. Data were also obtained, which reflected ED admissions for the year 2015.
Results:
The data provide a summary of provider concerns, a summary of MH presentations and diagnosis, and age groupings. The data also provide a time when most MH concerns present to the ED.
Discussion:
Based upon these results, a proposed model for delivering comprehensive regional emergency telepsychiatry and behavioral health services is proposed.
Conclusions:
Emergency telepsychiatry services may be a tenable solution for addressing the shortage of psychiatric consultation to EDs in light of increasing demand for MH treatment in the ED.
Introduction
Emergency Department (ED) providers constantly face the challenges of not knowing what medical condition will present next and not always having access to optimal response protocols. ED providers continue to offer the best care possible within the limitations of their clinical site and available resources. One set of challenges occurs in EDs when a patient presents with mental health (MH) concerns, and there is no MH consultant to assist with diagnosis, management, and disposition.
In a white paper prepared for the Emergency Nurses Association, Manton reports that while the increased demand for management of the MH patient in EDs has resulted in boarding these patients for hours or days, many ED providers do not feel as though they are able to adequately manage patients with MH concerns. 1 Previous research from Egan et al. and Gordon suggests similar findings. 2,3 Hart calls for a shift in perception and culture within the ED to ensure optimal medical and emotional care for the patient presenting with MH concerns. 4 As the trend continues for management of MH concerns within the ED, the need and demand for resources for such management also increase.
Nationwide, there has been a steady increase in the number of MH-related ED visits. 5 Turner and Stanton report a 5% increase over the course of 1 year of patients with MH concerns presenting to EDs, and they report a 28% increase over the previous 4 years. 6 Larkin et al. report that the rate of psychiatric disorders presenting to EDs in the United States (U.S.) in 2006 was 20 ED visits per 100 ED adult admissions. 7 Studies report a 50–75% increase in MH admissions to EDs from 1990 to 2005. 8 –10 Psychiatric patients represent the fastest growing component of emergency medicine practice. 7,11 As the trend continues, further demands are placed on ED providers to deliver care to patients with MH concerns.
This study reviews ED sites from a collective of 21 integrated regional medical facilities within 3 Midwestern states. The community populations that support these medical sites range from 1,000 to 67,000. These ED sites have experienced an increase in the number of patients presenting with MH concerns. However, none has regular access to consultations with psychiatry for medication management, diagnostic impressions, or treatment recommendations. Even those medical sites that have psychiatry departments within their health system are not able to routinely access onsite ED psychiatry consultation. Furthermore, the EDs do not have access to psychological consultation for diagnostic clarification and treatment recommendations. A few sites have limited access to social workers when called from their medical hospital responsibilities for assistance with patient discharge disposition, but typically, these consults do not address MH concerns. All 21 ED sites face similar struggles with extremely limited access for MH treatment consultation. The clinical needs of patients in the ED with MH concerns cannot be fully met due to the absence of routine ED psychiatry consultation.
With the current need to coordinate MH services throughout and within 21 ED sites, a variety of options have been presented. Several options have been discussed in the literature, including onsite psychiatry consultation, dedicated treatment protocols to guide ED providers, ED case management, mobile crisis units, and ED observation units. However, the health system being studied already has a strong telemedicine service and history. 12,13 Because of this, telepsychiatry consultation to the ED for the management of this subset of patients presenting to the ED was chosen as an appropriate first step in addressing the situation. The purpose of this study was to determine if, in fact, ED telepsychiatry could be implemented successfully in this system and develop a proposal for such implementation.
Study Methods
To meet the goal of this study, the authors determined that several methods of gathering data were needed. In choosing those methods, the team followed a Quality Improvement data collection process. These methods were reviewed by the authors' Institutional Review Board and included site visits, stakeholder workshop, online survey, and data review.
Needs Assessment
A needs assessment was designed with the primary goal of obtaining clarity about MH concerns as an underserved need within the ED. A secondary goal of the assessment was to determine one or two regional clinical sites as the best choices for initial sites for ED telepsychiatry consultation. As part of the needs assessment, site visits were conducted. During these visits, ED providers and staff were interviewed and direct observation of ED logistics and management was undertaken. The first author visited each of the ED sites during 2016 with deliberate goals of (1) facilitating site investment and buy-in, (2) observing each facility to envision environmental opportunities for telemedicine, (3) addressing any concerns or questions, and (4) facilitating mutual interactions between ED site and central site. It was important to relay the message that the proposal was being offered with each site rather than being offered to each site. Meetings were held with each ED Head Nurse, ED Providers when available, and Nurse Director when available.
