
Abstract
Background:
Telemedicine is increasingly used to care for patients with movement disorders, but data regarding its global use are limited.
Introduction:
To obtain baseline international data about telemedicine use among movement disorder clinicians.
Methods:
An online survey was sent to all 6,056 Movement Disorder Society members in 2015. Scope, reimbursement, and perceived quality of telemedicine were assessed.
Results:
There were 549 respondents (9.1% overall response rate) from 83 countries. Most (85.8%) were physicians, and most (70.9%) worked in an academic or university practice. Half of respondents (n = 287, from 57 countries) used telemedicine for clinical care; activities included e-mail (63.2%), video visits (follow-up [39.7%] and new [35.2%]), and video-based education (35.2%). One hundred five respondents personally conducted video visits, most frequently to outpatient clinics (53.5%), patient homes (30.8%), and hospital inpatients (30.3%). The most common challenges were a limited neurological examination (58.9%) and technological difficulties (53.3%), and the most common benefits were reduced travel time (92.9%) and patient costs (60.1%). The most frequent reimbursements were none (39.0%), public insurance (24.5%), and patient payment (9.3%). Half of respondents planned to use telemedicine in the future, and three-quarters were interested in telemedicine education.
Conclusions:
More than 250 respondents around the world engage in telemedicine for movement disorders; most perceived benefit for patients, despite challenges and reimbursement for clinicians. Formal instruction on telemedicine is highly desired. Although the survey response was low and possibly biased to over represent those with telemedicine experience, the study provides baseline data for future comparison and to improve telemedicine delivery.
Introduction
Telemedicine is an increasingly used and recognized method of expert and timely healthcare delivery. 1 For movement disorders, such as Parkinson's disease or tremor, visual assessment of abnormal movements and their severity is important. Thus, virtual visits are particularly well suited for remote care delivery. For Parkinson's disease, virtual visits are equivalent to in-office visits, patient costs are lower, travel burden is reduced, and patient satisfaction and quality of life are similar or improved. 2 –6 Canada and the United States already use telemedicine, as part of the government healthcare system or Department of Veterans Affairs, respectively, to deliver care remotely. 6 –9 Pilot programs sponsored by the International Parkinson and Movement Disorder Society (MDS) have promoted telemedicine to deliver movement disorders expertise internationally to Cameroon 10 and to enhance care delivery for Parkinson's disease in rural parts of China. 7 In addition, emerging technologies provide new opportunities to revolutionize care for patients with movement disorders, 11,12 including deep brain stimulation telemetry, 13 wearable devices, 14 –16 and smartphone applications. 17,18
The Telemedicine Task Force was created within the MDS to devise strategies and goals to integrate telemedicine for movement disorder patients. However, published literature regarding telemedicine for movement disorders is limited to a few countries and local networks. Little data exist on global use of telemedicine among movement disorder clinicians. Therefore, the Telemedicine Task Force conducted a cross-sectional survey of all MDS members, to assess their telemedicine participation, practice settings, technology, reimbursement, and future plans for telemedicine. The project was conceived to obtain baseline data, which could be used for comparison with future assessments about telemedicine use.
Materials and Methods
Participants
All individuals (N = 6,056) listed in the MDS database were invited to participate in an online survey regarding telemedicine use. These individuals were physicians, nurses, allied healthcare staff, in industry, researchers, and others affiliated with movement disorders. The survey was open from October 16 through November 16, 2015. Reminder e-mails were sent to all MDS members before the deadline.
