
Abstract
Introduction
Electronic consultation (eConsult) is an emerging health innovation designed to address excess wait times for specialist care by enabling primary care providers (PCPs) to obtain a specialist consultant's expert opinion in a timely manner. According to a 2016 Commonwealth Fund report, wait times for specialist care in Canada were the highest out of 11 countries surveyed. 1 In Canada, 56% of patients waited at least 4 weeks to see a specialist, a trend that has remained consistent since 2010 and is significantly higher than the Commonwealth Fund average of 36%. Furthermore, results of the report show that one in five Canadians report that their PCP is not informed about their specialist visit, indicating a need for improved communication between PCPs and specialists similar to the international average. 1
Other countries face similar challenges in accessing specialist advice. A recent wait time report in England showed that in the first 7 months of 2017, 89.4% of patients waited up to 18 weeks to see a specialist. This result failed to meet their standard of 92% of patients waiting no more than 18 weeks for their consult. 2 In Northern Ireland, statistics from the first 6 months of 2017 revealed that 71.6% of patients waited longer than 9 weeks to see a specialist and 24.2% waited more than 52 weeks. These results have increased from 64.8% and 13.4%, respectively, in the same timeframe of 2016. 3 In Brazil, specialists described the referral process as unorganized, lacking patient triaging, and consisting of inadequate communication between providers. 4
Previous reviews evaluating Consult's use and impact demonstrated its overall feasibility in application and its ability to improve timely access to specialty care. 5,6 However, both studies revealed a lack of literature analyzing the cost effectiveness of eConsult and its impact on patient outcomes and safety. It was additionally shown that many eConsult services were primarily limited to single specialty services, particularly dermatology, thus generalizability of impact across other specialty areas was not established.
Therefore, we conducted a systematic review to expand on past reviews of the literature and examine eConsult's impact on delivery of care by applying the Quadruple Aim Framework. 7 This framework proposes that the optimization of the performance of the health system should involve simultaneously pursuing four interdependent objectives: population health, experience of receiving care (patients), experience of providing care (providers), and per capita costs. This review will provide value in informing recently published perspectives, developments, and implications of eConsult services worldwide.
Methods
Study Design
This is a systematic review analyzing the impact of eConsult on the delivery of care. The protocol was registered on PROSPERO.2017, CRD42017069139.
Data Sources
On May 11, 2017 we conducted a search through OVID of Medline (from 1946), EMBASE (from 1947), and ERIC (1965 to April 2017) and through EBSCO of CINAHL. Titles published from August 2014 to May 2017 in English or French were included. We expanded on our previous review by including ERIC and CINAHL in our search databases. The search strategy consisted of two search clusters of keywords: (1) keywords for electronic consultation (e.g., eConsult*, teleconsult*) and (2) keywords for provider care (e.g., general practitioner [GP], specialist care). Our previous review only focused on terms regarding eConsult and primary care. We broadened the second search cluster to include search terms regarding both primary and specialty care.
Inclusion Criteria
Records were screened for publication type and relevance to eConsult. Conference proceedings/articles/abstracts, editorials, letters, notes, reviews and opinion pieces, policy papers, guidelines, pilot, and case studies were excluded. Distiller SR was used to screen titles and abstracts based on predetermined relevancy criteria. eConsult was defined as an asynchronous, directed communication between providers over a secure electronic medium that involved sharing of patient-specific information and sought clarification or guidance regarding clinical care. This excluded interventions, such as web-based discussion forums, e-mail communication (unless explicitly described as secure), videoconferencing, one-way communications, and services connecting patients and providers. Examples of PCPs included family doctors and nurse practitioners. Articles that defined dentists and pharmacists as PCPs were excluded.
Two reviewers (A.M. and N.N.) screened the abstracts for relevancy, with a third reviewer (I.M.) verifying 15 of the screened articles for rigor. C.L. and I.M. performed a second abstract screen to further eliminate (or include) any articles for full screening. Full articles were then screened for relevancy by N.N. and A.M.
A modified version of the Effective Public Health Practice Project (EPHPP) Quality Assessment Tool for Quantitative Studies by Thomas et al. 8 was used to assess the quality of articles. 5 The review team consisted of 4 members (C.L., E.K., I.M., and A.M.), each assessing 11–12 articles.