Emergency Telemedicine Visioning Workshop
An Emergency Telemedicine Visioning Workshop provided input from multidisciplinary ED providers and support staff. This was a day-long workshop attended by 40 people representing 10 disciplines. The 10 disciplines represented at the workshop encompassed a mix of front-line staff and leadership, including physicians (EM, Peds EM, Psych, Neuro), nurses, social workers, EMS, hospital administration pharmacy, information technology, management engineering, emergency communications, and admission transfer personnel. The workshop goals were multiple: to provide vision and inputs for the planning and pilot stages of a best-in-class emergency telemedicine program for healthcare providers and staff; to provide a solid foundation for future work, including scenarios and needs; to ensure the capture of end-user needs for both hub and spoke sites; and to create a high-level vision for the program at launch and beyond the launch at 3- and 10-year intervals.
Online Survey
An online survey was distributed to 146 ED providers across the 21 sites. Information obtained with the survey included medical and MH diagnostic considerations presented by patients as well as provider comfort regarding management of MH concerns. This survey also asked for provider impressions regarding such items as availability of psychiatry consultation, estimated number of referrals if psychiatry were available, concerns with safety for patients and staff, and frequency, acceptance, and anticipation of ED violence.
Review of 2015 Site Data
To better understand how sites operated and select pilot sites for implementation of ED telepsychiatry, daily admission data from the year 2015 were reviewed. The admission data included the total number of admissions per day/week/month/year, date, and time of MH-related admission, age of patients presenting with MH concerns, and general diagnostic considerations at the time of admission for depression, anxiety, thought disturbance, substance abuse, and personality disorder.
Results
Needs Assessment
All 21 (100% facility response rate) of the health system EDs provided valuable data. Ninety-eight medical providers responded from a pool of 146 providers for a 65% response rate. Information obtained included medical and MH patient flow in the EDs, diagnostic considerations presented, and provider perceptions of psychiatry consultation. Similarities and variations were noted within and between sites. An ED meeting/conference call and ED site visits also provided opportunities to validate or clarify information. Concern was expressed about the need and availability of psychiatry consultation, the effective treatment, and referral for patients with MH concerns and the safety of staff and patients. The needs assessment results are summarized below in the online survey and review of site data sections.
Emergency Telemedicine Visioning Workshop
Statements from the ED providers from the Emergency Telemedicine Visioning Workshop reflect concern and frustration about the management of patients presenting with MH concerns. “We need help with this patient's psychiatric needs—we simply aren't qualified.” “I need this patient assessed so we can begin treatment or placement.” “We need somebody who can help deescalate a situation!” “I am unsure if we should treat, admit, or transport this patient. What are my options?” and “I am transporting a patient—I need support on the way.” These responses point to the need for help in managing MH patients in these EDs where specialists in MH are not present or readily available.
Online Survey
Ninety-eight of 146 (67% response rate) medical providers responded to the assessment survey. Similarities and variations were noted within and between sites. On a rating scale of 0–100 with 0 representing “Never Available” and 100 representing “Always Available,” the access to psychiatry for ED consultation was rated at an approximate average of 20. On a rating scale of 0–100 with 0 representing “Very Uncomfortable” and 100 representing “Very Comfortable,” the average reported comfort level with the concept of ED telepsychiatry consultation was ∼80.
