
Abstract
Introduction:
Nonavailability of emergency healthcare services in mountainous, isolated, and sparsely populated regions is a universal problem. In a first of its kind initiative, Tele-emergency services (TES) was provided in Keylong and Kaza in Himachal Pradesh in Northern India, at an altitude of 3,353 meters with temperatures of −30°C during winter months.
Methods:
Existing rooms in regional hospital (Keylong) and community health center (Kaza) were converted into tele-emergency centers by connecting them, to a state-of-the-art emergency department at the Joint Commission International-accredited Apollo Main Hospital at Chennai, 2,925 km away. Training was carried out at both ends. Average turnaround time for an emergency teleconsult was less than 12 minutes. Tele-ECG, Spirometry, and Point-of-Care Diagnostics for blood biochemistry were made available.
Results:
In the first 35 months, 753 teleconsults were given in the 24/7 TES, out of a total of 10,213 teleconsults constituting 7.4%. Out of a total of 6,442 telelaboratory tests, 431 tests were done in an emergency setting constituting 6.7%. Of the 16 cases of myocardial infarction remotely diagnosed, 4 were thrombolysed through telementoring. Of seven patients with Supra Ventricular Tachycardia, six patients were stabilized through electrical cardioversion and one through chemical cardioversion through telementoring. Ten deaths were documented, of which one occurred at the site. One hundred ninety-six were stabilized and transferred to higher centers. Thirteen required helicopter evacuations. Detailed analysis revealed that the total average cost for a single emergency teleconsult during this period was US$208.
Conclusions:
Preliminary analysis confirms that delivering TES in inhospitable terrains in a Public Private Partnership mode is doable and is welcomed by the community.
Introduction
The Department of Health & Family Welfare, Government of Himachal Pradesh realized that due to climatic conditions and isolation of most regions, providing conventional affordable quality healthcare would be difficult. Operational challenges in setting up telemedicine services in such areas and attitude of healthcare providers in Himachal Pradesh toward remote healthcare, have been documented earlier. 1,2 It had been pointed out that shortage of healthcare providers made availability of 24/7 services impossible.
