
Abstract
Background/Objectives:
The Department of Veteran Affairs (VA) Home-Based Primary Care (HBPC) program provides care to over 37,000 high-risk, high-need, medically complex, and costly patients in their home. The VA's Home Telehealth (HT) program can potentially amplify HBPC's efficiency and reach, yet scarce data on use and experience with HT in HBPC exist. This exploratory study sought to provide a glimpse of HT use in HBPC and identify drivers and barriers for HT implementation.
Design:
National VA data were used to evaluate HBPC patients concurrently using HT. We conducted a cross-sectional survey of HBPC program directors to explore HT use, understand communication processes, and elicit open comments. Semistructured interviews were conducted of 18 HBPC program directors with varying HT use to clarify themes and understand HBPC experience with HT.
Results:
Fifteen percent of the overall HBPC patients used HT in 2011, with a wide variation in HT use by HBPC site. The national survey and semistructured interviews revealed that most HBPC staff recognized advantages of using HT, including increased patient engagement and staff efficiency. Crucial practices among sites with successful telehealth adoption included HT staff attending HBPC meetings and evaluating all HBPC patients for HT.
Conclusion:
Much remains to be done for effective HT integration in HBPC. Improving communication between HT and HBPC programs and establishing a system for identifying suitable patients for HT are vital. Future studies need to delineate operational processes and gather data on the added value of HT in HBPC to guide evidence-based integration of HT in VA and Medicare HBPC programs.
Introduction
Approximately 4 of the 9 million Veterans who enrolled in the Department of Veterans Affairs (VA) for care are over age 65. As Veterans age, their needs increase and become more complex. The VA Home-Based Primary Care (HBPC) program provides primary care in the home to community-dwelling aging Veterans who have complex acute and chronic medical disease burden and functional impairment 1 and is currently one of the largest HBPC providers in the United States. The HBPC interdisciplinary team traditionally monitors their patients' status between visits through telephone, providing close case management and often making urgent home visits as needed. 2,3 The mean age of HBPC patients is 78.4 years, they have on average more than eight chronic conditions, and 48% are dependent in two or more Activities of Daily Living. 1
While seemingly similar to Medicare home healthcare, HBPCs are markedly different: in contrast to the Medicare home healthcare's episodic, time-limited, and problem-focused skilled services typically provided by a single provider, HBPC provides comprehensive longitudinal primary care to patients, using an interdisciplinary team model. VA HBPC has been successful in lowering hospitalizations and also cost, although data regarding cost are mixed, so much so, that it now forms the foundation of Medicare's HBPC demonstration, Independence at Home. 4
Given overall success of the HBPC program in delivering high value care, the VA is examining means to expand the HBPC program capacity and efficiency, and the VA's Home Telehealth (HT) program offers a potential tool. 1,5 –11 The VA's HT is a national program providing secure technology-assisted health information exchange for monitoring and care coordination for community-dwelling Veterans with poorly controlled chronic conditions, such as diabetes, hypertension, heart failure, chronic lung disease, and so on.
The VA HT can broadly be divided into two categories as follows: (1) home monitoring with messaging devices without video, 12 and (2) video into the home through telehealth devices, including tablets. 13 This article examined only home monitoring with messaging devices without video, which will henceforth be called HT. The two major HT devices used by the VA at the time of this project were Health Buddy and Viterion which allowed monitoring of basic physiological data coupled with simple messaging.
To be eligible for HT, Veterans were required to have a chronic condition that would benefit from monitoring and have documented ability and willingness to use the HT technology daily, either themselves or with caregiver assistance. Every patient who is recommended HT by their primary provider is assessed for eligibility by a HT care coordinator: explicit enrollment criteria include a poorly controlled chronic condition or one that requires frequent admissions or ER visits, and their documented willingness and ability to respond to the HT technology daily. Care coordinators, including nurses, social workers, nutritionists, and so on, manage a panel of ∼100–120 patients each. Care coordinators select appropriate HT technology based on patient capability using an algorithm and provide training to the patient and caregiver.