Survey Design
Survey questions were designed by two members of the MDS Telemedicine Task Force (A.H., E.R.D.). A pilot survey was reviewed by all Telemedicine Task Force members, and the questions were refined to avoid a large number of “other” or “unknown” responses. The final survey contained 28 questions (Appendix). Telemedicine was defined in the survey as any “Internet-based technology to provide care at a distance.” Remote face-to-face interaction by video was designated as a “video visit.” The questions assessed responder demographics, use of telemedicine and other technology, perceived challenges and benefits of telemedicine, and future telemedicine interests. Those who responded in the affirmative to telemedicine use were presented with additional questions on telemedicine scope (types of activities, including e-mailing patients), technology (hardware, software), reimbursement, and video visits (connecting sites, frequency, duration, and perception of quality compared with office visits). The survey was estimated to take 10 min to complete. Some responses were forced choice selection (e.g., yes, no, or unknown) or had a drop-down menu (e.g., “in what country are you located?”). Other responses allowed the option to select more than one answer (e.g., types of software used) or had an “other” category with a free comments section. Free-text comments were reviewed and recategorized if applicable, and the response rate was calculated. SurveyMonkey was the online survey platform used.
Statistical Analysis
Descriptive statistics obtained (Excel, Microsoft) included mean, standard deviations, medians (ranges), and frequencies (percentages). For missing responses, the denominator was adjusted to reflect the total number of responses. Selected analysis was performed for the countries with the highest number of respondents on each continent.
Results
Demographics
The survey was e-mailed to all 6,056 MDS members. E-mails were undeliverable to 44 addresses. Of the 6,012 members who received the survey, 549 responded (9.1%). The characteristics of survey respondents are compared with those of all MDS members (Table 1). Among the respondents, 85.8% (471/549) were physicians, and 58.6% of these were movement disorder consultants. There was underrepresentation from Asia-Oceania and overrepresentation from African Sections. Respondents came from 83 countries on 6 continents (Appendix Table A1). One-quarter of respondents were from the United States (most of these were from New York and California), followed by Brazil (4.9%), India (4.1%), the United Kingdom (3.6%), Canada (3.4%), and Italy (3.4%). The majority (70.9%) worked in an academic (including university) setting (duplicate answers were excluded). Half had been in practice for 10 years or less.
Demographics of Survey Respondents Compared with Those of All Members of the Movement Disorder Society a
n = 549
Because respondents could select more than one response, total percentage is greater than 100.
MDS, Movement Disorder Society; NA, not applicable.
Telemedicine Use
Half of the respondents (287/549 [52.3%], from 57 countries) used telemedicine. Of these, half (n = 132, from 33 countries) used it for movement disorders. Within the United States, 75.0% (69/92) of respondents from academic or university practices used telemedicine, and 35.9% (33/92) used it for movement disorders.
The most common telemedicine activities were e-mailing patients (63.2%), video visits (follow-up [39.7%] and new [35.2%]), and video-based education (35.2%) (Table 2). One hundred five respondents from 28 countries currently personally participated in video visits with patients. Most were from the United States (n = 38), Canada (n = 11), India (n = 6), and Australia (n = 5), and other countries had 3 or fewer respondents performing video visits. The most common outside connection sites for video visits were outpatient clinics (53.5%), patient homes (30.8%), and hospitals (inpatients) (30.3%). The median frequency of video visits was monthly. The median number of video visits performed in the past year was between 6 and 25. About 10% were “super-users” and conducted more than 100 video visits per year. Two-thirds of typical video visits lasted less than 30 min, and 3.7% lasted more than 1 h. Video visits were successful more than 90% of the time for half of the respondents. Their duration was perceived as being less than or equal to that of office visits by the majority of respondents. The quality of care was perceived by equal proportions of respondents as being either inferior or equivalent to that of office visits, and less than 10% perceived it as being superior.
Telemedicine Scope and Characteristics of Video Visits among the 289 Respondents with Personal or Workplace Telemedicine Use
Because respondents could select more than one response, total percentage is greater than 100.
Technology
The hardware used (among 232 respondents) was most commonly a desktop computer (85.8%), followed by laptop computer (50.4%), tablet (22.8%), or smartphone (8.5%). The respondents (n = 227) listed 28 types of software; 14 of these were used by single respondents. The most common were any personal computer-based software (28.2%), Skype (Microsoft) (23.8%), and Vidyo (12.8%). About a third (37.0%) did not know what type of software was used. Most respondents (of 235) indicated workplace support for telemedicine with dedicated staff (46.0%) or help desk assistance (36.6%). However, 29.4% had no support. The majority of respondents (80.4% of 459) had viewed a video of a patient's movements on a patient's smartphone or other handheld device during a clinic visit. About half did this at least monthly. About a third (150/444) used a smartphone application or other device as part of routine care. These included one or more of tremor-recording applications (46.0%), accelerometry (30.7%), examination tools (e.g., Unified Parkinson's Disease Rating Scale, spasticity scores, cognitive testing, optokinetic nystagmus strips) (10.7%), video of patient movements or gait analysis (7.3%), and sleep tracking devices (6.7%).
