
Abstract
Purpose:
The purpose of the current systematic review is to (1) guide and inform speech language pathologists involved in the treatment of persons who stutter in the development and implementation of live-stream, video telepractice services and (2) identify areas for future research related to telepractice and stuttering.
Materials and Methods:
Systematic searches of electronic databases, reference lists and journals identified seven studies that met predetermined inclusion criteria. These seven studies were analyzed and summarized in terms of the: (1) sample size, (2) characteristics of the participants, (3) technology and equipment utilized, (4) clinical setting, (5) treatment type, (6) research methodology, (7) results of the study, and (8) Oxford evidence-based practice levels.
Results:
Telepractice was used by university-based researchers and educators in the delivery of services to 80 participants who stutter. The services delivered included implementation of the Camperdown Program, the Lidcombe Program, and an integrated treatment approach.
Conclusion:
Live-stream, video telepractice appears to be a promising service- delivery method for treatment of stuttering using the Camperdown Program, Lidcombe Program, and integrated approaches. Further research is needed to determine if the initial evaluation and diagnosis of stuttering can be made using telepractice methodologies.
Introduction
Stuttering is a communication disorder characterized by repetitions, prolongations, and/or blocks of sound during speech production. According to the American Speech-Language-Hearing Association, 1 the majority (67%) of speech language pathologists (SLPs) working in schools reported that they serve children who stutter. Yet, ∼25% of SLP graduate programs do not require stuttering coursework and ∼67% of graduate programs do not offer clinical practicums for stuttering. 2 The lack of required coursework and practicums has resulted in decades of reports stating that many SLPs feel uncomfortable treating persons who stutter. 2 –5 Therefore, there is a critical need for SLPs who are well-versed in evidence-based services for individuals who stuttering. Telepractice may be one method for connecting SLPs, who specialize in working with children and adults who stutter, to the communities that are lacking such resources.
Treatment protocols for stuttering
Several treatment approaches currently exist for persons who stutter. The current review contains three primary stuttering treatment frameworks that were delivered using telepractice: (1) Camperdown Program, (2) Lidcombe Program, and (3) an integrative approach involving a combination of widely accepted stuttering treatments (e.g., fluency shaping, stuttering modification, and avoidance reduction).
O'Brian et al. 6 describe the Camperdown Program as a treatment for adolescents and adults who stutter in which the clients modify their overall speech production to facilitate fluency.
The Lidcombe Program treats children under the age of 6, who stutter, using systematic caregiver training in two stages by a trained Lidcombe SLP: Stage 1 is completed when the child presents with extremely mild to no stuttering during a set timeframe, and Stage 2 (i.e., the maintenance phase) systematically decreases clinician visits until treatment concludes. Initially, a caregiver is taught to measure the child's stuttering on a 10-point scale (1 = no stuttering to 10 = severe stuttering), and then caregivers are taught to provide contingent responses (e.g., praise, acknowledgement, or request for self-correction). 7
The third treatment, the integrated treatment approach, includes evidence-based intervention protocols that include stuttering modification, fluency shaping, avoidance reduction, and desensitization. 8
Telepractice and stuttering
Lowe et al. 9 reviewed telehealth methodologies in the assessment and treatment of stuttering. Their review included 11 articles which examined the use of telephone, webcam, internet-driven, and asynchronous treatment of stuttering. The majority of the studies (82%) included by Lowe et al. 9 yielded significant outcomes as a result of stuttering treatment provided through telepractice. However, Lowe et al. also reported concerns related to cost-effectiveness, a lack of standard of care guidances for the use of the telehealth service delivery, and a dearth of evidence-based research examining the telehealth assessment of stuttering.