Patients using HT technology receive automated text-based disease-specific messaging and provide disease-specific physiologic data such as blood pressure and blood sugar daily. Patient responses are processed and are available to care coordinators through secure websites for review, and the data are prioritized based on preset alerts for specific signs and symptoms. Care coordinators contact patients with high risk responses to evaluate symptoms, assess changes and medication adherence, determine interventions needed, and coordinate their care with the primary physicians, pharmacy, social work, and other care team members. Daily monitoring of patients through HT can enable care coordinators and primary providers to detect early warning signs and intervene preemptively and, therefore, prevent expensive emergency department visits and hospitalizations.
Figure 1 is a schematic representation of the VA's HT program. We use a circle to depict care coordination activities, following the model from the Agency of Healthcare Research and Quality. 14 One review of over 40,000 Veterans enrolled in HT showed a reduction in admissions (19.7%) and admission length of stay (25.3%). 15 However, analysis was not specific to HBPC patients.
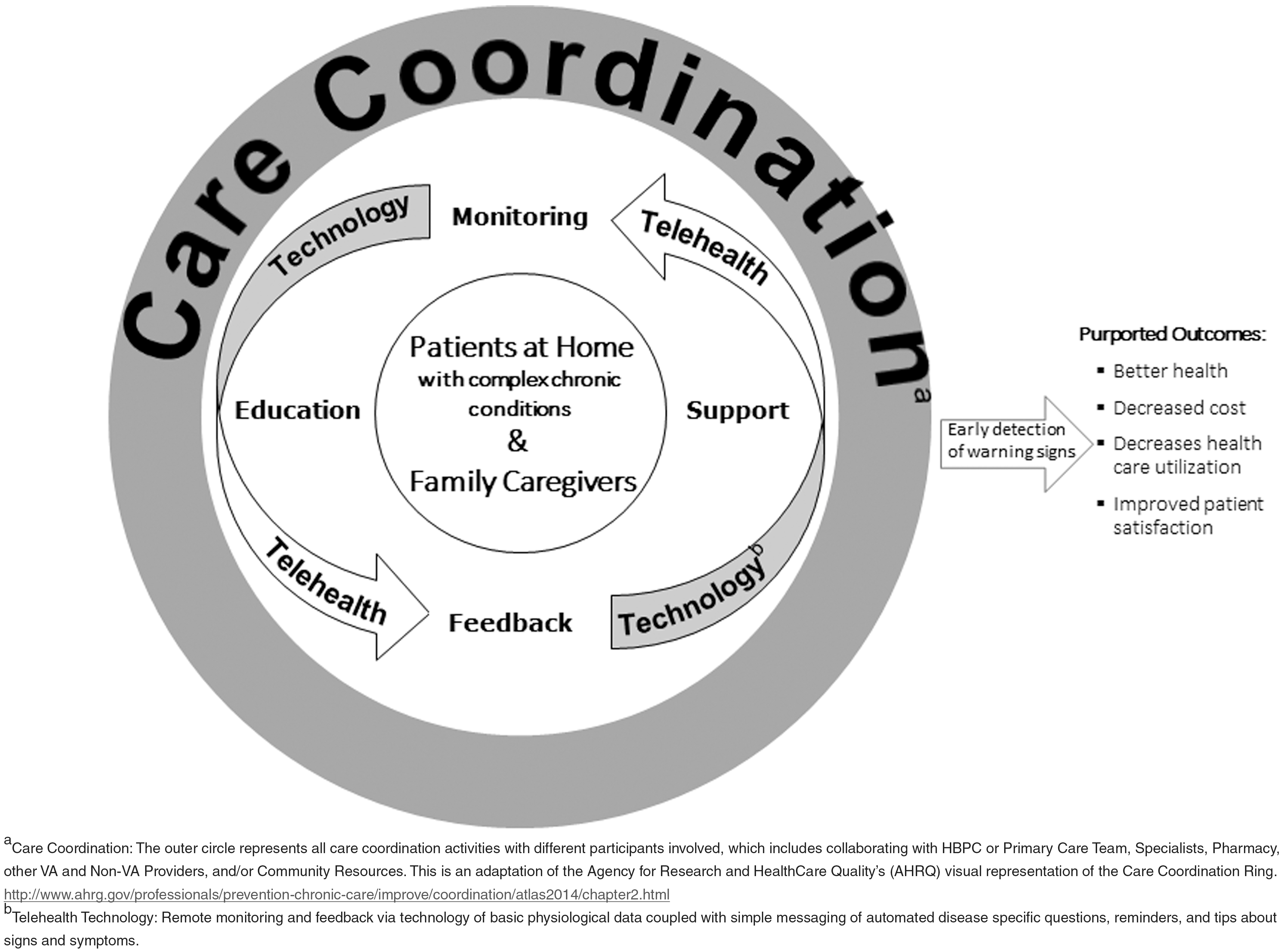
Schematic of VA Home Telehealth Chronic Disease Model.
