
Abstract
Background:
Telephone-delivered intervention can provide support in diabetes self-management to improve glycemic control. “eStar® program” is a telephone support platform for type 2 diabetes on glargine insulin treatment. Its objective is to help patients to perform insulin titration to reach target fasting blood glucose levels. Patients are contacted by trained nurses on a regular basis to adjust the basal insulin dose and reinforce the diabetes education. This study aimed to evaluate if eStar program was effective in helping patients reach their optimal insulin glargine dose within 6 months.
Materials and Methods:
An observational prospective study was conducted with type 2 diabetes patients who were initiating insulin glargine or requiring dose titration and were eligible to be included in the eStar program. Those participants who followed the program comprised the intervention group, while those who discontinued, the control group. The primary outcome was to evaluate if this program was effective in helping patients reach their optimal insulin glargine dose within 6 months. Secondary outcomes included changes in glycosylated hemoglobin (HbA1C), fasting plasma glucose (FPG), insulin dose, and body mass index after 6 months.
Results:
A total of 228 subjects [intervention group, 143 (62.7%); control group, 85 (37.3%)] were included in the study. A significantly greater percentage of patients in the intervention group reached their optimal glargine dose than in the control group (83.8% vs. 31.5%; p < 0.001). After 6 months, significant reductions in mean HbA1C levels were observed in both groups: 1.49% (p < 0.001) for the intervention group and 1.08% (p < 0.001) for the control group. Furthermore, a mean reduction in FPG between group was achieved (34.96 mg/dL; p < 0.001).
Conclusions:
The eStar program is an effective way to help patients reach their optimal insulin glargine dose, besides improving their glycemic control.
Introduction
Given its prevalence, diabetes is one of the most serious health emergencies of the 21st century, with 382 million people suffering from the disease worldwide in 2013, a number which is expected to increase to 592 million by 2035. 1 Type 2 diabetes is a chronic and complex disease that requires continuing medical care, nursing intervention, and ongoing patient self-monitoring to prevent acute complications and reduce long-term complications. 2
Insulin is commonly prescribed to treat uncontrolled diabetes 3,4 if optimized oral antidiabetic drugs (OADs) and lifestyle interventions are unable to maintain blood glucose at target levels. Patients are started on a low dose of insulin that is adjusted according to their blood glucose levels until they reach an optimal dose that best controls their glucose levels. Insulin titration normally occurs in several face-to-face encounters with a physician, as generally one titration is not enough to reach glycemic control. 5 Attending multiple appointments can be burdensome for patients, as they are required to miss work hours, arrange transportation to the clinic or childcare, etc.
Suboptimal adherence to the recommended diabetes treatment and self-care management is a well-recognized problem 6 –9 with implications for the successful achievement of clinical targets, leading to severe consequences in patients with uncontrolled diabetes. 10 Patient education in disease self-management has been shown to be an essential part of diabetes treatment to improve glycemic control. 11 A wide variety of strategies and techniques can be used to provide adequate education in diabetes self-management, offered individually or in a group, 12,13 face-to-face, or remotely. 14 –17 Several studies suggest that patients with diabetes do best when they are engaged in self-management programs, such as telemonitoring, showing significant reduction in glycosylated hemoglobin (HbA1C) and complications. 18
Despite the increased treatment options and advances in technologies, the inability to reach the desired target in diabetes management is an important issue for healthcare providers. The eStar® is a telephone support program, with an additional Web-based platform, complying with all security rules and data privacy protection, for subjects with type 2 diabetes who are currently on treatment with insulin glargine. Physicians introduce the following patient data on the Web: insulin dose, glycemic target, and contact details. Then trained nurses, who have access to the Web, contact the patient and deliver the telephone support. It is intended to help patients to perform insulin titration and reach target fasting blood glucose levels. The aim of the study was to evaluate whether the eStar program was effective in helping patients reach their optimal insulin glargine dose within 6 months.