The Quadruple Aim Framework
In 2008, Berwick et al. first described the Triple Aim Framework as simultaneously improving population health, improving the patient experience of care, and reducing per capita cost. 9 The Quadruple Aim Framework, proposed in 2014 by Bodenheimer and Sinksy, builds on Berwick et al.'s work by introducing a fourth dimension, provider experience of care, which researchers have described as an essential component to adoption and sustainability. 7 Therefore, the updated framework, which we have used in the present review (Table 1), includes the provider experience dimension and the corresponding outcome measures.
Overview of Quadruple Aim Framework Impact and Outcome Measures
ED, emergency department.
Data Extraction
We followed the data extraction template used in our previous review with a few modifications to capture the dimensions of the Quadruple Aim Framework. 7 The potential impacts and outcome measures are shown in Table 1. Items extracted included title, author, location, research question/objective, study design, service type, sample size, main outcomes, and findings.
Analysis
Using the Quadruple Aim Framework as a guide, we conducted a narrative synthesis of included studies. While the articles included in the study use a variety of terms to describe their electronic consultation services (e.g., e-consultation, teleconsultation), for the purposes of this study we will use the term eConsult exclusively.
Results
A search of target databases on May 11, 2017 revealed 1,021 citations. A total of 43 studies were used for data extraction after limiting publication dates to 2014-present, excluding articles not published in English or French, and removing duplicates and ineligible articles (Fig. 1).

Flow chart for study inclusion.
Table 2 shows that the majority of studies were conducted in the United States (44%) and Canada (28%), with some in Brazil (9%), Europe (Spain, Italy, Austria, The Netherlands; 7%), and Australia (2%). In addition, two services extend globally across countries: Médecins Sans Frontières (MSF) and Naval Medical Center Portsmouth (NMCP) for military services around the world.
Characteristics of Included Studies
MSF, Médecins Sans Frontières; NMCP, Naval Medical Center Portsmouth; PCPs, primary care providers; VHA, Veterans Health Administration.
The breadth of specialty services offered has greatly expanded beyond dermatology, with most studies focused on multispecialty service (84%), ranging from 8 to 86 specialties. Only 7 (16%) studies described a single specialty service, which included services in the following specialty groups: dermatology, cardiology, and pulmonology. Figure 2 shows the distribution of top specialties accessed through eConsult, with endocrinology being the most frequently accessed at 19%, followed by dermatology (16%), hematology (9%), cardiology (9%), gastroenterology 8%), and neurology (7%). The number of eConsults reported ranged from 65 to 217,014, and number of participating providers ranged from 17 to 4,260 PCPs and 4 to 479 specialists. Most articles described eConsult for PCP–specialist communication, with only one reporting on specialist-to-specialist communication. 10