HBPC has utilized HT as a tool to monitor patients for several years; however, little is known about HBPC's use and experience with HT, and even less is known about interpersonal behaviors such as communication patterns in this setting. While there are some data illustrating HT's potential and exploring its sustainability in Medicare home healthcare, 16 –19 and examining the role of video in HBPC, 13 to the best of the authors' knowledge, there is no report on use of HT specifically in VA HBPC. The aims of this exploratory project were to: (1) obtain an overview of use of HT in HBPC, (2) identify drivers and barriers of HT use in HBPC, and (3) identify crucial practices among sites with high HT use. We did this by examining national data and surveying the field.
Methods
This exploratory project was conducted in 2011 in three parts.
Examining National Data
Using national data, the number of HBPC patients using HT was extracted from the VA's Managerial Cost Accounting System, formerly called Decision Support System. This is an activity based cost allocation system that generates cost estimates for individual VA hospital stays and healthcare encounters. Co-utilization data were used to gather “HT use”—the percent of patients enrolled in HBPC during the previous year who also used HT for any period during the year. HBPC programs were sorted arbitrarily into high (≥20% of HBPC patients using HT during the year), intermediate (11–19%), and low (≤10%) HT users.
National Survey of HBPC Program Directors
Next, we created a brief questionnaire in collaboration with the national HBPC director and an HBPC medical center director. The goal was to explore HT use and HBPC experience with HT and invite open comments on the topic (Table 1). All 137 HBPC program directors were invited to answer the nonvalidated questionnaire through a single e-mail. To enhance participation, the national HBPC director described the survey and explained its importance during a national HBPC program directors' monthly call; response was encouraged from everyone, but not mandatory. Survey responses were identified.
Questions in the National Program Director Survey
HBPC, home based primary care; HT, home telehealth.
Semistructured Interviews of HBPC Program Directors
We interviewed HBPC program directors from VA's around the country using a semistructured interview guide with open-ended questions (Table 2). Questions were drafted after reviewing themes identified in the national survey with input from VA Geriatrics and Extended Care Office personnel. The same interviewer conducted all interviews over the telephone, lasting between 15 and 30 min. We sought to understand barriers and facilitators of HT use and best practices. Questions specifically queried regarding HT experience, monitoring, communication, patient identification, structural setup, and added value.
Questions in the Semistructured Interview
We collected semistructured interviews of 18 program directors. The sampling frame was designed to gather feedback from HBPC programs across the HT user spectrum (high, intermediate, and low utilization), while ensuring reasonable variation in geographic region and catchment area. The final HBPC program directors interviewed were as follows: eight high, four intermediate, and six low HT users, based on national data with a reasonable variation in geographic region [Northeast (4 sites), Southeast (7), Midwest (6), Pacific (1)] and catchment area [urban (14), >50% rural (3)]. 20 –22 We specifically oversampled the high users to understand best practices for implementation and low users to understand their reasons for nonuse.
