
Abstract
Introduction:
Burn care requires multiple disciplines to collaborate to achieve best patient care. Because of this, rounds involve a very large burn team to assess patients' wounds and formulate plans. To decrease the amount of team members on rounds, our burn center implemented a new budding technology: telemedicine. We created “Zoom Rounds,” a Health Insurance Portability and Accountability Act (HIPAA)-compliant, secure videoconferencing system to relay patient wound evaluations to a remote conference room where team members can participate digitally. We sought to evaluate this new rounding process by querying the burn team, patients, and families regarding their experience.
Methods:
Surveys were developed for each group and were distributed over a 2-month period. Respondents were asked to rate the videoconferencing rounding experience and comment on the educational experience (staff/providers) and one's personal experience (patient/family). We analyzed both the quantitative data with the qualitative responses. Qualitative data analysis for content was used to independently code and analyze responses to the open-ended survey questions by two authors and verified by adjudication review.
Results:
Thirty-three patients/families and 69 burn staff members completed the confidential survey (response rate of 90% and 83%, respectively). Coded responses identified several themes: inconsistent technology, improved visualization and communication regarding the wounds, better learning experience, and improved patient experience by decreased crowds in the room.
Conclusions:
There was strong support for the use of videoconferencing for patient wound rounds among providers, burn center staff, and patients/families. Telemedicine is a promising technology to improve inpatient burn rounds.
Introduction
The interdisciplinary nature of modern burn care mandates that clinicians from multiple disciplines collaborate to achieve wound healing and optimal function for burn-injured patients. In addition to physician and nursing providers who routinely perform burn wound evaluations, burn therapists, nutritionists, pharmacists, and social workers all play a role to help formulate the next plan of care. Furthermore, the need to educate the next generation of clinicians is an important goal on rounds, which further increases team size. The presence of large groups during wound evaluation conflicts with patient privacy and comfort, which are the cornerstone to patient-centered care. Patients may feel vulnerable when exposed and when many team members examine and discuss their opinions at the bedside. As such, our burn center has sought a solution that balances teamwork, communication, and patient-centric care for wound evaluations.
Telehealth solutions are part of rapidly expanding technology tool primarily used for outpatient settings. 1 –3 Although our institution implemented outpatient videoconferencing with remotely located patients several years ago, we had not yet adopted it for inpatient care. Our recent outpatient success prompted our team to adapt videoconferencing to the inpatient setting. We created a process called “Zoom Rounds,” utilizing an existing Health Insurance Portability and Accountability Act (HIPAA)-compliant, secure, videoconferencing platform (Zoom, San Jose, CA) to reduce bedside numbers during rounds. HIPAA is legislation in the United States to safeguard medical information. Through “Zoom Rounds,” primary team members evaluate wounds at the bedside, with video and audio feed to a remote conference room by two-way communication. Team members in the conference room communicate to providers at the bedside through a chat feature within the program. In this way, all team members continue to participate in patient care without being directly in the room. Education and teaching can continue in the video room without subjecting the patient to a large team presence. The goal of this quality improvement (QI) study was to assess stakeholders' perspectives on this new method to improve burn rounds and see what challenges arise using this new technology.
Materials and Methods
Context and Process of Care Evaluated
Harborview Medical Center, an affiliate of University of Washington Health System, is the sole level 1 trauma and regional burn center for Washington, Alaska, Northern Montana, and Northern Idaho. Our burn center encompasses an 18-bed burn and pediatric intensive care unit and a 24-bed burn acute care ward with a catchment area of four states. We utilized the Zoom videoconferencing program, a HIPAA-compliant, secure videoconferencing system for daily burn wound evaluation rounds. Staff explained the process of telemedicine rounding to patients and families before the start of the process. At a scheduled time each day, select patients chosen for Zoom Rounds are pre-medicated, and their wounds are undressed and cleansed in preparation for burn wound evaluation rounds. The unit charge nurse leading wound evaluation rounds carries a dedicated mobile device, either an iPad or iPod Touch (Apple, Cupertino, CA), to host the videoconferencing session. Bedside team members typically include the attending physician, the bedside nurse, and the patient's therapist. The remainder of the team, including other burn providers, nurses, therapists, pharmacists, rehabilitation psychologists, nutritionists, and social work and research staff, logs into the secure session from the conference room with a 70-inch high-definition television. The medical staff includes general and plastic surgeons, residents, medical students, as well as advanced practice providers. Communication is bidirectional (through audio feed from the patient's bedside and chat text from the conference room). In this manner, team members in the conference room can ask questions and make recommendations for care.