Review of 2015 Site Data
Variability of ED admissions for MH concerns for 2015 was noted per month, per day, and time of day. One site with 553 ED admissions for MH concerns exemplifies the typical results for all sites combined (5,112 ED admissions with MH concerns). The five MH concerns typically represented in EDs (mood disruption, anxiety, thought disturbance, suicidality, and substance abuse) are similarly represented at Site 1 (Table 1). There were fluctuations from 35 to 62 MH patient admissions/month and fluctuations from 62 to 96 MH patients/day. The busiest times during the day were from 1000 h through 2300 h, absorbing 442 of the 553 (80%) patients presenting to the ED with MH concerns. From 2300 h through 0800 h, 119 of the 553 (22%) patients were admitted to ED. The busiest spikes were from 1900 h through 2100 h with 119 patients (22%) and 1200 h through 1300 h with 71 patients (13%) (Fig. 1). The MH patient admissions to ED in 2015 per age are itemized as “<18 years” (69 admissions, 12%), and 18–29 (157, 28%), 30–39 (91, 16%), 40–49 (69, 12%), 50–59 (48, 9%), 60–64 (23, 4%) and “65+” (96, 17%) years (Table 2). Sixty-two patients were discharged or transferred from ED to a psychiatry unit and 24 patients were discharged from the ED to a legal facility. The average length of stay (LOS) for all ED patients was 3.2 h/admission and the average LOS for patients with MH concerns was 4.0 h/admission.

Number of ED admissions for MH concerns by 24-h clock. ED, emergency department; MH, mental health.
Site 1 Mental Health Emergency Department Admissions by Diagnosis, Number, and Percent
Percent reflects only specific diagnosis and does not account for all admissions.
Age, Number, and Percent of Site 1 Mental Health Emergency Department Admissions
Percent numbers rounded, so do not total 100%.
Two regional sites were selected as potential pilot sites representing a larger and a smaller ED site, respectively. These two sites were selected because of their proximity to each other and some shared ED staff. Site 1 is located in a community with a population of ∼16,500. The ED has seven beds available and one secure/isolation bed. In 2015, Site 1 ED processed 11,399 admissions, of which 553 patients (4.9%) were identified with some form of MH concern. ED providers in this site believe about 50% (range 25–97%) of their patients with MH concerns require psychiatry consultation and indicate that they would refer ∼8–10 (range 2–12) patients per week to psychiatry if consultation were available. Site 2 is located in a community with a population of ∼5,100. The ED has three beds available. In 2015, Site 2 processed 2,654 admissions, of which 88 patients (3%) were identified with some form of MH concern. Table 3 provides a comparison between Site 1 and Site 2 EDs for admissions of patients with MH concerns. The percent of ED admissions presenting with MH concerns is similar between sites (Site 1 [4.9%] and Site 2 [3.1%]) and the time of day for admissions of patients with MH concerns is similar (busiest times 1100–1300 h and 1800–2100 h). In 2015, the Site 2 ED served a greater percent of patients with MH concerns older than 50, than Site 1 ED. Site 1 ED served a greater percent of patients younger than 30.
Site 1 and Site 2 Emergency Department Data Reflecting Number/Percent of Diagnosis of Emergency Department Admissions
Discussion
Based on the data and analysis, this study suggests that, in fact, ED telepsychiatry can be implemented successfully in this system. The data reflect consistency in the percent of patients admitted to the ED for MH concerns compared to overall ED admissions across all 21sites. The diagnostic presentations, age groups, and time of admissions are also consistent. Providers expressed concern about the need and lack of availability of psychiatry consultation, managing the effective treatment and referral for patients presenting with MH concerns, and the safety of staff and patients. The need for MH services in the EDs is critical to patient care and the ED providers feel they have insufficient training to provide optimal care for patients with MH concerns.
National numbers as reported to the Academy of Emergency Medicine reflect that mood disruption, anxiety, thought disturbance, suicidality, and substance abuse are the general reasons that account for ∼80% of all MH ED visits. 7 The Academy report further reflects that mood disruption accounts for 30%, anxiety 23%, thought disturbance 10%, suicidality 7%, and substance abuse 30% (Table 4). A comparison of Site 1, Site 2, and national data reflecting percent of MH admissions is offered in Table 5. The differences reflected between national and Site 1 data may reflect documentation inconsistencies within regional ED sites. The Site 1 and 2 numbers are rough estimates due to inconsistent documentation procedures, but the numbers are consistent with estimates received from the other regional ED sites. Due to documentation variables, the actual number of ED admissions with specific MH concerns remains unclear. As best can be determined with the available data, the general reasons for regional site ED admissions include mood disruption, anxiety, thought disturbance, suicidality, and substance abuse, as was noted with the national data.