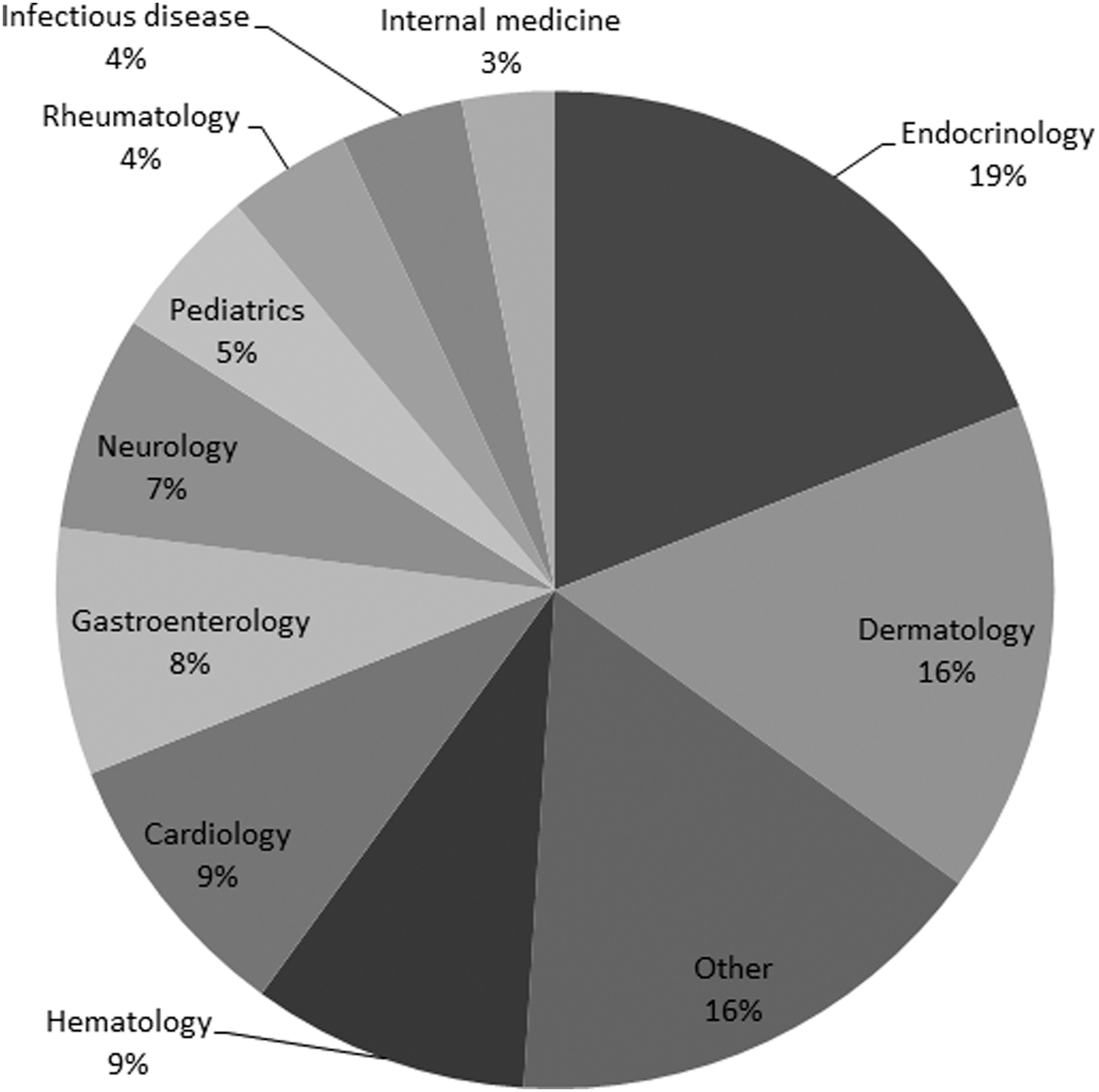
Proportions of specialties accessed via eConsult service (based on the top three specialties assessed most frequently in each article). Note: “other” refers to small proportions (1% each) for the following specialties: Chronic Back Pain, Gastroenterology and Hepatology, Medical Toxicology, Obstetrics and Gynecology, Orthopedics, Psychiatry, Pulmonology and Spirometry, Radiology, Sleep medicine, Spine Center, Transgender Care General, and Urology.
Study designs varied with most studies (40%) classified as retrospective and cross-sectional (16%), and smaller proportion of mixed method designs (7%) and randomized controlled trials (RCTs; 7%). Due to the fact that most studies were descriptive in nature, the majority (88%) of articles were categorized as “weak” based on the quality assessment tool. We did not exclude any articles based on the quality assessment.
There were multiple articles describing six eConsult services, which accounted for 67% (n = 29) of the articles: 30% (n = 13) from the Champlain BASE™ eConsult service, 9% (n = 4) from the TNMG (Telehealth Network of Minas Gerais) in Brazil, 7% (n = 3) from the Mayo Clinic, 7% (n = 3) from San Francisco General Hospital, 5% (n = 2) from the University of California San Francisco (UCSF), 5% (n = 2) from MSF, and 5% (n = 2) were from the Veterans Health Administration (VHA) (Table 3).
Service/Article Breakdown
AKO, Army Knowledge Online; CHCI, Community Health Center, Inc.; DHS, Department of Health Services; HELP, Health Experts onLine at Portsmouth; KP, Kaiser Permanente; KPCO, Kaiser Permanente Colorado; SFGH, San Francisco General Hospital; TNMG, Telehealth Network of Minas Gerais; UCSF, University of California San Francisco; VA, Veterans Affairs.
eConsult services were implemented on a variety of technological platforms (Table 4). Several services, including those at the VHA, 11,12 Veteran's Affairs (VA), 13 –15 UCSF, 16,17 and the Mayo Clinic, 10,18,19 use private networks, where the eConsult service is embedded into an electronic health record shared by referring providers and specialists, enabling the specialist to directly access patient information. Other eConsult services are independent of individual health records and use a secure web-based portals to link providers, such as the Champlain BASE in Canada, 20 –32 TNMG in Brazil, 33 –36 and KSYOS in The Netherlands, 37 or harness secure intranet e-mail as the means of communication, such as Army Knowledge Online (AKO). 38
Description of Technological Platforms
EHR, electronic health record; EMR, electronic medical record.