Reimbursement
Reimbursement patterns varied widely among 237 respondents (Fig. 1). More than half either were not reimbursed (39.0%) or did not know how they were reimbursed (19.0%). The most common type of reimbursement was public insurance (government, Veterans Affairs, universal health insurance) (24.5%), followed by patient payment (9.3%), private insurance (8.4%), and grants (7.6%). We evaluated how reimbursement differed in countries with the highest number of respondents on each continent who used telemedicine (United States, Canada, United Kingdom, Brazil, Egypt, India, and Australia) (Appendix Table A2). Public reimbursement was the most common type for Canada and Australia. In contrast, patient payment and no reimbursement were more common in the United States and India. Reimbursement status did not seem to correlate with the frequency of video visits (Appendix Table A3).
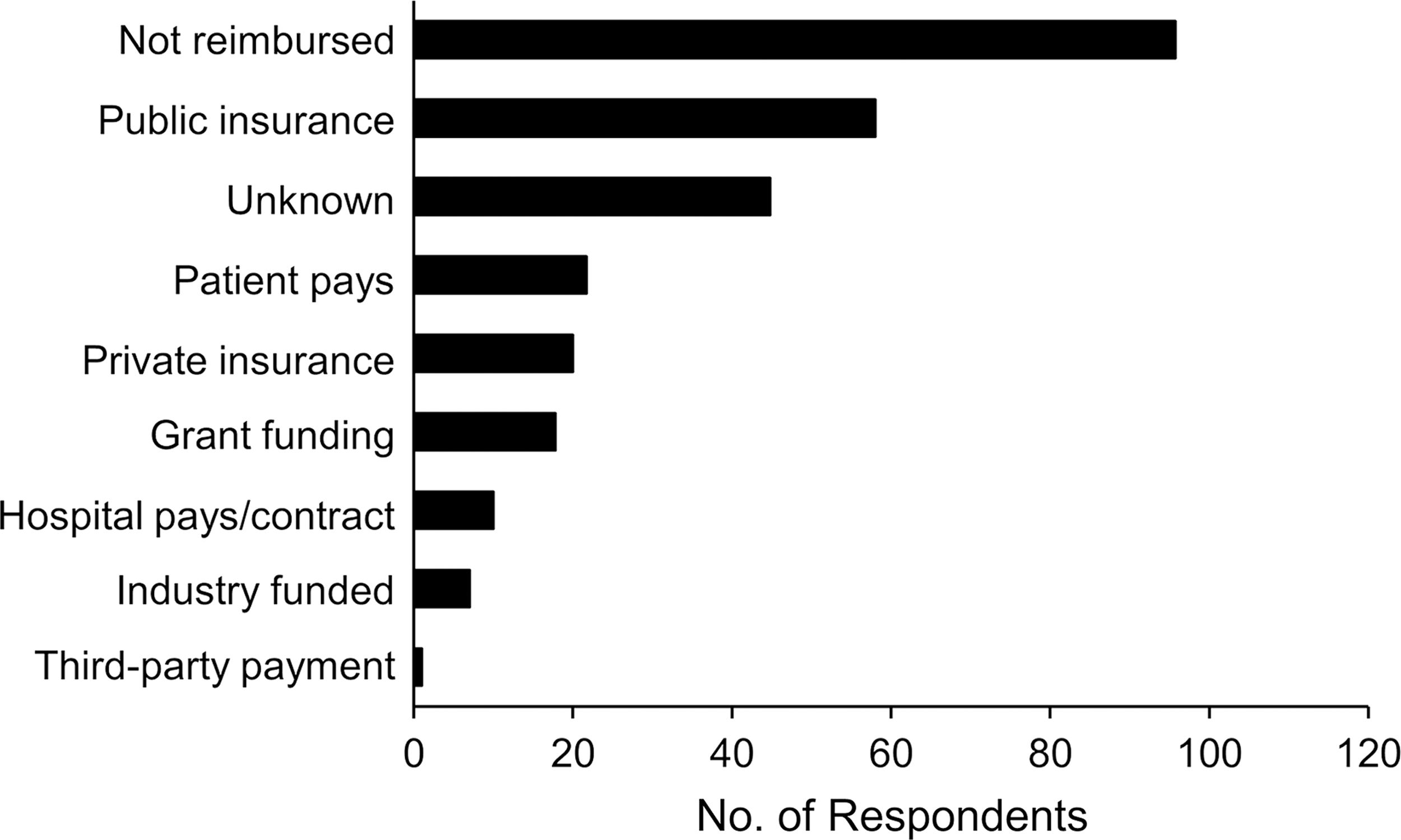
Type of reimbursement for telemedicine at workplace (n = 237 respondents).
Perceived Challenges and Benefits
A wide range of benefits and challenges of telemedicine were identified. The top 3 perceived challenges were the inability to perform a complete neurological examination (58.9%), technology difficulties (53.3%), and technical support issues (46.5%) (Fig. 2A). The top 3 perceived benefits were reduced patient travel time (92.9%), reduced patient costs (60.1%), and equivalence to office visits (20.6%) (Fig. 2B). For comparison of telemedicine users with nonusers, a greater proportion of nonusers identified challenges (89% vs. 73%, p < 0.001) and benefits (87% vs. 73%, p < 0.001) than telemedicine users.