Data Collection Instrument
Using an iterative process, where two members of the team (T.L.L. and T.N.P.) created and piloted specific questions for this QI project, we were able to develop separate questionnaires for patients/families and members of the burn team. Questions in the patient/family questionnaire included age, education level, explanation of the process, respect of privacy, who the supervising doctors are, concerns addressed on Zoom Rounds, and a free text portion of the survey. The survey for the burn team included questions focused on role in the burn center, age, role in Zoom Rounds, evaluation of connectivity, number of times involved with Zoom Rounds, and a free text portion of the survey. To obtain an estimate of the level of support for specific facets of Zoom Rounds, we devised the questionnaire responses according to a five-point Likert scale (from strongly agree to strongly disagree).
Sampling Strategy/Data Collection Methods
We used a purposive sampling method over a 2-month period. We distributed paper surveys from September to October 2017, to both patients/families and burn team members. Completed surveys were returned anonymously to the unit nurse manager's office. To improve survey response rates, we provided reminders through emails and huddles, and during staff meetings over the study period.
Data Processing and Qualitative Data Analysis
Survey responses were entered into Microsoft Excel (Microsoft, Redmond, WA) to prepare for data analysis. Data were imported into Dedoose Version 7.0.23 (SocioCultural Research Consultants LLC, Los Angeles, CA), an online, HIPAA-compliant, data analysis software platform. This program allowed us to perform a mixed-methods analysis to score quantitative data and evaluate qualitative data through content analysis of open-text responses. We applied sentiment weighting to add a value scale (negative, neutral, and positive) to each subcategory of themes. By scoring phrases according to negative or positive direction of the content, we accounted for statement strength dictated by specific key words or phrases. We organized a categorical code structure grounded in the major themes expressed by patients/families and staff on the experience of Zoom Rounds. From the free-text responses, we identified key words to code comments into subthemes, which can then formulate major overarching themes. Research team members validated the codes for inclusion and relevance through an iterative process of ongoing discussion and double coding.
Results
Thirty-three patients/families and 69 burn staff members completed the confidential survey (response rate of 90% and 83%, respectively). Breakdown of age and education level among participants is displayed in Table 1. Survey respondents for the patient group were nearly evenly distributed among the different age brackets. The majority of patient/family respondents had a high school education. Staff characteristics are