Population Health Outcomes
There were very few reports of eConsult's impact on traditional population health outcomes, such as risk and mortality. In a RCT of cardiology eConsults, patient outcomes, including adverse events (e.g., death, myocardial infarction, coronary artery bypass grafting, urgent or emergent cardiac catheterization and/or angioplasty) as well as hospital and emergency department utilization for potential cardiac complaints or events, were compared between those patients who had an eConsult versus those referred through a traditional referral pathway. 39 The results showed that those who had an eConsult were significantly more likely (1.5 times) to receive a consultation with a cardiologist and had lower rates of emergency department utilization than those who had traditional face-to-face consultations. 39 In another study, Price et al. 40 conducted an assessment of patient harm based on a review of all electronic referrals to a gastroenterology clinic that did not result in scheduling of appointment. Within referrals considered resolved (where the referral complaints have been resolved or addressed), only nine patients (9%) received unplanned care while awaiting scheduling decisions, five of whom experienced harm that was related to referral complaints, although authors noted that scheduling of appointments may not have avoided this harm. Within unresolved referrals (no evidence that the referral complaints resolved spontaneously or were addressed in some other way), 55 (73%) were identified as having potential for major harm (including prolonged hospitalizations, permanent disability, delayed diagnosis of malignancy, and/or death). 40 The authors concluded that the few adverse outcomes that were observed were not due to communication lapses in the referral process, but rather to being unintentionally left unscheduled with evidence for discontinuity of care and lack of patient or provider follow-up. A retrospective analysis of dermatology cases referred by MSF field doctors revealed that only 10 of 65 cases (15%) had patient follow-up data with two cases of patient death. 41 The lack of information about patient follow-up was a critical issue raised by the participating specialists and referrers. 41 Similar lack of follow-up was noted by Byrom et al., who reported that patient outcome was largely unknown in 83% of 406 cases. 42
Patient Experience of Care
Thirty (out of 43) studies reported on percentage of avoided face-to-face visits. The lowest was 7.4% 43 and the highest 78%, 36 with most studies reporting between 22% and 68% reductions in face-to-face specialist visits. Barnet et al. noted a threefold variation in the rate of eConsult requests resolved without a visit across specialist consultants. 44
Only one study described interviewing patients (in addition to providers), who had an eConsult, about their experience, including satisfaction with the eConsult program and perceived facilitators of and barriers to eConsult utilization. Overall, the patients were satisfied with the eConsult program (median ratings of 5 on a 5-point Likert scale) in terms of met expectations and confidence in eConsult. 13 They also rated the service high (median ratings of 4) for quality of care, timeliness, improved access, and safety. Furthermore, patients identified communication (effective communication with PCPs or providers) as the domain that was most important regarding their overall satisfaction with the eConsult process and unanimously indicated that they intended to use eConsults in the future based on the quality of care and the timeliness of care. 13 Other studies surveyed users (PCP referrers and specialists) to examine the services' benefits for patients. Bonnardot et al. showed that 79% of referrers reported that the advice received improved their management of the patient. 45 Similarly, Thijssing et al. reported that in 72% of the cases, the referrers indicated that they and the patients were helped by the consultant's response. 37 In three separate studies from the Champlain BASE service, primary healthcare providers (i.e., nurse practitioners and/or physicians) were asked to rate the value of eConsult to their patients using 5-point Likert scale (from 1: little/no value to 5: very high value). 24,29,31 The findings were consistently positive, with most providers (89%) rating eConsult's value to patients as high or very high (i.e., 4 or 5 out of 5).