A tele-emergency services (TES) was planned as a value added service, to provide sophisticated tele-triage services, reducing unnecessary transfers and managing patients in the remote casualty, under the guidance of an experienced Chennai-based emergency medicine specialist. In other cases, following stabilization, transfers to secondary centers 200 kms away were facilitated. Government health facilities at Kaza and Keylong (Fig. 1) were chosen for the initial pilot study on the TES.
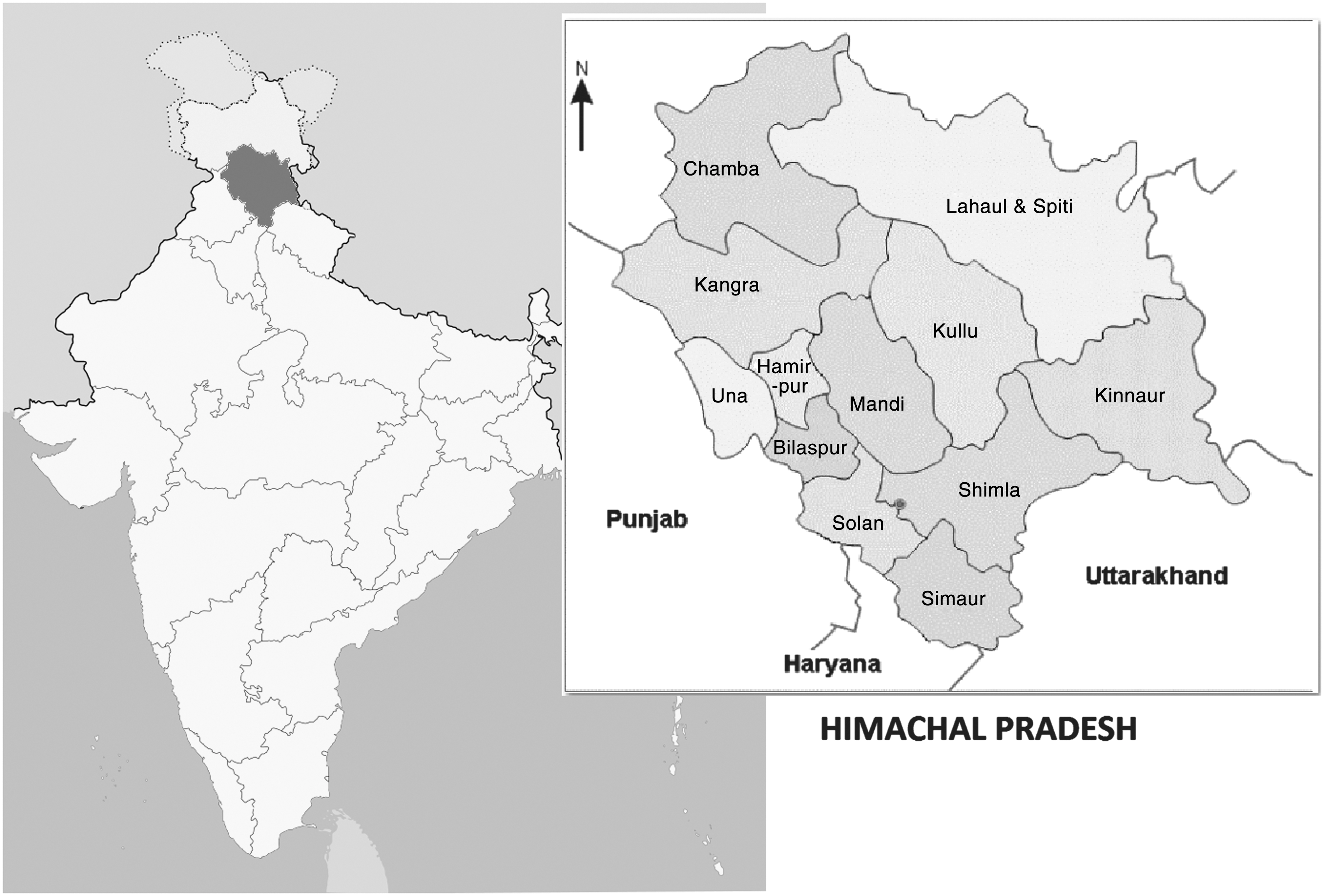
Location of Himachal Pradesh and its districts.
Challenges Peculiar to Establishing TES
Lahaul and Spiti, covering 13,835 sq km, has a population of 34,000. The nearest secondary care hospital, is 200 km away. Landslides and hostile weather of −30°C made transport difficult. Transportation through helicopter was expensive and necessitated time consuming multiple levels of approvals. A program management approach, including a need assessment study, budgeting, and drawing up specifically defined service level agreements, was adopted. The implementation component included training, capacity building, weekly and monthly project reporting, and optimized capacity utilization. Major change management issues were faced with the local staff initially. Making available drugs prescribed through the TES was difficult, but this is being addressed. If an ultrasound or CT scan was required, the patient was transferred to the higher level center. Making sophisticated urban teleconsultants prescribe generics for the limited medicines available and avoiding sophisticated investigations was also difficult.
Risk of nonutilization of TES was addressed by having a full-time employee in each center dedicated for community outreach. Mass communication with customized, cost-effective, need-based information modules, were deployed to ensure that the population became aware of the TES. A rigorous detailed Standard Operating Procedure was formulated. Nonfamiliarity with hardware, software, and reluctance to use tools supplied was addressed by training, retraining, and ensuring constant skilling and upskilling. Learning, relearning, and unlearning were carried out. Risk of nonavailability of Hindi-speaking teleconsultants in real-time and for emergencies was mitigated by having English speaking translators at the remote end. Risk of interrupted power supply was addressed with dedicated generators. Subsequently solar power was made available. Risk of absence of human resources was reduced by having additional staff.