also displayed in Table 1. Burn center staff respondents were younger, with the majority of patients younger than 40. Eleven team roles were represented in the survey with nurses being the largest group. Twenty-six percent of participants remained solely in the videoconferencing room, 43% lead rounds or were bedside, and 34% participated in both roles.
Patient and Staff Demographics
N/A, non-applicable.
Sentiment data from the patient/family survey are displayed in Figure 1. The majority of patients/family felt that what to expect with wound rounds was sufficiently explained and that privacy was respected. The three respondents who stated privacy was not respected did not elaborate further in their survey. Patients felt that they were able to ask questions and that the role of supervisor attending was clear.
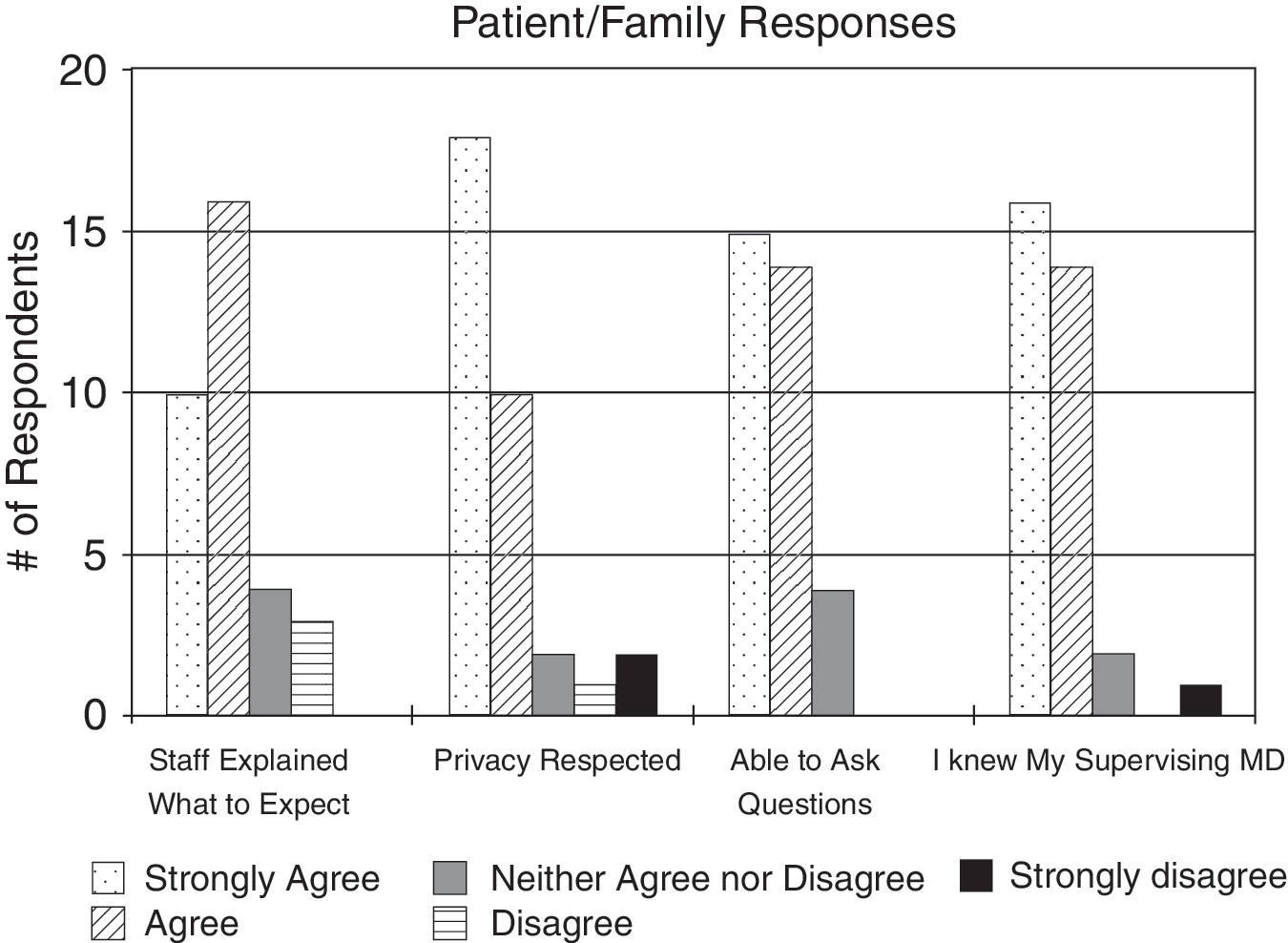
Patient and family responses.
Staff member responses are shown in Figure 2. The majority of participants who were present in the conference room felt that they could usually or sometimes view and hear participants. Most felt comfortable asking questions and relaying concerns. Figure 3 shows the overall effectiveness of Zoom Rounds. Around half of respondents felt that this was a positive change for the unit. Seventy-five percent of respondents felt that this enhanced learning.
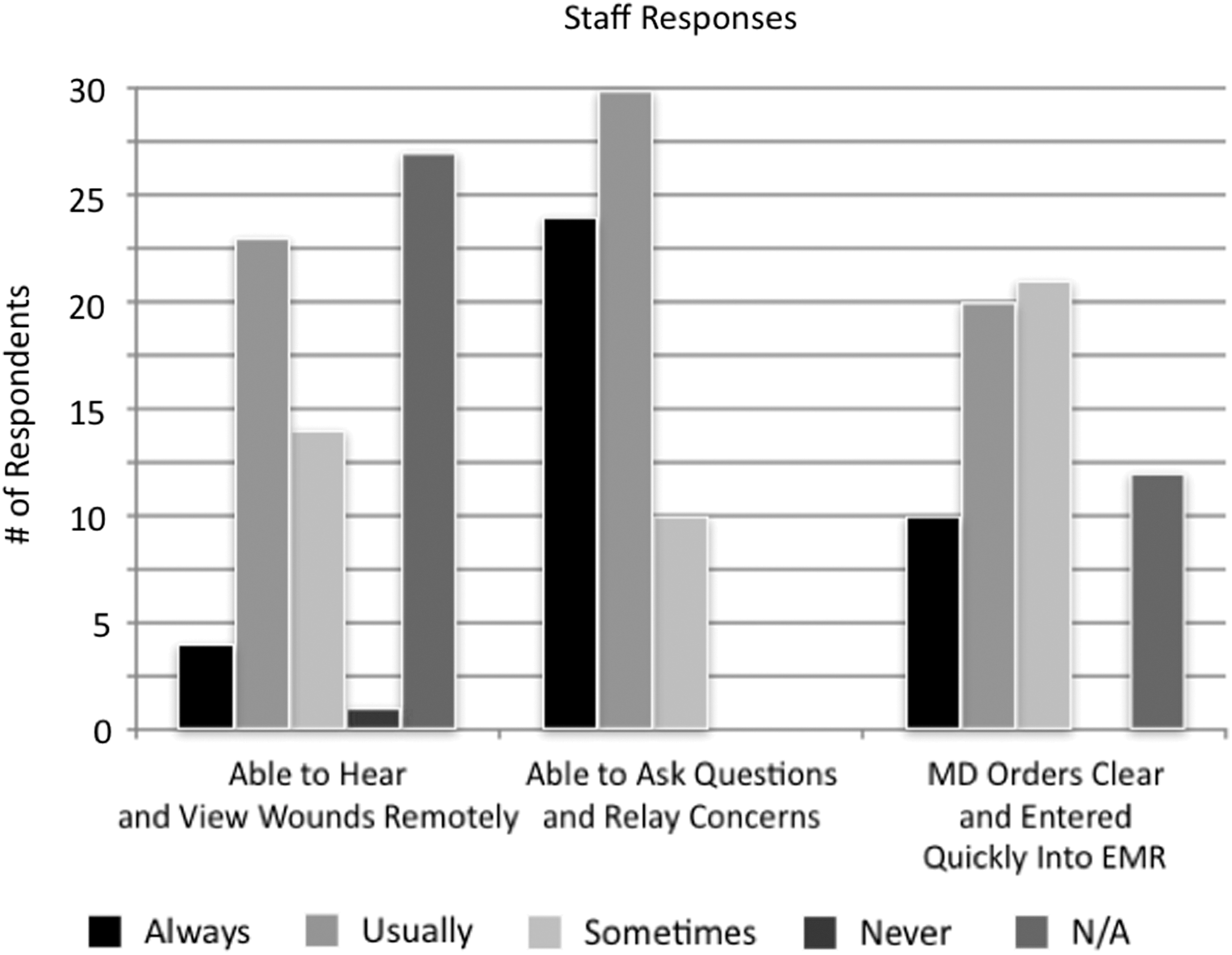
Staff responses.
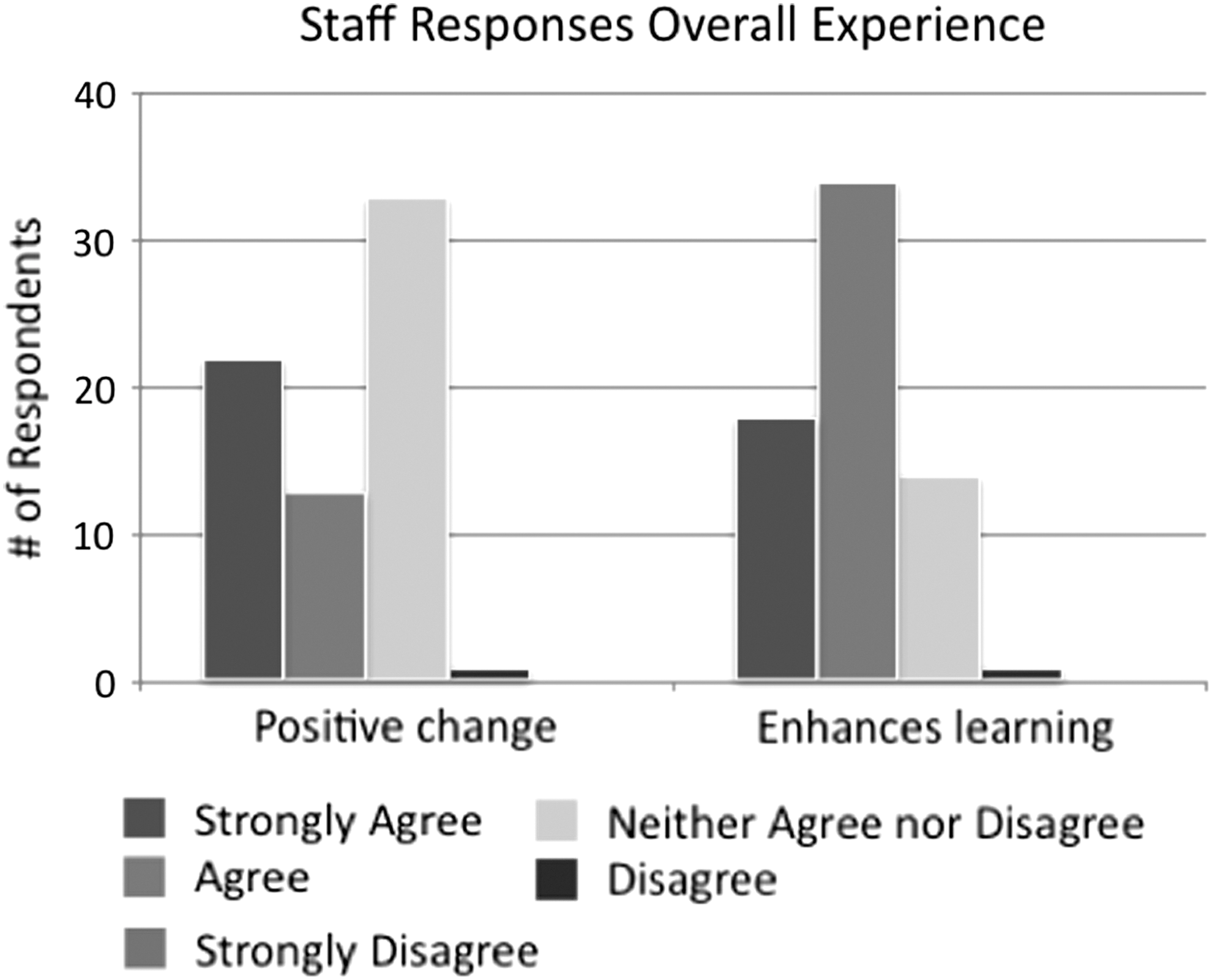
Staff responses, overall experience.