A variety of remote delivery methods exist for stuttering. These include (1) telephone-based intervention, (2) live-stream video during which clinicians deliver services in real-time via videoconferencing software, (3) asynchronous treatment consisting of e-mails, messages, and/or prerecorded videos, and (4) a hybrid or mix of direct (i.e., in-person) and telehealth services. 10 However, the current preferred mode of telepractice delivery is video-based and synchronous (i.e., live-stream). 11 One reason for this preference for live-stream video intervention is that it may allow for clinician-client rapport building that most closely matches that of direct interactions. Additionally, one study comparing synchronous and asynchronous intervention noted that the time-delay associated with asynchronous intervention may result in anxiety for the client. 11 Finally, given the physical and occasionally inaudible nature of stuttering, video-based software may allow for increased accuracy in service delivery, particularly with regard to assessment. The review of Lowe et al. 9 included five telephone-based treatments and three asynchronous programs. Additionally, since the Lowe et al. 9 review, higher-quality research has been conducted on the efficacy of telepractice for stuttering. Thus, a review of the newest, synchronous, video-based telepractice services for stuttering is warranted. 12
Purpose
The current systematic review identified and analyzed peer-reviewed journal articles investigating live-stream, video telepractice treatment methodologies for stuttering. Each study is described in terms of (1) sample size, (2) characteristics of participants, (3) technology and equipment utilized, (4) clinical setting, (5) treatment type, (6) research methodology, (7) results of the study, and (8) Oxford evidence-based practice levels. This review has two purposes: The first is to guide and inform SLPs involved in the treatment of persons who stutter in the development and implementation of live-stream, video telepractice services. The second purpose is to identify areas for future research related to the use of telepractice in the treatment of stuttering.
Materials and Methods
A search of peer-reviewed journal articles was conducted in April 2017 by the second and third authors using the PubMed, Gale Group, and ASHA Journal databases and the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) Framework. 13 The PRISMA Framework allows for standardization in reporting information from peer-reviewed studies and includes both a checklist and a flow diagram. 14 This framework was selected in an effort to provide a systematic and transparent procedure for the inclusion and exclusion of articles. Moher et al. found that only 10% of systematic reviewers reported using a publicly accessible protocol, making replication of searches and inclusion/exclusion criteria difficult. 13 This literature search was performed on papers published between 2000 and 2017 to ensure the review included only the most recent and applicable research, while also accounting for rapid developments in technology. Searches included a combination of the keywords “stuttering” and “telepractice” or “telehealth” or “telemedicine” or “telerehabilitation.” Literature from non-peer-reviewed sources, such as conference papers, book chapters, and theses/dissertations, was not included in the current review. Studies were excluded if they were not in English or did not involve human subjects (e.g., simulated telehealth). Additionally, articles which used telephone-based treatment were excluded, given that the purpose of this review was to analyze live-stream, video telepractice methods for treating persons who stutter.