Bandwidth Challenges During Implementation
Dedicated, customized, highly subsidized Very Small Aperture Terminal satellites were provided by BSNL 3 –(largest network provider of the Government of India) VSee, a HIPAA-compliant telehealth application, is being used for video conferencing, keeping patient data secure with 256-bit AES encryption. Partnering with e-KSS VSee has provided peer-to-peer low-bandwidth video that works over satellite broadband and 3G networks in the Amazon. 4 Minimum bandwidth, compatible hardware, and software were deployed. From a clinical patient management perspective “Just enough” bandwidth always available was better than unreliable ideal bandwidth.
TES Implementation Process
The intensive 3 months training for remote location staff, carried out at Chennai for the Telehealth Services program, included exposure to clinical emergencies. Presenting a clinical problem, in an emergency situation, through video conferencing, management information systems, reporting, and troubleshooting Internet connectivity problems, was taught. A well-integrated teleconsultation unit with remote diagnostic devices (digital 12-lead ECG, Spirometer, 5 Stethoscope, Point-of-Care Diagnostics [POCD]), and seamless Internet connectivity of 512 Kbps, enabled TES implementation. X-ray films developed at the remote casualty center (digital X-ray machines are not available) were scanned and sent.
The TES system blended seamlessly with the government-provided limited emergency services theoretically available. The emergency setup at the remote ends was, to the extent possible, in accordance with Joint Commission International (JCI) prescribed protocols. Prescribed emergency medicines, medical disposables, emergency mobile cart, hardware/software, and video conferencing systems were made available at Kaza and Keylong. With support of a well-trained telehealth facilitator, available around the clock, patients were able to get teleconsultations with an Apollo Emergency Department (ED) consultant at Chennai 24/7 (Fig. 2).

Emergency Department consultant at Chennai connected to TES at Keylong. TES, tele-emergency Services.
The state-of-the-art ED, recognized as a training center for emergency medicine, has 25 beds, 50 nurses, and ventilators and annual intake of 19,000 patients. Challenges faced by tele-emergency consultants at the Apollo Main Hospital were many. Foremost was obtaining a reliable history from the remote patient or the caregiver. Most patients spoke the local dialect. To the clinician at the other end, English was a foreign language. As digital imaging was not available, hard copy images had to be photographed and sent electronically. This had limitations.
The doctor at the remote end, having to interact with different teleconsultants, was unable to establish specific rapport. Presence of a doctor at the remote end was insisted upon. All requests for emergency teleconsults needed the remote doctor's approval. Challenges at the tele-emergency center in Kaza and Keylong (Figs. 3 and 4) were also many. Although identified and corrective measures initiated, some still do exist. Lack of continuous reliable power is a concern. The Uninterrupted Power Supply backup is only for 2 h in summer and 30 min in the winter. Diesel for generators was not always available. An additional solar power backup has recently been obtained. The only radiology technician was also not available after 4 pm or on holidays. Ultrasound is not available. Blood was often not available.

Tele-emergency Center at Keylong.

Tele-emergency Center at Kaza.
A Web-based electronic medical record (EMR)—a Comprehensive Electronic Patient Health Information System (CEPHIS) was used for documentation. This included demographic, patient data, clinical and family medical history, examination reports, and investigations. The customized software enabled import and export of complete patient records, including images and files. The solution, catering to multiple medical specialties, offered “store-and-forward” and “real-time” teleconsultation, providing its users the facility of generating and viewing various reports.
Appointment scheduling, live chatting, and interfacing with telediagnostic medical equipment was also possible. Personal interaction by telemedicine coordinators on both sides ensured that traditional human touch continued. An experienced emergency medicine specialist from Apollo Main Hospital Chennai telementored the Casualty Medical Officer/duty nurse at Kaza and Keylong to provide initial medical support to stabilize the patients.