Analyses
Descriptive statistics was calculated for HT use in various HBPC sites. Semistructured interviews were transcribed, and responses entered using a Microsoft Excel. Two researchers then read the data independently searching for common themes. After open coding, data were analyzed and arranged into themes, to understand perceptions toward HT use, HT drivers and barriers, and effective practices.
Results
National Data
The total number of unique Veterans served by HBPC nationwide during 2011 was 39,387, and the number of unique HBPC patients who used HT at any time during the same year was 5,755 or 15% of the overall HBPC patients nationally. However, the percent of unique HBPC patients using HT in the 129 HBPC programs that we had data on varied widely, ranging from 0% to 60% of HBPC patients using HT for any period during the same year. Forty-five HBPC programs were high users, 45 were intermediate users, and 39 were low users.
Results of the National Survey of HBPC Program Directors
We e-mailed a field survey (Table 1) to all 137 VA HBPC program directors to understand current practices for HT use. We received 41 responses (response rate = 30%). A wide variation in HT use was again noted among the respondents, with 13 of 41 reporting no HT use. Although the distribution of responses by level of HT use (high, intermediate, and low) is not available for this group, there were about 1,000 U of HT devices in use among the 41 HBPC sites, and the majority of them were using Health Buddy technology. Patients' HT responses were monitored by HT staff, and HT and HBPC staff mostly communicated by cosigning in the VA's electronic health record referred as Computerized Patient Record System (CPRS). Most locations reported that the HT staff did not attend weekly HBPC meetings.
Five themes emerged from the national survey regarding HT use in HBPC patients, based on survey comments: (1) staff acknowledgment of advantages of using HT; (2) patient usability challenges; (3) lack of timely and easy access of HT data to HBPC staff; (4) variation in communication patterns between the HBPC and HT teams; and (5) lack of role clarity and duplication of case-management functions between HBPC and HT teams.
Semistructured Interviews of High and Low HT Users
Eighteen HBPC program directors were interviewed, eight with high HT use, four intermediate, and six low HT users.
Evaluation of the interview data reinforced major themes from the national survey (Table 3). Patients' HT responses were monitored by HT staff. HT nurses made initial patient contact for outlier parameters and then HT or HBPC staff would follow-up as needed. HBPC staff was involved even when HT provided follow-up, leading to some redundancy and role confusion. Everyone used CPRS to communicate at a minimum by assigning HBPC staff as cosigner on alerts, monthly or quarterly notes. Communication challenges were posed by the HBPC staff who were often out in the field. Programs with higher percent of HT enrollees felt communication with HT teams was good or excellent. Attendance of HBPC weekly meetings by HT staff was uncommon and appeared to depend on the volume of patients and relative location of HBPC and HT programs in the facility.
Perceptions Regarding Drivers and Barriers of Home Telehealth Integration in Home Based Primary Care
Drivers of HT integration in HBPC included perception of utility of HT, including increased patient and staff support and HBPC provider efficiency, as well as organizational alignment of both programs. However, while some HBPC providers recognized the value of HT technology use with their patients, others felt it would not add value because they were already is such close communication with their patients in the HBPC program. Besides the barriers identified in the national survey regarding usability, data access, communication, and duplicative case management, additional ones surfaced, including HBPC staff perception of adequacy of the HBPC program and problems identifying appropriate patients.
Practices in HBPC Programs with High HT Use
We analyzed data to look for key characteristics in HBPC programs, such as interteam communication, enrollment, and collaboration practices, which might explain higher HT use. These are summarized in Table 4.
Key to Practicing Among Home Based Primary Care Programs Using More Home Telehealth
CPRS, computerized patient record system.