The search yielded 22 articles matching the keywords. See Figure 1 for a flow diagram outlining the search and selection process. The second and third authors conducted independent database searches, both yielding the same 22 articles matching the keywords. Additionally, the second and third authors reviewed the articles by reading each abstract to determine the inclusion/exclusion of studies. Interrater reliability of inclusion of studies was 100%.
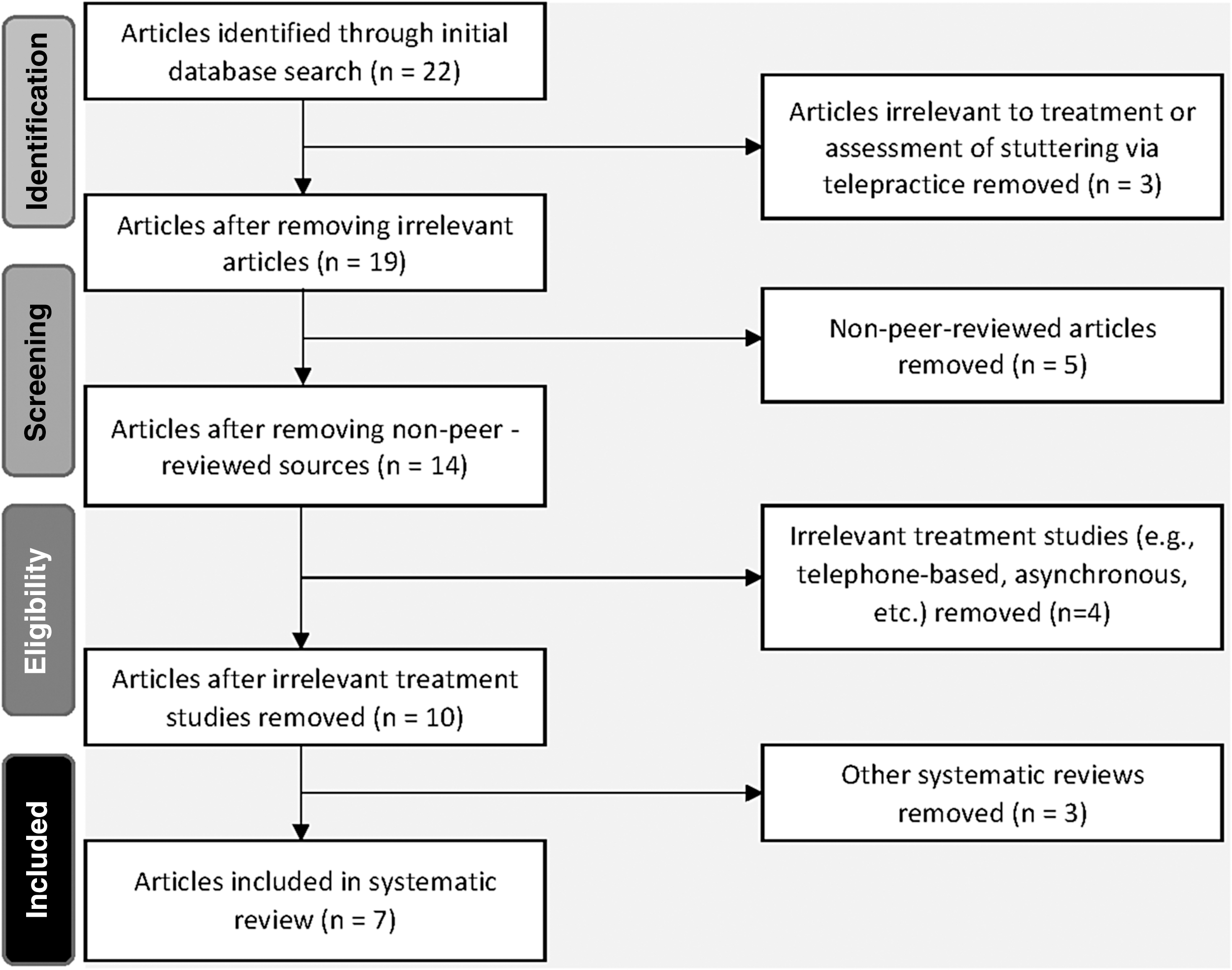
A PRISMA-style flow diagram of the search and selection process. PRISMA, Preferred Reporting Items for Systematic Review.
A standardized form was used to identify critical components of each of the studies involving stuttering treatment via video telepractice. The critical components identified included authors, publication year, sample size, participant demographics, technology and equipment utilized, clinical setting, type of stuttering treatment, research design, and results of the study.
Additionally, using the Oxford Centre for Evidence-Based Medicine (OCEBM) framework's 10-point structure, each article included in the current systematic review was assigned a level of evidence. 15 The assigned level of evidence rates the quality of the article; lower scores indicate a higher strength of evidence. The framework is outlined as follows: (1a) Meta-analyses; (1b) Individual randomized controlled trials (RCTs); (1c) Non-RCTs; (2a) Systematic reviews of cohort studies; (2b) Individual cohort studies; (2c) Outcomes research; (3a) Systematic reviews of case-control studies; (3b) Individual case-control studies; (4) Case-series; and (5) Expert opinions without explicit critical appraisal.
The second and third authors independently rated each article based on the OCEBM. Initially, interrater reliability for the articles included in the review was 71% (complete agreement for five of seven articles). Following deliberation and a discussion of the discrepancies, the raters reached agreement, resulting in 100% interrater reliability for the levels of evidence for all seven articles.
Results
Seven articles were included in the current systematic review (Table 1). Each article explored one of three primary stuttering treatment frameworks delivered using telepractice: (1) Camperdown Program, (2) Lidcombe Program, and (3) an integrative approach involving a combination of widely accepted stuttering treatments (e.g., fluency shaping, stuttering modification, avoidance reduction). Populations represented in these articles ranged from preschool children to adults. Specifically, two articles exclusively examined preschool children, one article involved school-age children, two articles investigated adolescents, and one article primarily focused on adults. Additionally, one article evaluated treatment in patients ranging in age from 3 to 19 years. Thus, the following results include a variety of treatment frameworks with a wide range of populations.
Summary of Telepractice in Stuttering Assessment and Treatment
%SS, percent syllables stuttered; CAT-R, Communication Attitudes Test-Revised.