Cost Effectiveness
Literature on economic aspects and financial viability of TES are few. MacKinney et al. 6 point out that a “business case” from the literature, supported by objective data and/or qualitative judgment, to implement or continue TES cannot really be relied upon as each TES is truly unique. Savings in a tele-emergency setting primarily accrue when physician ED backup and physician ED staffing costs are substituted. TES includes remotely monitoring patients. It has been stressed that start-up costs and training time costs need to be computed in a cost benefit analysis with its implication on healthcare dollars when TES is deployed in a trauma/ambulance setting. 7 However, as TES enables paramedics to initiate consultations with emergency physicians enabling treatment in non-life-threatening cases, there could be a financial savings. 8
Although there was no information available on the number of emergency ambulance transfers before the introduction of the TES, only 83 emergency ambulance transfers were done (from both the centers) over the duration of 35 months, besides 14 emergency helicopter evacuations. It is estimated that during this period many ambulance and helicopter transfers were avoided resulting in financial savings and reduced carbon print. A survey of 140 users of TES indicated that considerable effort, time, physical discomfort, and emotional stress were reduced, besides not incurring out-of-pocket expenses of about US$20,000. Nontangible benefits such as satisfaction and happiness that a caring government has facilitated quality accessible healthcare round the clock and free of cost cannot be quantified.