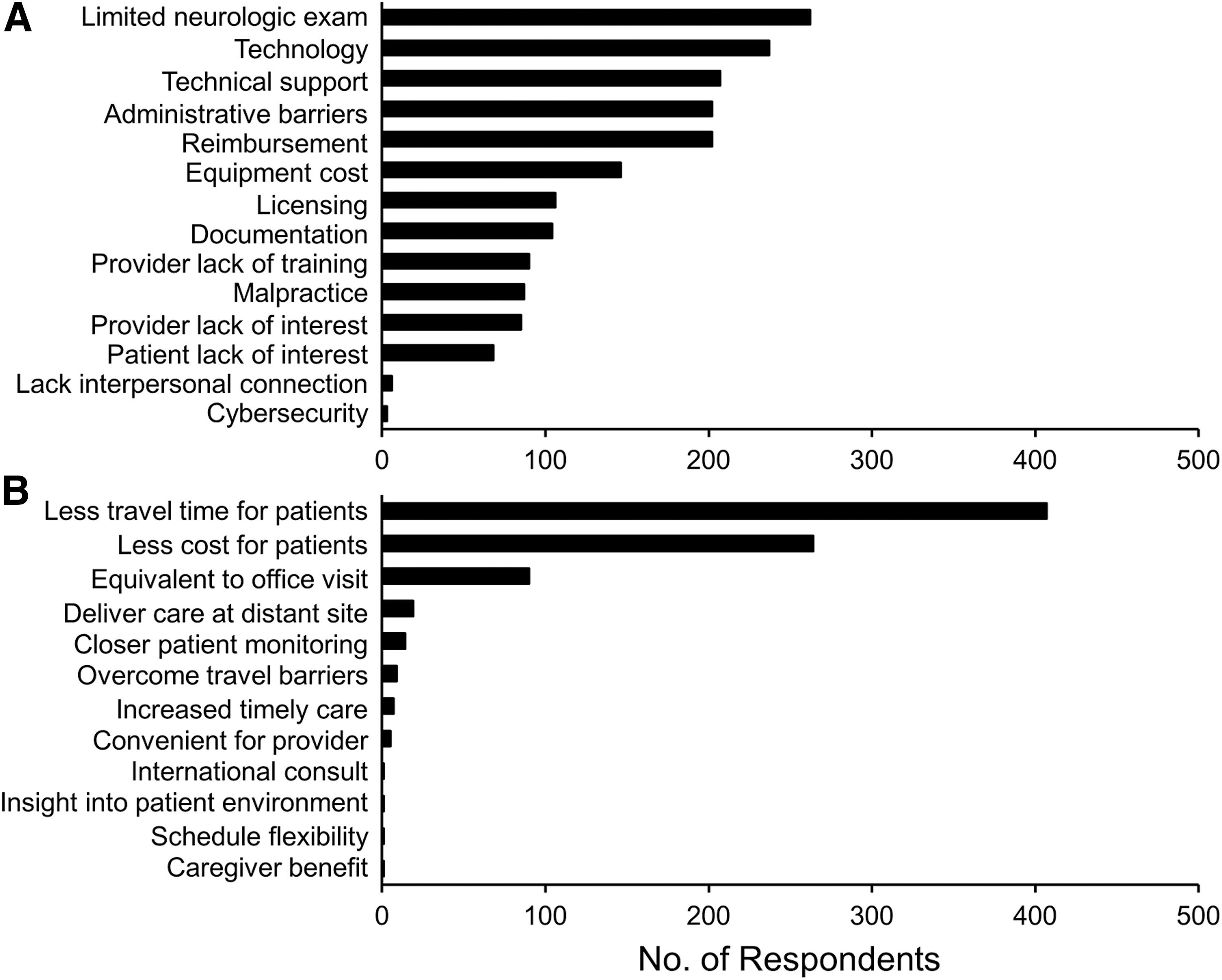
Perceived challenges
Future Telemedicine Plans
There was an interest to engage in telemedicine in the future (Fig. 3). The most requested activities were follow-up video visits (81.4%) and video-based education (58.1%). In the next year, half of respondents (52.9% of 454) planned to conduct video visits. Most (74.8%) estimated performing up to 20 visits, and 10% indicated more than 100 visits. Three-quarters of those surveyed (76% of 461) expressed an interest in an MDS telemedicine education course.

Future desires for use of telemedicine and technology (446 respondents).
Discussion
This first global survey of telemedicine use for movement disorders found that more than 250 clinicians from 57 countries are engaged in telemedicine, and more than 100 clinicians from 28 countries use it for video visits. Types of telemedicine used include e-mail, video consultation, and video-based education. The main barriers are technology and reimbursement, and the main benefits are for patients. Three-quarters of respondents are interested in telemedicine education, and half plan to conduct video visits in the future. Despite the low survey response rate, the findings provide baseline information to facilitate telemedicine services and to act as reference data for future telemedicine surveys.
Current Engagement in Telemedicine
Many movement disorder clinicians around the world currently use telemedicine for various purposes. Data for 83 countries were collected in the survey; thus, there was global representation. The use of telemedicine for movement disorders seems to be increasing. A 2012 survey reported that 60% of leading U.S. neurology departments used telemedicine and 22% used it for movement disorders. 19 In comparison, our survey found that 75% of U.S. academic respondents use telemedicine, and 36% use it for movement disorders. The increased use likely reflects the increasing uptake of telemedicine in other areas of medicine and neurology, such as telestroke. 20
Challenges and Benefits
The challenges and benefits of telemedicine were similar to those identified in other studies. 19,21 Benefits are largely accrued by patients, both tangible (reduced travel time and costs) and intangible (patient convenience, video visit access instead of no care). 22 Barriers are mounted against physicians (limited examination, technological issues, reimbursement). The restricted examination is an impediment for telemedicine when hands-on evaluation is required in addition to visual assessment. The technological issues are less problematic for active users and highlight a need for user-friendly solutions. Only half of video visits were successful 90% to 100% of the time, a rate that can undermine confidence to deliver care reliably.