Camperdown program via telepractice
Two research studies included in the current systematic review implemented the Camperdown Program via video telepractice. Specifically, Carey et al. 16 evaluated the effectiveness of a Phase I Camperdown Program trial on percent syllables stuttered (%SS) and maintenance with three adolescents who stuttered. A quality analysis found this article to be an evidence level 4 study according to the OCEBM due to its case-series study design without a control group. Participants in this study used Audacity software to record speech samples between Skype-led sessions. Audio recordings were then emailed to the SLP for evaluation. Across the three adolescent participants, Carey et al. 16 observed an overall 84% decrease in stuttering frequency (i.e., %SS), following 18 telepractice treatment sessions.
In their follow-up study, Carey et al. 17 investigated the Camperdown Program with an additional 14 adolescents who stutter. In this Phase II replication, participants received an average of 25 sessions of Camperdown treatment via Skype. Similar to the original (Phase I) study of Carey et al., this study (Phase II) was rated as an evidence level 4 investigation according to the OCEBM. Stuttering frequency, as a group, decreased from 6.1%SS pretreatment to 2.8%SS posttreatment. Thus, it appears that the Camperdown Program can be effectively administered for the treatment of stuttering via telepractice.
Lidcombe program via telepractice
Two articles looked specifically at the Lidcombe program conducted via telepractice. O'Brian et al. 7 investigated the telepractice implementation of the Lidcombe Program with three preschool-aged children. This study was determined to be an evidence level 4 study on the OCEBM due to its case series design with a small sample size. O'Brian et al. 7 reported that inclusion criteria for these participants included a diagnosis of stuttering obtained from a web-based assessment; however, the telepractice stuttering assessment was not detailed. Per their design, the parents used a PC-mounted webcam with broadband internet access and videoconferencing software. Participants' %SS decreased to less than 1% when measured at least 6 months after Stage 1. On average, participants reduced their %SS by 83%. Clinicians reported that the quality of audio and visual components was “acceptable for most consultations” despite occasional lapses in video. 7 Caregivers also reported overall satisfaction using the webcam. Using the Lidcombe severity rating, at pretreatment, parents rated their child's disfluencies as 4, 5, or 6 out of 10. At 6 months following Stage 1, all parents reported their child's stuttering severity as 1 or 2 out of 10.
In a follow-up RCT, Bridgman et al. 18 utilized procedures similar to those of O'Brian et al. 7 but added a direct clinician-child interaction. Forty-nine preschool children were randomly assigned either to an experimental webcam group or to an in-clinic, control group. This study 18 was rated as an evidence level 2b study according to the OCEBM due to its study design (RCT), lack of blindness, and dropout rate (10% attrition at 9 months and ∼33% attrition at 18 months). Similar to the work of O'Brian et al., 7 pretreatment and posttreatment disfluencies were analyzed from audio samples which were recorded over the telephone to determine %SS. Telepractice sessions were transmitted to parents of children who stutter using a personal computer and a webcam with videoconferencing software. Results from both groups (i.e., telepractice and direct) were found to be similar with respect to changes of %SS and stuttering severity as measured by caregivers. 18 Additionally, although 44% of parents reported that they had not used a webcam before the treatment, anecdotal reports by parents suggested that telepractice required less time (17% shorter consultations) as compared with direct treatment. 18 Thus, evidence supports the use of live-stream, video telepractice for Lidcombe Program delivery.