The total costs incurred for setting up the TES, including the initial capital expenditure, the recurring operational expenditure (salaries, connectivity charges, consumable charges), and the program management charges (all for the TES component), were computed. This was divided by the number of patients who utilized the TES. The cost per patient in the first 145 weeks was US$208. However, if one takes into account the average yearly depreciation on the capital expenditure, average annual cost escalation on operational expenditure, and the expected percentage increase in annual patient footfalls, when distributed over 5 years, the cost could come down to US$120 in the fourth year with a 5-year average of US$143. Although higher, considering that there is no other alternative for providing emergency quality accessible healthcare in these isolated areas, the prices are not unreasonable.
The Clinical Story
Figure 5 shows the age and gender distribution. Figure 6 shows provisional clinical working diagnosis. Due to infrastructure limitation, a specific definite diagnosis could not be made in all patients but presenting symptoms were managed. Utilization of TES in different specialties does not reflect the incidence and prevalence of these clinical conditions in the community, as there are other compounding factors. One hundred nine cases were probably not real “emergencies.” Attempts to discourage use of a 24/7 facility, when not really indicated, could not be enforced all the time. One hundred thirty-seven were advised to be transferred to a higher center, out of which 134 were actually transferred. Two did not want further treatment and one was admitted in the local ward, not wanting escalation of treatment.
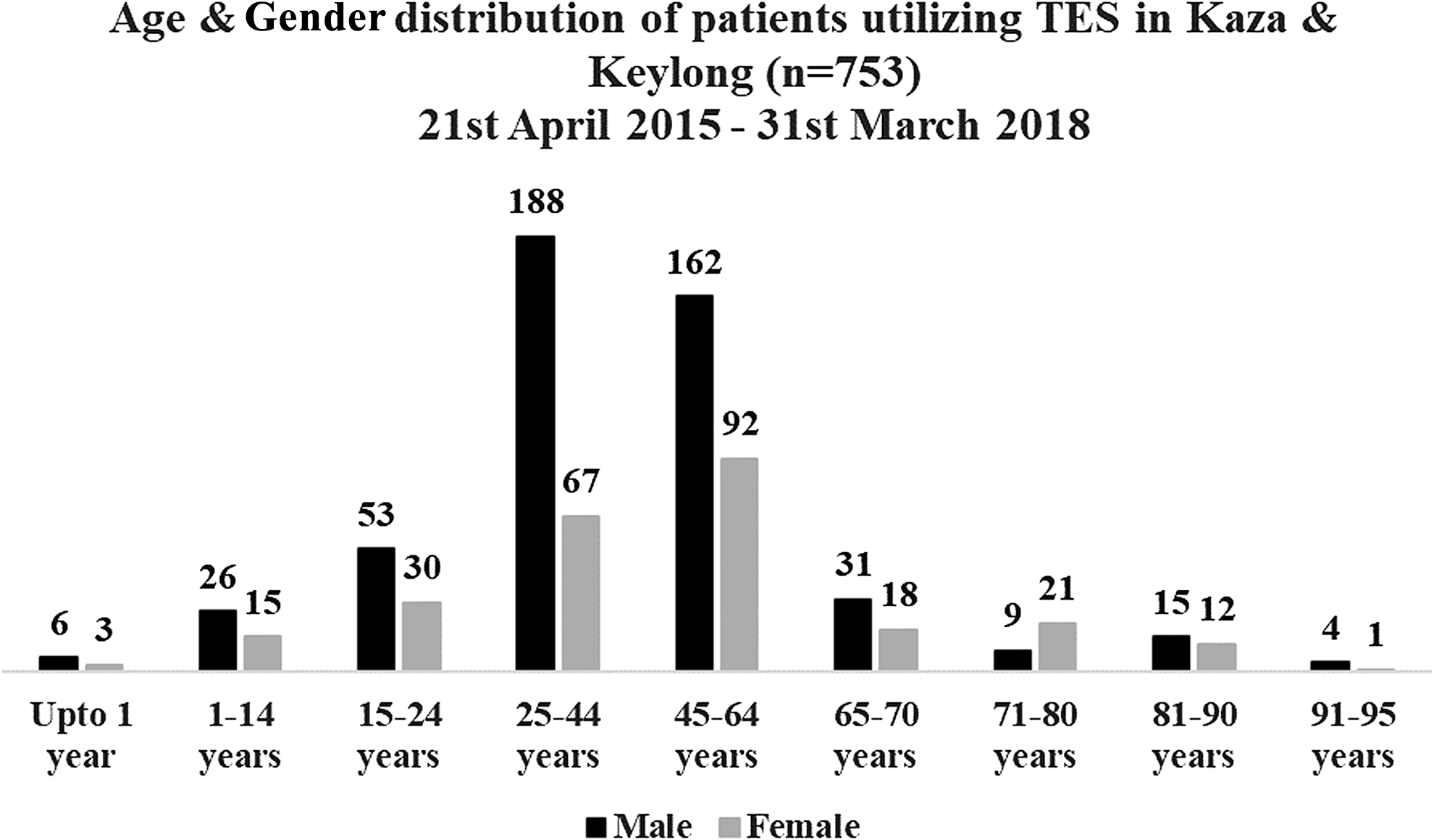
Age and gender distribution of patients utilizing TES.

International Classification of Diseases, classification of TES Diagnosis.
Follow-up was attempted and only 140 responded. The follow-up was 1–145 weeks. This revealed that 10 patients had died at various intervals. Figure 7 gives details of the cause of death. Figures 8 – 10 are examples of a few patients treated. Figure 11 is a rare example of telementored electrical cardioversion.