National Mental Health Emergency Department Admissions by Diagnosis and Percent
Percent reflects only specific diagnosis and does not account for all admissions.
Site 1, Site 2, and National Emergency Department Data Reflecting Percent of Diagnosis of Emergency Department Admissions a
Percent reflects only specific diagnosis and does not account for all admissions.
Based upon the available data, discussions with ED providers, and established precedence, Site 1 appears to have the necessary components for initial application of ED telepsychiatry consultation. This site appears to be a good representative of a regional ED. It is not the busiest or the quietest regional ED, but is busy enough to provide sufficient data for review of a telepsychiatry effort. The patient flow is similar to that noted throughout the regional sites in consideration of patient admission per community size. The ED providers have a good awareness of the needs of patients with MH concerns and a good recognition of the benefits of psychiatric consultation. A site visit to this ED revealed interest and investment in ED telepsychiatry consultation, which provided further support for recommending this location as an initial site. The community has an MH residential center that lacks onsite psychiatry management, so the ED is routinely used as a local resource for MH patient management. In addition, the ED site receives referrals/transfers from other local EDs for management and boarding. A careful staged step-wise implementation in phases, adding one ED at a time, would allow for learning, practice, and adaptation. Consideration for a secondary smaller site (Site 2) provides an opportunity for ED telepsychiatry to interact with two sites simultaneously without substantially increasing the consultation load. The similarities and differences between these two EDs allow for comparison with the application of telepsychiatry. Patient admissions managed in Site 2 represent ∼34% of the total number of ED admissions, ∼22% of number of MH concerns in Site 1. This comparison provides an opportunity to understand and adjust the ED telepsychiatry consultation before application throughout all 21 regional ED sites.
The benefit of implementing two sites together offers the opportunity to better adjust application of multisite consultation for EDs that may simultaneously compete for services. For example, if requests from two EDs present at approximately the same time, a prioritization for severity/demand must occur. This also provides opportunity to determine the functional (tele-equipment) needs of larger sites compared to smaller sites. It will be better to challenge such opportunities early on in this process. This addition of a second site is not anticipated to create a significant increase in consultation application or complications for such, but is anticipated to create an opportunity for adjusting the application of ED telepsychiatry consultation for multiple sites.
Reimbursement for telepsychiatry is becoming increasingly common among insurance providers, and in some states, it is mandatory. Two types of events are billed for every telepsychiatry visit, a provider fee and a facility fee. Telepsychiatry reimbursement guidelines for private insurance providers, Medicare, and Medicaid are found at the Center for Telehealth and e-Health Law and the American Telemedicine Association.
This article reflects something different from what already exists elsewhere in the published literature. This article presents an entire health system that is interrelated. That is, services are provided by colleagues for colleagues within the health system sites, which facilitate opportunities for greater continuity in psychiatric consultation, assessment, and intervention. Mutual ownership is greater within this effort.
Conclusions
Developing a proposal for implementing an ED telepsychiatry is the next step of this work. This implementation would occur within the framework of an already existing and successful acute telemedicine program. Already in existence in the region are other acute care telemedicine services, for example, telestroke, teleneonatology, and tele-emergency medicine, all which utilize the same telemedicine technology. All are coordinated through a centralized telemedicine activation, dispatch, and admission and transfer center (ATC). Telepsychiatry would leverage existing technology and the centralized activation system. Following the framework of the existing program, the ED telepsychiatry will rely on a central hub to process the regional ED site requests for telepsychiatry consultation. The regional sites will call a central number that connects with the ATC. Team members will triage the calls to a telepsychiatry consultant or social worker. The proposed ATC activation process is shown in Figure 2. This system is already in use by other telemedicine services in this health system and has shown to be efficient and effective.