Integrated approach via telepractice
Three included studies explored the integrated approach for stuttering. Kully 8 analyzed the use of videoconferencing software for posttreatment consultations with one adult male who was 2-months post-intensive treatment. This study was rated as an evidence level 4 study due its case study design with one participant. The clinician used a document camera to show images to the participant during his sessions. Following this telepractice service delivery, the client and clinician “reported satisfaction with the structure of the session and the effectiveness of the feedback.” 8 According to the clinician, the audio and visual components did not interfere with their perceived accuracy of “most aspects of the patient's speech performance” with the exception of speech breathing which was more challenging to decipher. 8 Additionally, the clinician reported feeling at ease with the technical aspects of the service delivery except for some concerns related to “patient confidentiality and comfort in addressing speech-related emotional and attitudinal issues.” 8
Sicotte et al. 19 analyzed qualitative and quantitative outcomes of the feasibility and efficacy of telepractice intervention. This study was assigned an evidence level of 4 because of its case series design with a smaller sample size. Participants were six children and adolescents who were included on the basis of %SS (i.e., greater than 5%), self- or family-reporting as a person who stutters, and no other developmental, medical, or behavioral concerns. Treatment was delivered via videoconferencing with Polycom ViewStation MP using an intranet system of 768 kilobits per second. 19 Following 12–20 weeks of intervention, clinicians and clients/client families were asked to rate their experiences with telepractice. According to clinicians, technical quality was rated as moderately good with most criticisms related to image quality. The majority of clinicians reported that they were satisfied, moderately satisfied, or highly satisfied with clinical quality related to the interactions between SLPs and children with behavioral challenges. The majority of clients and their families rated both the technical quality and the clinical interaction as highly satisfactory. The majority of clients also self-reported that they were highly satisfied with both the reduction in their stuttering frequency and their overall improvement of communication skills. The average reduction of stuttering posttreatment for the six participants was 52%SS. However, at follow-up, despite some fluency being maintained, four of the six participants were noted to have an increase in %SS posttreatment. Sicotte et al. 19 demonstrated that treatment of stuttering can be successfully conducted via telepractice with mixed results for the maintenance of treatment.
Valentine 20 studied two school-age children to determine if telepractice was an effective means for generalization of skills in children who stutter. A quality review found this article as an evidence level 4 study in the OCEBM framework due to its design of three case reports across three conditions. Treatment outcomes were evaluated across three intervention types: direct (Phase I), hybrid (i.e., direct plus telepractice) (Phase II), and telepractice-only (Phase III) during a 10-week treatment period. The direct treatment sessions were conducted at a university clinic. Telepractice was delivered using Skype and personal laptops. Measurements of fluency and the clients' attitudes toward his or her speech were conducted before and after treatment phases. Best- treatment results followed the direct-only treatment condition (Phase I). However, participants continued to make gains throughout the hybrid and telepractice-only phases. It is important to note that attendance was lowest for the telepractice phase for both participants. Valentine speculated that weekly appointments outside of the home may require more preparation and attention, resulting in better attendance when compared to telepractice. 20
One parent reported a preference for the hybrid treatment, stating that, while telepractice was convenient, direct contact with the clinician was important. Of the two children, one preferred telepractice and one preferred direct treatment. Clinicians reported that telepractice sessions were “less personable than in-person contact, and they could not develop personalized transfer activities,” despite also reporting that the telepractice sessions allowed easier transfer to natural environment using participants' families. 20 Taken together, results from the three studies exploring the integrated treatment approach demonstrate that telepractice is an effective delivery method for persons who stutter.
Discussion
To summarize, the purpose of the current systematic review was to guide and inform SLPs, involved in the treatment of persons who stutter, in the development and implementation of live-stream, video telepractice services. A secondary purpose was to identify areas for future research related to telepractice and stuttering. This systematic review summarized and analyzed seven studies involving the use of telepractice to deliver SLP services to 80 participants who stutter. Services delivered included Camperdown Program, Lidcombe Program, and an integrated treatment protocol. All seven studies reported successful implementation and positive outcomes of services delivered via telepractice.
The majority of the included studies did not provide specific telepractice equivalency data but suggested that the results from their investigations were comparable to those gleaned from direct intervention. In a RCT of the Lidcombe Program by Bridgman et al., 18 no differences were detected between the direct and telepractice conditions regarding %SS and stage completion rate (i.e., the number of sessions needed to progress to Stage 2). These results are in contrast with O'Brian's 7 findings in which telepractice patients required nearly double the number of sessions to complete Stage 1 of the Lidcombe Program than is typical for patients receiving direct treatment. With regard to treatment phases, improvements in stuttering were noted during all stages, including establishment and follow-up phases, for patients with and without previous treatment. In Valentine's 20 three-phase study, the researcher found that attendance and gains were lowest in the final telepractice-only session. However, this may be due to other factors including the general plateau of improvements following initial gains and decreased motivation to attend toward the end of study. Patient and clinician satisfaction with treatment and technology appeared moderate to high across all studies despite occasional incidents of mild technical difficulties. Sicotte et al. 19 specifically discussed the challenges regarding behavior management of young children in a telepractice setting for which they recommend increased parent involvement.