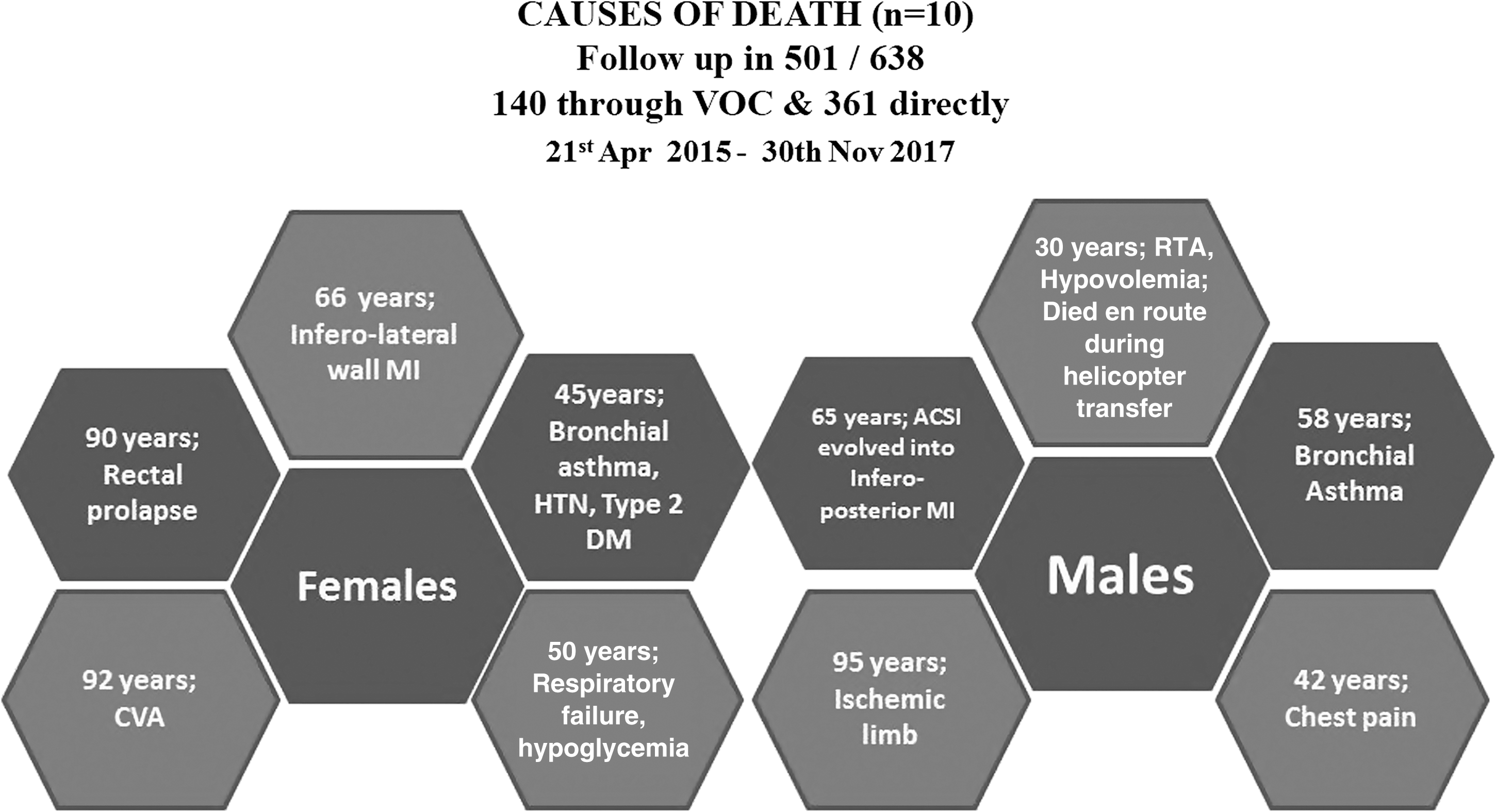
Causes of death among patients attending TES.