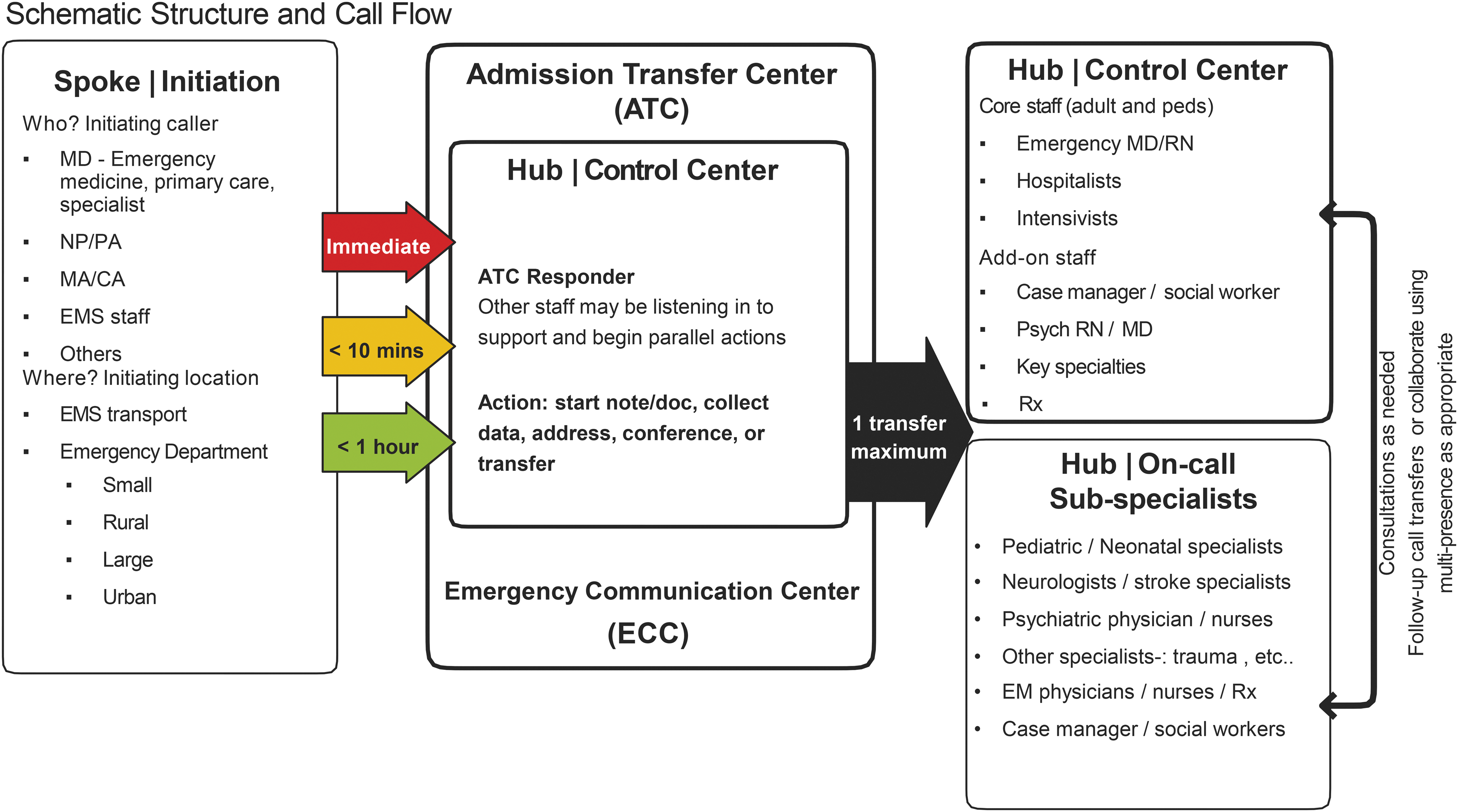
Admission Transfer Center (ATC).
The stability of this proposed telepsychiatry consultation for the regional EDs is dependent upon the standardization of a social work triage (possibly by telemedicine), the standardization of a protocol for management of patients with MH concerns, and the establishment of safety and security protocol consistent throughout the ED. These factors are inherent within this proposal and define the essential foundational components upon which the effectiveness of the proposed telepsychiatry consultation is built. Standardization and reliability within telepsychiatry consultation require standardization within each facility upon which the consultation is built. Figure 3 represents the proposed model for telepsychiatry consultation to the regional ED sites.