These findings are consistent with the previous literature exploring telepractice treatment of autism spectrum disorders, 21 aphasia, 22 and traumatic brain injury. 23 Similar to the current review, Hall et al. 22 found that telepractice was an effective method for assessing, treating, and consulting with persons with aphasia even when compared to direct services. Specifically, they concluded similar advantages of telepractice service delivery including cost- and time-effectiveness and the provision of services to those who live in rural or geographically remote areas.
Limitations
Although the current systematic review appears to support the use of telepractice with clients who stutter, it has limitations. First, the current systematic review includes only seven studies investigating the use of synchronous, live-stream video telepractice for treatment of persons who stutter. The authors anticipated this small sample size, given the limited available research on this topic. The inclusion of only seven studies illustrates the need for future research to explore the use of evaluation and treatment protocols using synchronous, live-stream-video telepractice methods.
A second limitation is that not all of the seven articles reported the hardware and software used in their implementation of telepractice. Thus, it is difficult to recommend a specific web-based platform, computer, and webcam for use in telepractice management of stuttering. Despite a lack of evidence for hardware and software recommendations, it is recommended that clinicians use password-protected hardware and dually encrypted software to ensure client privacy. 24 Future research should include information about the hardware, software, and internet speeds used by both clinicians and clients to provide specific recommendations for practitioners.
Third, the majority of the studies included are considered low-level evidence based on their relatively weak study designs and small sample sizes. Only one study was an RCT and rated higher than an evidence level 4 on the OCEBM scale. As the current systematic review suggests, there is a need for more carefully controlled research designs, such as RCTs that directly compare a treatment and control group using telepractice methodologies. Larger sample sizes are also needed to yield stronger evidence in favor of telepractice as a service delivery option for people who stutter. Additionally, there is an ongoing need for single-subject designs, which allows a case-by-case approach for the assessment and treatment of stuttering via telepractice. The suggestion of additional single-subject designs is in line with the conclusions of Lowe et al. 9 Together, single-subject research and RCTs will allow for a more comprehensive evaluation of the use of telepractice in stuttering treatment.
Finally, despite treatment being deemed both feasible and successful across a variety of treatment programs, the efficacy of assessing stuttering using a web-based, live-stream telepractice methodology has yet to be explored. Although three of the seven studies evaluated assessment of stuttering via telepractice, none explored comprehensive stuttering assessments (e.g., percentage of stuttering, attitudes and perceptions related to stuttering, and speech and language skills). Future research should investigate the reliability and validity of telepractice assessments of stuttering as compared with direct assessments.
Clinical implications
The results of the current systematic review demonstrate the potential benefits of a telepractice delivery model for stuttering treatment. These benefits may include cost-effectiveness, time-effectiveness, and convenience. In addition, the implementation of stuttering intervention via telepractice allows clients who stutter to have increased access to SLPs who specialize in treating this population. SLPs considering treating persons who stutter via telepractice should consider several factors. First, SLPs must ensure that their software programs are dually encrypted to protect client privacy. Additionally, internet speeds should be sufficient for audio-visual transmission. Given the indirect nature of telepractice services, it is vital that SLPs devote time and effort to rapport building, particularly in the first few sessions. SLPs should also be aware that certain evaluations and treatment activities may not transfer seamlessly to telepractice, therefore requiring modification and additional creativity. Additionally, both Carey et al. 16,17 and Valentine 20 discuss concerns surrounding forgetfulness and lack of attendance for this delivery model. Hence, it may be beneficial for SLPs implementing the telepractice delivery method to consider an efficient scheduling tool with reminders to ensure attendance.
Conclusion
This current systematic review analyzed research studies investigating live-stream, video telepractice treatment methodologies for stuttering. Search results revealed seven articles related to treatment services for stuttering using the Camperdown Program, the Lidcombe Program, and an integrated treatment approach via telepractice. These studies were analyzed and summarized in terms of (1) sample size, (2) participant characteristics, (3) technology/equipment utilized, (4) clinical setting, (5) treatment type, (6) methodology, (7) results, and (8) OCEBM-levels. Evidence from the studies suggests that telepractice appears to be a promising service delivery approach in the treatment of stuttering.
Footnotes
Disclosure Statement
M.M is an Assistant Professor at Portland State University. N.N. and J.S. are graduate students at Portland State University and research assistants in the Portland State University Stuttering Laboratory. Funding for this research was provided to the first author by the Oregon Scottish Rite of Freemasonry and through Portland State University's Faculty Development Grant.