The lack of reimbursement for telemedicine remains an important issue. Despite increasing interest, reimbursement in most regions of the world lags behind use. Interestingly, the lack of reimbursement did not seem to affect the frequency of video visits, a suggestion of altruism in telemedicine care. Patterns of reimbursement seemed to reflect a country's healthcare system: public reimbursement was most common in Canada and Australia, probably because of their universal health systems. In contrast, patient payment or no reimbursement was more common in the United States and India. Technology and reimbursement also emerged as topics with which respondents were unfamiliar, a finding that may explain why they were perceived as barriers.
Interest in Education and Training
Half of respondents (n = 240) planned to engage in video visits in the future, a rate that is more than twice the number currently involved in video visits (n = 105). Of the 92 U.S. academic or university respondents, 74 (80.4%) indicated a desire for future telemedicine activities. This frequency is comparable to that in the 2012 survey, in which more than 85% of 12 top departments in the U.S. planned to use telemedicine in the next year. 19 In addition, three-quarters indicated interest in a telemedicine education course, a signal of the potential future growth of telemedicine.
Technologies other than video visits are also being introduced into clinical practice and portend future change. For example, 80% of respondents had viewed a video of a patient's movement disorder on a smart device during a clinic visit. This method could greatly enhance a patient's history when describing episodic movement disorders or unclassified spells such as functional movement disorders. Respondents were interested in using smartphone applications and wearable technology, an indication that technology is poised to transform care for movement disorders in new ways. This cellular technology is now more universally available and could help overcome one of the considerable limitations of providing Internet-based care for movement disorders, especially in circumstances of poor Internet connectivity, interruptions, or no service at all for some rural residents.
Limitations
Despite our use of strategies to enhance the survey response rate (sending a reminder email stating the average time to complete the survey, and deadline for completion), 23,24 the survey response rate was low. This could be attributed to a lack of interest in the topic, time required to complete the survey, language (survey was available only in English), or outdated e-mail addresses on the MDS database. The low response rate could bias toward respondents who have an interest in or experience with telemedicine by virtue of geography, practice type, or occupation. To illustrate this point, 83.2% of respondents fit at least one of these criteria: U.S. resident, in academic practice, or being a consultant movement disorder neurologist. We did not survey the sex of respondents and thus could not assess for gender bias that may have been reflected in answers to telemedicine participation and perceptions. However, the respondents ranged from newly minted to experienced providers and thus likely reflect a wide age range. The low response rate restricted our ability to completely characterize responses within subgroups of respondents. Therefore, the findings should be interpreted with caution. However, interest in telemedicine was high as measured by absolute numbers. Future methods to increase the survey response rate include completion of the survey when renewing MDS membership or at the annual meeting, offer of monetary or nonmonetary incentives, increased marketing, adding the survey response rate to reminder e-mails, offer of survey results, or telephone follow-up. Other limitations were that the definition of telemedicine (although it was provided in the survey) was not clear to respondents and that the survey was not validated with formal testing.
Future Directions
This survey provides data to help improve telemedicine services and serves as a baseline for future comparison. Repeating the survey in the next 5 years could measure changes in telemedicine use, assess anticipated increased availability of technology, and identify shifts in reimbursement and licensure. A similar global survey of patients about telemedicine could complement the clinicians' views.
Conclusions
Telemedicine education and training were highly desired by survey respondents and should be made available. Education could be included in future movement disorder conferences, through online webinars, or through telemedicine instruction manuals on movement disorder websites. Education would also provide an opportunity to facilitate further discourse, ideas, and networking opportunities between novices and experts in the telemedicine field.
Footnotes
Acknowledgments
The authors thank the survey respondents who made this study possible.
Disclosure Statement
Financial disclosures for the previous 12 months:
Anhar Hassan: Consulting with honoraria: Bioblast. Grants/research: none. Intellectual property rights: none. Ownership interests: none. Royalties: Oxford University Press. Salary: Mayo Clinic.