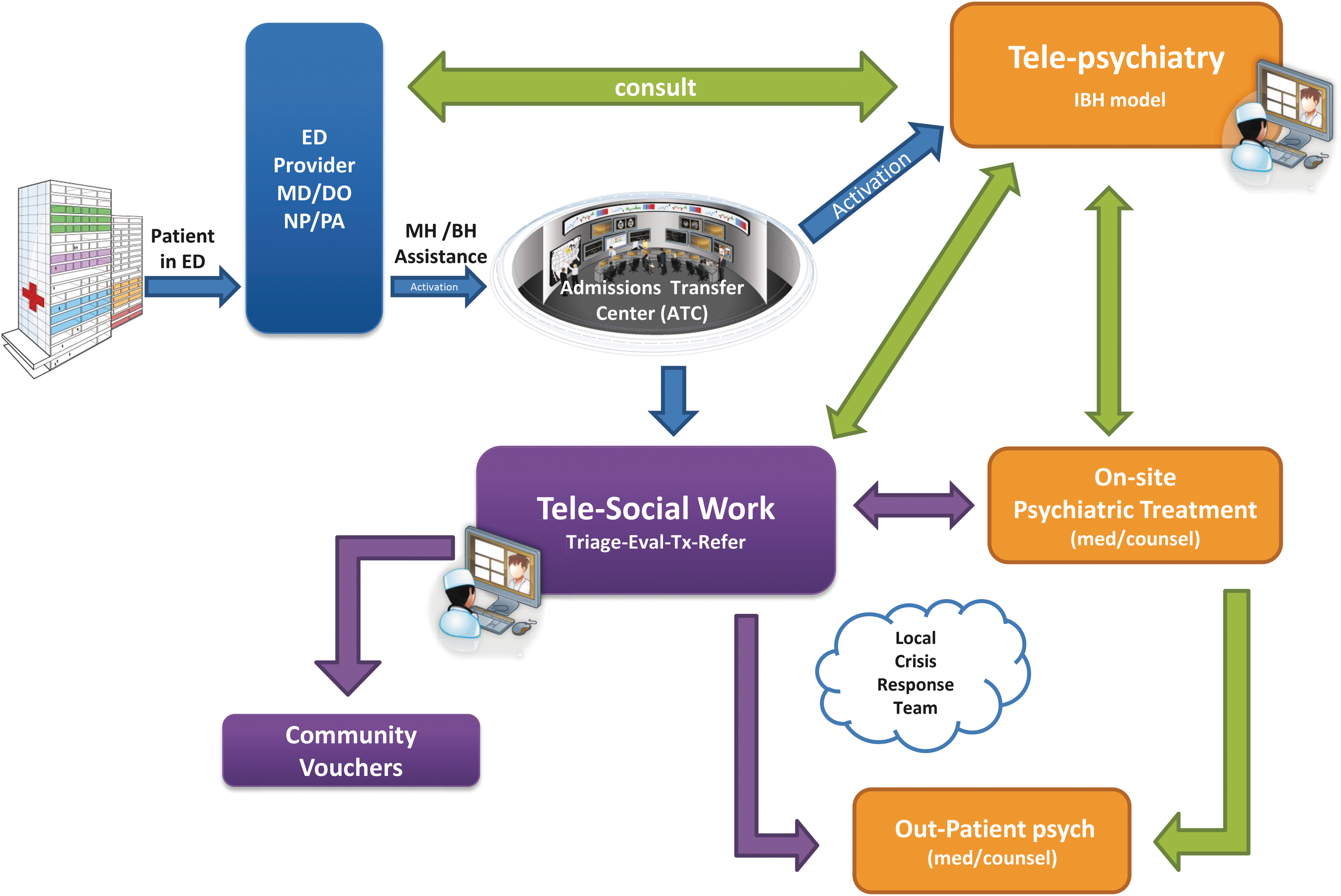
Proposed Telepsychiatry consultation to Mayo Clinic Health Systems Emergency Departments. BH, behavioral health; ED, emergency department; IBH, integrated behavioral health; MH, mental health.
ED telepsychiatry offers a clear option to assist ED staff in addressing the needs of patients who present with MH issues. It can address the issues raised by teams in this health system as well as the national concerns for managing MH in EDs. Piloting in two sites allows for better exploration of prioritizing care and collaboration between hub and spoke sites, both of which will be necessary for efficient patient care. Future research will look into the operationalization of this proposal and begin to gather foundational data concerning ED telepsychiatry.
Footnotes
Disclosure Statement
No competing financial interests exist.