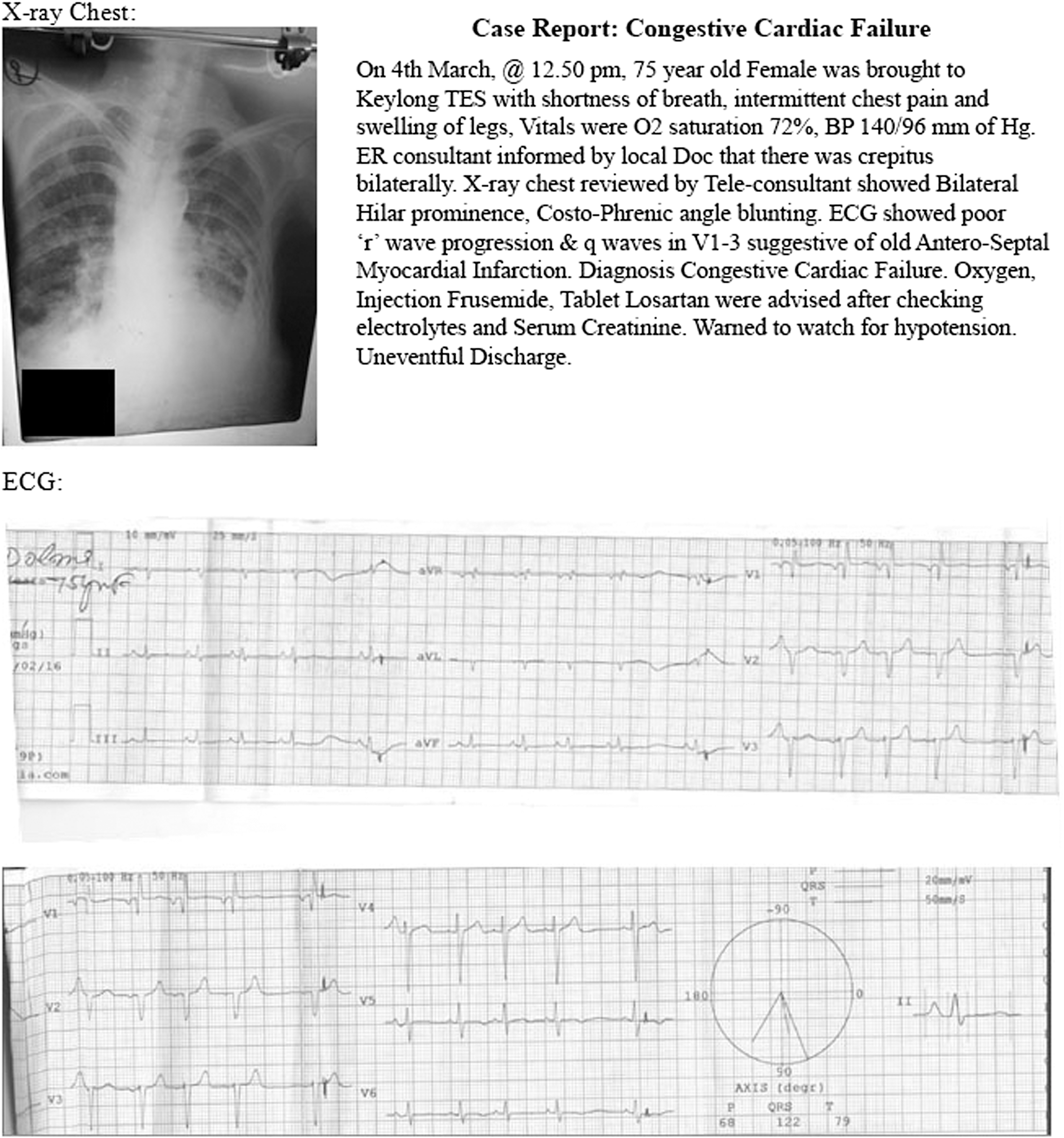
Clinical illustration.

Clinical illustration.

Thrombolysis through telementoring.