E. Ray Dorsey: Dr Dorsey's effort was supported by the Patient-Centered Outcomes Research Institute. Consulting with honoraria: Abbott, AbbVie, GSK, Karger, MC10, MedAvante, Teva, UCB, Voyager Therapeutics. Grants/research: AbbVie, AMC Health, Burroughs Wellcome Fund, Huntington Study Group, Greater Rochester Health Foundation, Michael J. Fox Foundation, National Institute of Neurological Disorders and Stroke, Roche, Patient-Centered Outcomes Research Institute, Safra Foundation, and Teva Pharmaceuticals. Intellectual property rights: none. Ownership interests: stock options in BlackFynn and Grand Rounds. Royalties: None. Salary: University of Rochester Medical Center.
Christopher G. Goetz: Consulting or advisory board membership with honoraria: Acadia, Addex, Avanir, Boston Scientific, Neurocrine, Oxford Biomedica, WebMD. Grants/research: funding to Rush University Medical Center from NIH, Michael J. Fox Foundation for research conducted by Dr Goetz. Dr Goetz directs the Rush Parkinson's Disease Research Center that receives support from the Parkinson's Disease Foundation, and some of these funds support Dr Goetz's salary and his research efforts. He directed the translation program for the Movement Disorder Society Unified Parkinson's Disease Rating Scale and Unified Dyskinesia Rating Scale and received funds directed to Rush University Medical Center from the International Parkinson and MDS for this effort. Honoraria: Oregon Health and Science University. Intellectual property rights: none. Ownership interests: none. Royalties: Elsevier Publishers, Oxford University Press, Wolters Kluwer. Salary: Rush University Medical Center.
Bastiaan R. Bloem has received research grants from the Michael J. Fox Foundation, the Stichting Parkinson Fonds, the Topsector Life Sciences and Health, and UCB Pharma for research projects related to wearable sensors.
Mark Guttman: Consulting for CHDI, advisory board: Roche, Ionis, UCB Pharma. Research grants from Teva, Pfizer, NIH, NPF, and CHDI. Ownership interest: Neuroderm.
Caroline M. Tanner is an employee of the San Francisco Veterans Affairs Medical Center and the University of California–San Francisco. She receives grants from the Michael J. Fox Foundation, the Parkinson's Disease Foundation, the Department of Defense, Sage Bionetworks, and the National Institutes of Health, compensation for serving on Data Monitoring Committees from Biotie Therapies, Voyager Therapeutics, and Intec Pharma, and personal fees for consulting from Neurocrine Biosciences, Cynapsus Therapeutics, and Adamas Pharmaceuticals.
Zoltan Mari: Consulting with honorarium: Ipsen, Gerson Lehrman Group. Grants/research: NIH, MJFF, NPF, Great Lakes Neurotechnologies, and Medtronic; Ownership: Neuraly
Alexander Pantelyat: Consulting with honoraria: none. Grants/research: NIH/NINDS 5U01NS082133-05, 5P50NS038377-18; NIH/NIA 2R01AG038791. Intellectual property rights: none. Ownership interests: none. Royalties: none. Salary: Johns Hopkins University School of Medicine.
Nicholas B Galifianakis: Consulting with honorarium: none. Grants/research: NIH/NINR, Patient-Centered Outcomes Research Institute, Boston Scientific Corp. Intellectual property rights: None. Ownership interests: none. Royalties: none. Salary: San Francisco Veterans Affairs Medical Center and the University of California San Francisco.
Jawad A. Bajwa: Grants/research: intramural research grant from King Fahad Medical City, Riyadh, Saudi Arabia. Honoraria: none. Intellectual property rights: none. Ownership interests: none. Royalties: none. Salary: King Fahad Medical City, Riyadh, Saudi Arabia.
Emilia M. Gatto: Consulting or Advisor Tuteur Argentina, Bago, GlaxoSmithKlein, Teva, UCB, Genzyme, Boehringer Ingelheim, Gador Argentina.
Esther Cubo: Grants/research: European Huntington's disease Registry, International Parkinson's disease and Movement Disorder Society, AbbVie. Travel grants: Allergan, AbbVie. Honoraria: none. Intellectual property rights: none. Ownership interests: none. Royalties: none. Salary: Hospital Universitario Burgos, Spain.