Coded open-text responses were then analyzed. Common positive themes included improved visualization and communication, better learning experience, improved patient experience, and potential for lower infection risk. Challenges faced were technological barriers such as poor audio and video quality and less interaction with patients. Residents inputting orders in the conference room felt that attendings needed to be more specific in regard to desired wound care orders. Illustrative comments that exemplify the respondents' sentiments are reported in Table 2.
Patient/Family Comments
Discussion
In 2008, Donald Berwick, the head of Centers for Medicare and Medicaid Services, described the “Triple Aims” of healthcare: improving the experience of care, improving the health of populations, and reducing per capita costs of healthcare. 4 This became the key philosophy in medicine for the following years, but leaving out one key component: clinicians. Therefore, a new quadruple aim was created, including improving clinician experience. 5 With these core beliefs, we wanted to improve the experience of both patients and clinicians in our burn center. We assumed that patients were uncomfortable and exposed during wound care and many staff felt that they were not given the opportunity to examine wounds. We also believe that less members entering and exiting patient room decreases infection risks and increases efficiency of rounding. Telemedicine offered us a unique solution. Already used successfully in an outpatient setting, 6 using the guidelines from the American Telemedicine Association Guidelines for Teleburn, we adapted this strategy for inpatient wound evaluation. 7 This telemedicine wound rounding was dubbed “Zoom Rounds.” From patient and family members, Zoom Rounds had to be an intimate and informative process. Previous studies indicate that patients are receptive to telemedicine. 8 With this new technology, fewer team members had to be physically in the room speeding up the process of rounding. From our surveys, we found that patients felt that their privacy was protected and the whole process of rounding was explained sufficiently well.
Another important requirement among the quadruple aim is to improve the staff experience. Every team member should feel they could have a good evaluation of the patient and maintain communication with other members of the team. Similar to previous studies, our telerounding was an overall positive experience with the majority of participants reporting that this was a positive change in our workflow. 9,10 The majority of staff respondents reported that this new system enhanced education compared to traditional in-person rounding. This correlates with previous studies that show telemedicine does not jeopardize and may even in fact enhance medical education. 11,12 Respondents felt that there was more time to visualize wounds without causing patient anxiety. In particular, trainees (medical students and residents) reported feeling more comfortable asking questions and discussing patient care.
Challenges that were exposed mainly involved the use of technology. The majority of problems encountered in the study included intermittently poor video quality or unreliable wireless signal. We have since addressed these challenges by working with our hospital Information Technology department to improve connectivity in specific areas of the intensive care and acute care units. Specific routers were added to each of the units and connectivity was extensively tested and improved over a 6-month period. We have also upgraded the handheld devices in which rounds are conducted to improve the quality of images and audio feed. We also have trained our providers leading rounds based on feedback from respondents to articulate thoughts and orders to ensure proper communication. Nursing staff is also undergoing feedback training to optimize video and audio feed, to make sure that proper evaluation of wounds is possible at every visit. We believe that with these improvements, Zoom Rounds has the opportunity to consistently serve as an important rounding tool for patients and providers alike.
Conclusions
At our regional burn center, there is strong support for the use of videoconferencing for examination of patients' wounds among providers, burn center staff, and patients/families. From the comments and surveys of patients/families and burn team members, respondents appreciate fewer individuals present in the room on rounds and view this inpatient telerounding strategy as a positive change to our system. One of the biggest challenges identified was technological with occasional poor video and audio quality. This has since been improved with a wireless system upgrade as well as higher quality recording devices.
Footnotes
Disclosure Statement
No competing financial interests exist.