HBPC programs with high HT enrollees stated that HT staff attended HBPC team meetings to discuss dually enrolled patients, provide a report on HT use and data, and identify new candidates. Two programs said that HT staff attended meetings especially when there was a change in patient status or change in HT use. However, the high HT users endorsed using face-to-face meetings as needed, in addition to some form of frequent, consistent, formal, or informal communication—either in person or through phone, pager, e-mail, or CPRS. The low HT enrollees mainly used CPRS cosigning to communicate. The level and mode of communication between the teams appeared to depend on patient volume and relative staff location.
The high HT using programs reported screening all HBPC patients for HT eligibility, and all eligible patients willing and able were enrolled in HT. Two programs mentioned that “Veterans appropriate for HT” is a standing item for every HBPC weekly meeting and generates a couple of new HT patients weekly. One HBPC program assessed every new HBPC referral for HT suitability and places a HT consult, regardless of HBPC enrollment. Another HBPC program mentioned that all staff in both their HBPC and HT programs were oriented to the other program. In a couple of cases, both programs marketed together and shared consults.
There appeared to be structural factors associated with increased HT use: at few sites, the HBPC and HT programs shared a manager, and rarely, the HBPC program housed the HT program (both programs are usually distinct). Some programs reported that one assigned HT coordinator monitored responses for all HBPC patients, while another mentioned that an HBPC staff member monitored the HT responses.
Discussion
This exploratory study provides a glimpse into HT use in VA HBPC and indicates a wide variation of HT use. There is no standardization regarding communication across HT and HBPC teams. Two practices dominate among HBPC programs that have a relatively high number of HT users: more communication between the two programs with greater use of face-to-face and telephone modalities when there are more shared patients, and a system for identifying suitable patients for HT which usually includes screening all patients for HT use.
Important considerations for practice and education emerged which can improve HT integration in HBPC. These include educating both program members about the other program and its utility, generating guidance on appropriate patient selection criteria for HT based on contextual needs and capability, identifying strategies to enhance timely and meaningful information exchange between the two programs, and structurally and administratively aligning both programs.
Both HBPC and HT target populations are quite similar: both have older patients with significant chronic disease that lend themselves to close monitoring and case management. Therefore, many HBPC patients would be eligible for HT; however, older more frail patients may be less inclined to use technology. Although both HBPC and HT programs provide care coordination, HBPC assumes total management and primary care of its patients, while HT plays a supportive role, providing monitoring and care coordination without assuming care.
Care coordination starts with following up on abnormal HT alerts or change in status by contacting patients for further information through phone and timely sharing of this validated information between the two teams, to coordinate patient care. Thus far, there are no delineated processes for information flow, communication, or coordination between the two teams in response to abnormal HT data, raising concerns regarding role confusion and duplication of work and responsibility, as noted by other HT programs. 23 –25 Moreover, there is little current agreement on what constitutes a good handoff between HT and HBPC teams to support effective exchange of information and productive working relationships. 26,27 HBPC and HT teams that share more patients appear to have developed dependable relationships and improved communication over time, and perhaps, we can learn from their experience.
The VA system has not achieved seamless integration of CPRS with HT vendor data and currently requires that the stand-alone HT vendor systems be accessed through secure website by HT staff, who document data in a CPRS note at least monthly, or ideally for all abnormal responses; sometimes the HT notes are not timely and HBPC nurses deliver care without the support of the augmenting HT data to improve care decisions.
The VA nationally has been working tirelessly to make continuous advancement in development of robust mechanisms for automated and timely data export and integration from the HT vendor databases into CPRS, despite issues of interoperability, security, validity, etc. Achieving this will have significant potential to minimize—if not eliminate—the need for redundant data entry and telephone calls and help to better integrate HT services into the HBPC care-delivery processes. In addition, the VA information technology offers tools like instant messaging, e-mail, and secure messaging, which allow shared tasks and lists etc., to alleviate some of these communication challenges.