Materials and Methods
Study design
This was an observational prospective study to assess the effect of a telephone support platform for type 2 diabetes—the eStar program—on insulin glargine treatment.
Study participants
Between June 2013 and August 2015, adult subjects with a diagnosis of type 2 diabetes who were initiating insulin glargine or requiring the titration of an existing insulin glargine dose were eligible to be included in the eStar® program, after signing the informed consent form. The intervention group included participants who followed the program. Those who discontinued the follow-up after the first telephone call, without any recommendation given in that call, comprised the control group. For both groups, treatment followed routine clinical practice and was in no way affected by participation in the study.
A glycemic target was determined by physicians for each patient. The optimal insulin glargine dose was defined as the dose at which a patient achieved at least three fasting blood glucose values within the predetermined glycemic target.
The eStar program intervention
The eStar program consisted of weekly telephone sessions until the patient reached the glycemic target. After that, calls were scheduled monthly during a 6-month period. The sessions were delivered by diabetes nurse educators that had neither face-to-face contact with patients nor access to their medical records. The nurses had access to the Web-based platform where glycemic target and current insulin dose were registered by physicians. Patient's needs concerning insulin administration and hypoglycemia management were established based on a nonvalidated questioner about diabetic education. During each session, patients received tailored education and expert advice on titration of their insulin glargine dose to reach their target fasting plasma glucose (FPG) levels, as well as other aspects related to diabetes, such as the importance of glucose self-monitoring or diet. Furthermore, patients had a free 24-hour telephone service to solve their doubts.
Data were collected at initiation of the eStar program (baseline) and after 6 months.
Study outcomes
The primary outcome was whether patients reached their optimal insulin glargine dose within 6 months. The secondary outcomes were changes in HbA1C, FPG, insulin dose, and body mass index (BMI) at 6 months.
Statistical methods
A descriptive analysis of the study variables was carried out using measures of central tendency and dispersion for quantitative variables and valid frequencies and percentages for qualitative variables. To analyze statistically significant differences between quantitative variables, we used the t test or the Mann–Whitney U-test, according to the distribution of data; for qualitative variables, we used Fisher's exact test or the chi-square test. The significance level was set at p < 0.05, and all statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS)® software version 23.0. (IBM Corp. Released 2015. IBM SPSS Statistics for Windows, Version 23.0. Armonk, NY: IBM Corp.)
Results
Participants
A total of 228 subjects were included in the program, of whom 143 (62.7%) comprised the intervention group and 85 (37.3%) the control group. Mean age of the overall study population was 62.8 ± 13 years, and 60.1% of participants were men.
At baseline, most patients were receiving OADs exclusively (53.5%) followed by those on OADs+insulin (26.8%) and insulin only (10.1%).
Outcomes
Data on glargine dose titration were lacking for 13 subjects. Thus, a total of 215 participants were considered for the analysis of optimal dose titration: 142 in the intervention group and 73 in the control group. The number of participants who reached their optimal insulin glargine dose was higher in the intervention group than in the control group [119 (83.8%) vs. 23 (31.5%); p < 0.001], with an odds ratio of 11.25 (95% confidence interval [CI], 5.78–21.89). Table 1 shows the changes in the study parameters for both groups.
Clinical Characteristics of the Study Participants
BMI, body mass index; FPG, fasting plasma glucose; HbA1C, glycosylated hemoglobin.
Six months after completing the study program, significant changes in mean HbA1c levels were observed: −1.49% (95% CI −1.21 to −1.77; p < 0.001) for the intervention group and −1.08% (95% CI −0.69 to −1.48; p < 0.001) for the control group (Fig. 1). Other differences between the groups at 6 months were observed in FPG, with a mean reduction of 34.96 mg/dL (95% CI 18.21–51.72) (p < 0.001). No differences in BMI were observed between the groups.

Evolution of HbA1C levels following 6 months of the e-Star Program.