Reducing Per Capita Cost of Care
Six articles, including two by our study group, reported on costs of eConsults (Table 5). Different techniques were used that included cost analysis, cost-minimization analysis (comparing the costs of eConsult with traditional referral methods), and cost effectiveness (determination of a savings ratio, such as a return on investment or ROI). Studies comparing costs (i.e., those conducting a cost-minimization analysis) of eConsults with in-person specialist visits report eConsult costs (viewed through impact on health services) ranging from $5 per eConsult (compared with $56 for face-to-face) 33 ; to $298 per person using eConsult (compared with $338 for face-to-face). 14 Alternatively, another study estimated monthly savings for the military (using a cost minimization analysis) by using eConsult to be $140,907 (yearly savings were $467,181); where civilian monthly savings were estimated as $28,260 (yearly savings were $105,400). 46 The return of investment was also estimated at 6.1 for eConsult in one study assessing cost effectiveness. 33 From a societal perspective, another study found (through a cost minimization analysis) that costs of eConsult averaged at $460 per patient, compared with face-to-face costs of $542 per patient. 14 Similarly, in another study, societal savings (including cost to the healthcare payer, and costs to the patient) were estimated to be approximately $11 per eConsult. 23 Finally, another study suggested a potential for millions in transportation saving by implementing eConsult to minimize face-to-face consultations. 12
Reducing per Capita Cost of Care
CA, cost analysis; CE, cost-effectiveness; CMA, cost-minimization analysis; ROI, return on investment.
Provider Experience of Care
Many studies assessed provider experiences of eConsult, including perceived value, satisfaction, educational value, quality of response, and impact on workload. There are several reports from Champlain BASE assessing perceived value using a 5-point Likert scale. Overall, more than 90% of providers rated eConsult as having a high to very high value for themselves (i.e., at a value of at least 4 out of 5). 24,29,31 In other studies, when asked about satisfaction with eConsult, 75–100% of providers reported being satisfied, 33,47 and most providers reported that they would use eConsult again in the future. 13
eConsult's educational value was noted in several studies, with 90% of providers reported having learned from eConsult, 37 whereas in others 74% reported their questions were answered, 35 and 89% thought eConsult results were conclusive. 47 Providers also reported that psychiatric eConsults increased access to specialty consultations for mental health and improved support for diagnosis and treatment. 48 In another study, 75% of providers reported no impact or decreased workload as a result of eConsult. 39 In general, the time it took for the specialists to prepare an answer to the question from an eConsult ranged from under 20 min, 24 to under 30 min, 15 to 78 min. 11
Many studies also evaluated timeliness of eConsult. The average/median time for the PCPs to receive a response from the specialists to the eConsult requests ranged from <118,49,50 to <6 days. 11,51 In a cardiology RCT, which compared time to response between eConsult and traditional referrals, the median number of days to receive a response was 5 days for eConsults versus 24 days for traditional referrals. 39 Only one study determined the median time for patient notification after eConsult and found it to be 3 days. 18
Open-ended input responses revealed that most providers appreciated the service, finding it safe, timely, easy to use, beneficial to patient care, and capable of improving communication and facilitating provider education. 25 Some challenges associated with eConsult were those relating to unclear directions from specialists, an occasional lack of information or pertinent questions delivered to specialist by the PCP, and lack of patient follow-up. 41 Moreover, although the few studies which assessed specialist experiences found them to be positive (i.e., in terms of perceived impact on patient, ease of use, improving access, usefulness), one identified challenge was the potential for an increase in workload for specialists, along with the potential for issues in communication. 30 Issues in communication refer to unclear specialist responses or expectations, which may be the result of unclear questions and expectations posed, 15 or from an unclear understanding on how to use the program. 41 Fort et al. reported that many of the specialists participating in the Safety Net Specialty Care eConsult Program in Denver Metropolitan Area believed there was room to expand the program beyond the current volume of eConsults, although this perception varied by department, with high-volume or lower-staff-ratio departments expressing interest in maintaining the program at its current size. 52
Discussion
In our updated systematic review of eConsult services worldwide, we viewed eConsult through the lens of the Quadruple Aim Framework, and attempted to assess the impact of this innovative technology on population health, patient experience of care (including quality and satisfaction), provider experience of providing care, and healthcare costs. Similarly to our past review, we found that, while the majority of new research examined outcomes related to patient and provider experience, reporting on population health and cost measures is still limited. In contrast to the previous review, we have found an increased international presence of eConsult and noted that the breadth of specialty services offered has greatly expanded beyond dermatology, with most studies (84%) focused on multispecialty and only a handful of studies addressing a single specialty service.
eConsult services in this review were shown to be effective in terms of providing faster access to specialists advice, with short response times of the participating specialists and resulting in substantial avoidance of face-to-face referral visits. The average/median time for specialists to respond to eConsult requests sent by PCPs ranged from 1 to 6 days. 11,18,51 Comparing these wait times to those typically experienced with a traditional referral pathway for face-to-face visits with a specialist, which are at least 4 weeks in Canada, 1 eConsults provide a promising alternative.