Provider support for HT depends largely on their perception of the utility of telehealth use and is key to getting their buy in, as shown by others. 25,28 Some HBPC staff expressed lack of conviction regarding the added benefit of HT to the close case management that HBPC provides. Moreover, evidence thus far on clinical and cost effectiveness of HT overall has been mixed and difficult to interpret, 29,30 and even less is known regarding HT in HBPC. While it is widely thought that HT should at a minimum offer some efficiency in terms of fewer telephone calls or in-person visits, convincing data to support these assumptions are currently lacking and are urgently needed. Furthermore, usability and adherence challenges with HT technologies noted previously in various settings, including Medicare home care 19 and VA non-HBPC patients, 31 may be amplified in this functionally limited HBPC population. 1
This exploratory study has several limitations. The national survey response rate was about 30%, thereby reflecting only a minority of HBPC environments and leaders. While not high, it is somewhat comparable to other national surveys for home care programs. 32 The semistructured interviews reflect the perceptions of a minority of HBPC environments and leaders, because program directors alone and not all HBPC staff from a few were interviewed. We stopped the interviews when we felt saturation had been reached, and no new themes were being uncovered. We identified some lack of clarity regarding the roles of the care coordinators from both programs; however, we did not examine whether this role confusion spills over to patients and caregivers.
Our study also has several strengths: not only do we use national data, we also use mixed methods to provide both breadth and depth in characterizing HT in HBPC and present data from HBPCs with varying HT use. Despite the fact that data presented are from 2011, and HT technologies used within and outside the VA are changing with rapidly advancing technology, the rules of engagement, communication, and interteam collaboration that are vital to successful integration are still valid.
HT-related capabilities and their integration into care-delivery processes present exciting opportunities to enhance HBPC care, by affording continuity and augmented information exchange to support enhanced care decisions. In the end, however, the individuals and medical conditions for whom HT use in HBPC is suitable need to be ascertained. 31 Moreover, much work is needed to characterize viable structural and process guidelines and models for workflow and productive information sharing to streamline the case management function to reduce redundancy between the two programs and to identify synergies that dual enrollment in HT and HBPC can achieve on efficiency, effectiveness, and cost of delivering HBPC care.
A lot more needs to be done for effective HT integration in HBPC. This article outlines some practices that can advance HT use in HBPC, but does not study impact of its use on patient or process outcomes. The challenges presented are not unique to the VA HBPC-HT collaboration 19,28 and add to a growing literature highlighting vital concerns about integration of HT with effective care models which need thoughtful evaluation and resolution. Importantly, these timely efforts may have crucial implications in the effort to serve more high-risk high-need patients, not only through VA HBPC alone but also through Medicare's Independence at Home program, which has shown promising results and tremendous cost savings thus far. 4,33,34 In fact, the new House and Senate extension legislation for Independence at Home calls for a specific analysis on the use of telehealth, including remote monitoring technology, by practices in the demonstration and its impact on outcomes. 35
Footnotes
Acknowledgments
This work was supported, in part, by a VA Office of Geriatrics and Extended Care's Patient Centered Alternatives to Institutional Extended Care Pilot, Transformational (T21) Initiative Award (546-4), a Merit Award (IIR 12–152) from the United States (U.S.) Department of Veterans Affairs Health Services Research and Development Program, on which Drs. Dang, Levi, Kinosian, and Edes are Co-Investigators, and by the Miami VA Geriatric Research Education and Clinical Center (GRECC). The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States government.
Authors' Contributions
Dang: concept, design, analysis, interpretation, and preparation of article. Ruiz: analysis, interpretation, and preparation of article. Klepac: analysis and interpretation of national VA DSS data. Morse: conduct, design, analysis, and interpretation of national HBPC survey. Becker: conduct, design, analysis, and interpretation of national HBPC data. Levy: preparation and revision of article. Kinosian: concept and interpretation. Edes: concept, interpretation, and preparation of article.
Disclosure Statement
The authors Dang, Ruiz, Klepac, Morse, Becker, and Levy report no conflict of interest. Dr. Kinosian is a HBPC provider; Dr. Edes has national responsibility for HBPC.