Considering previous treatment, patients who were initially on OADs reached better glycemic control in both groups (Table 2). In addition, a higher number of patients receiving OADs previously reached their optimal glargine dose in the intervention group (47.8% on OADs vs. 29% on OADs+insulin and 7% on insulin) (Fig. 2).
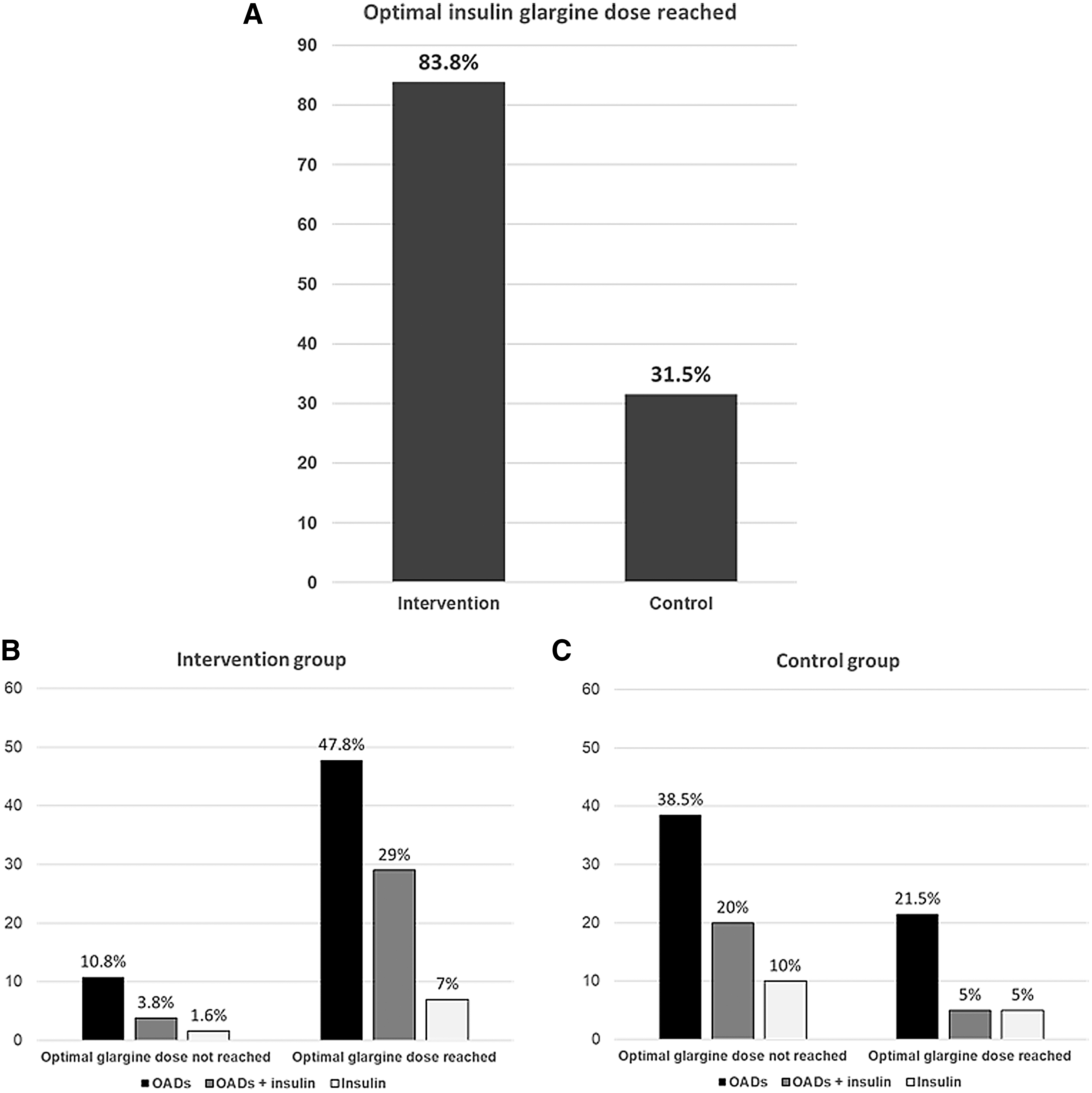
Optimal glargine dose achievement.