While a wider breadth of specialty services are now being offered by many eConsult services worldwide, which may enable a wider population to obtain access to specialty care, there are still significant gaps in understanding the impact of the service on population health using traditional measures of mortality, morbidity, and clinical outcomes. Only three articles in this systematic review provided some outcomes in relation to risk and mortality. While an RCT demonstrated the potential of eConsult for reducing adverse cardiovascular outcomes, 39 2 retrospective studies reported potential for harm due to lack of patient follow-up. 40,41 As the number of patients receiving eConsults increases, linking to healthcare databases to determine impact may be beneficial, despite their shortcomings related to data availability and limitations in their ability to capture the details of clinical encounters across healthcare sectors. 53,54
A majority of studies assessed patient experience of care from a PCP perspective, which points to a need to measure patient experience directly. In our own recent study, we interviewed patients who have had an eConsult done on their behalf by their PCP and reported that all patients expressed acceptance for eConsult as a model for improving access to specialist care, had largely positive experiences with it as a model of care delivery, and supported its use in their future care. 55 It is important that future research includes the patient voice through the incorporation of patient-reported outcomes and the direct measurement of the patient experiences with services such as eConsult that have direct impact on the quality of care they receive.
Findings in this review support the view that eConsult improves the work life of healthcare providers as per the Quadruple Aim Framework. Unlike other e-health technology solutions, eConsult services show sustained use and spread, high adoption, and little pushback from the providers who use them, as evidenced by high provider satisfaction ratings. 25 Furthermore, reports of provider education, quality of responses/feedback, and impact on healthcare support and workload, 37 suggest the provider experience is generally positive in these domains and point out that eConsult has the potential to improve overall job satisfaction, retention in remote communities, and provide educational/continuing professional development opportunities.
Although the articles analyzed in this review shed a considerable amount of light on the prevalence and impacts of eConsult, there are a number of limitations to consider. First, the paucity of RCTs reflects the early, emerging nature of this health technology. There is a need for more studies with stronger designs, including more traditional measures of population health. Similarly, the impact of eConsult services on specialists, although deemed fairly positive by a few articles, is another understudied area in need of further attention, especially since there is a potential for increases in workload, which could affect quality of care. 30 Finally, in agreement with our previous review, the question of cost effectiveness continues to be underexamined. Only six studies attempted to address and report on the economic impact of eConsult services. All used different methods, ranging from cost analysis, through cost-minimization analysis, to cost effectiveness. In general, these studies yield promising findings in terms of cost savings to the healthcare systems, return of investment, and societal savings. Regardless, studies like those assessed in this review, are useful in assessing and adding to our current understanding, and can be used as an exploratory base for further research.
Conclusions
We assessed the breadth of literature on eConsult through the lens of the Quadruple Aim Framework to guide our narrative synthesis and attempted to assess the impact of this innovative technology on population health, patient experience of care (including quality and satisfaction), provider experience of providing care, and healthcare costs. We characterized the various technology platforms used and confirmed that they still range from services built into existing shared electronic health systems to stand-alone web-based portals. The results to date indicate that eConsult systems have expanded significantly internationally and are largely multiservice in nature. While the majority of new research examined outcomes related to patient and provider experience, the population health and cost measures continue to be limited and require further development.
Footnotes
Acknowledgments
The authors would like to thank Canada Health Infoway for providing financial support for the students who helped conduct this study. Additional funding for this study was provided by the Ontario Ministry of Health and Long-Term Care and the Canadian Institutes for Health Research. The funders were not involved in the study design, data collection, data analysis, or article preparation, or in the decision to publish the results. The views expressed do not necessarily reflect those of the Province of Ontario. For the purposes of transparency, the authors would also like to note that their service, the Champlain BASE eConsult service, was among the programs identified by this review.
Disclosure Statement
The authors have no conflicts of interest to declare, real or perceived.