Differences in Insulin Dose and Glycemic Control Based on Previous Treatment
OADs, oral antidiabetic drugs; SD, standard deviation.
Discussion
Our findings support and extend previous studies of telephone-delivered interventions conducted among subjects with type 2 diabetes.
Consistent with existing research, 19 –21 the intervention contributed to improvements in glycemic control, with lower HbA1c levels in the intervention group after 6 months of initiating the eStar program. Previous studies have shown that subjects with diabetes tend to manage their chronic conditions better after receiving follow-up phone calls from a healthcare provider. 22 The longitudinal randomized trial led by McMahon 23 to investigate whether telephone or online care management improves diabetes-related outcomes over time, compared with usual care supplemented with internet access and training, concluded that there was a substantial improvement in HbA1C levels over a 1-year period with online, telephone-based care management, and Web training in patients with poorly controlled diabetes.
This result was consistent with previous findings reported by Walker et al., 16 which aimed to compare the effectiveness of a telephone and a print intervention over 1 year to improve diabetes control in subjects with HbA1C ≥7.5%, showing that telephone interventions led by health educators resulted in a significant, although moderate, decline in HbA1C of 0.23% ± 0.11% compared with a rise of 0.13% ± 0.13% for the printed material group. After adjusting for baseline HbA1C, sex, age, and insulin use, the difference in HbA1C between both groups was 0.40% (95% CI 0.10–0.70; p = 0.009). In addition, the study led by Stone et al. 24 demonstrated that patients receiving home telemonitoring, coupled with active care management, showed significantly greater reductions in HbA1C at 3 and 6 months compared to subjects who received monthly care coordination telephone calls.
Our results also showed that a greater percentage of patients in the intervention group reached their optimal insulin glargine dose compared to the control group, with patients included in the eStar program being 11.25 times more likely to reach their optimal insulin glargine dose at 6 months' follow-up in comparison to those who discontinued the program at some point. This result agrees with previous literature. In a pilot study evaluating an intervention for patients requiring insulin glargine titration in the outpatient setting, it was shown that simple SMS text messaging and weekly titration phone calls were effective ways to help patients reach their optimal insulin glargine dose. Within 12 weeks, a significantly greater proportion of patients in the intervention arm reached their optimal insulin glargine dose compared to patients in the usual care arm (88% vs. 37%; p < 0.001), without an increase in the number of hypoglycemic events. 25
Different studies have shown that most telemedicine strategies can be effective in reducing HbA1c in patients with type 2 diabetes compared to usual care, with mean difference ranging from 0.37% and 0.71%. 26,27 This article reinforces the role of telemedicine in diabetes.
Among the limitations that need to be mentioned are the following: (1) The relatively small sample size. This was based on the constraint of the observational period. Nonetheless, the number of patients included is representative of the volume of consultations performed. A longer period of observation would probably have better consolidated the data but would have required a longer period and greater resources, (2) FPG levels were different between the two study groups at baseline, so the two groups were not homogeneous; and (3) Data on adverse events such as hypoglycemic events were not systematically solicited nor were reported events assessed.
Conclusions and Implications for Practice
A telephone-delivered intervention program led by trained nurses is an effective approach to help patients reach their optimal insulin glargine dose, contributing to improvements in their glycemic control and maintenance of self-management of their disease.
Footnotes
Acknowledgments
The authors thank Ana López-Ballesteros and Antonio Torres-Ruiz at Dynamic Science S.L. for their medical writing and editorial support.
Disclosure Statement
No competing financial interests exist.