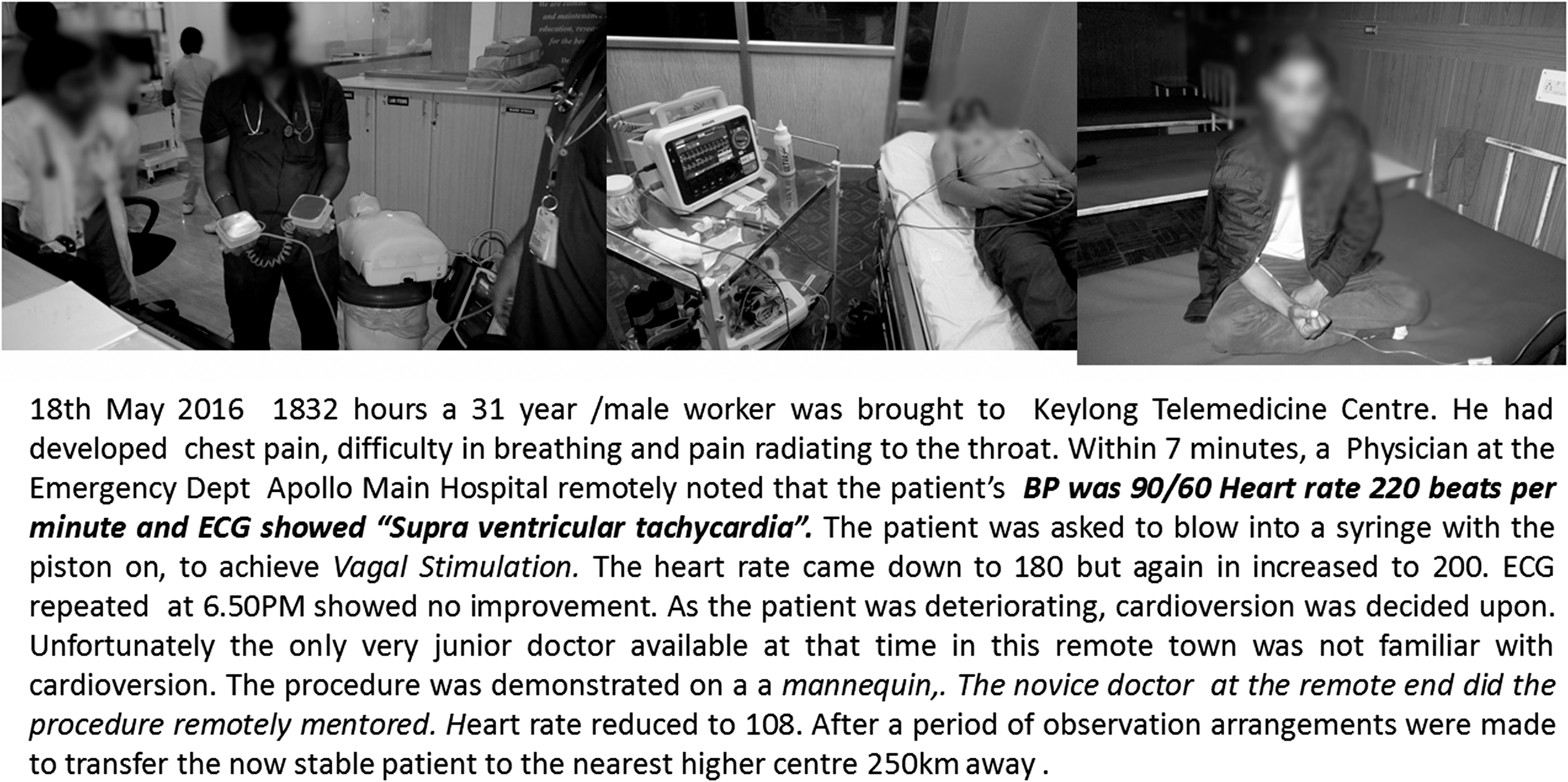
Cardioversion through telementoring.
Utilization of TES
A detailed analysis was done to determine if there was any particular time slot or day of the week when the 24/7 services were utilized more (Figs. 12 and 13). Due to initial software glitches time of presentation was unavailable in 51 patients. It was surprising that contrary to expectations, there were only 8 patients who utilized the service between 9 pm to 9 am, although the services were available. Lack of awareness, lack of transport, and the very harsh weather conditions at this time could have been contributory factors. Some recordings at this time could have been missed. Footfalls at the TES were almost the same on different days of the week. As expected, footfalls were less during the harsh winter season, but were still significantly more than the visits to the government hospital in the previous years.

Time of consultation at TES. TES, tele-emergency services.

Utilization of TES based on day of week. TES, tele-emergency services.
The monthly and seasonal footfalls are given in (Figs. 14 and 15). Despite an elaborate Voice of Customer (VOC) follow-up system in place, VOC follow-up could be obtained only in 140. A rating of 9–10 was given by 68% and none gave below 7, when queried about satisfaction levels, system in place, and the impact of the TES.
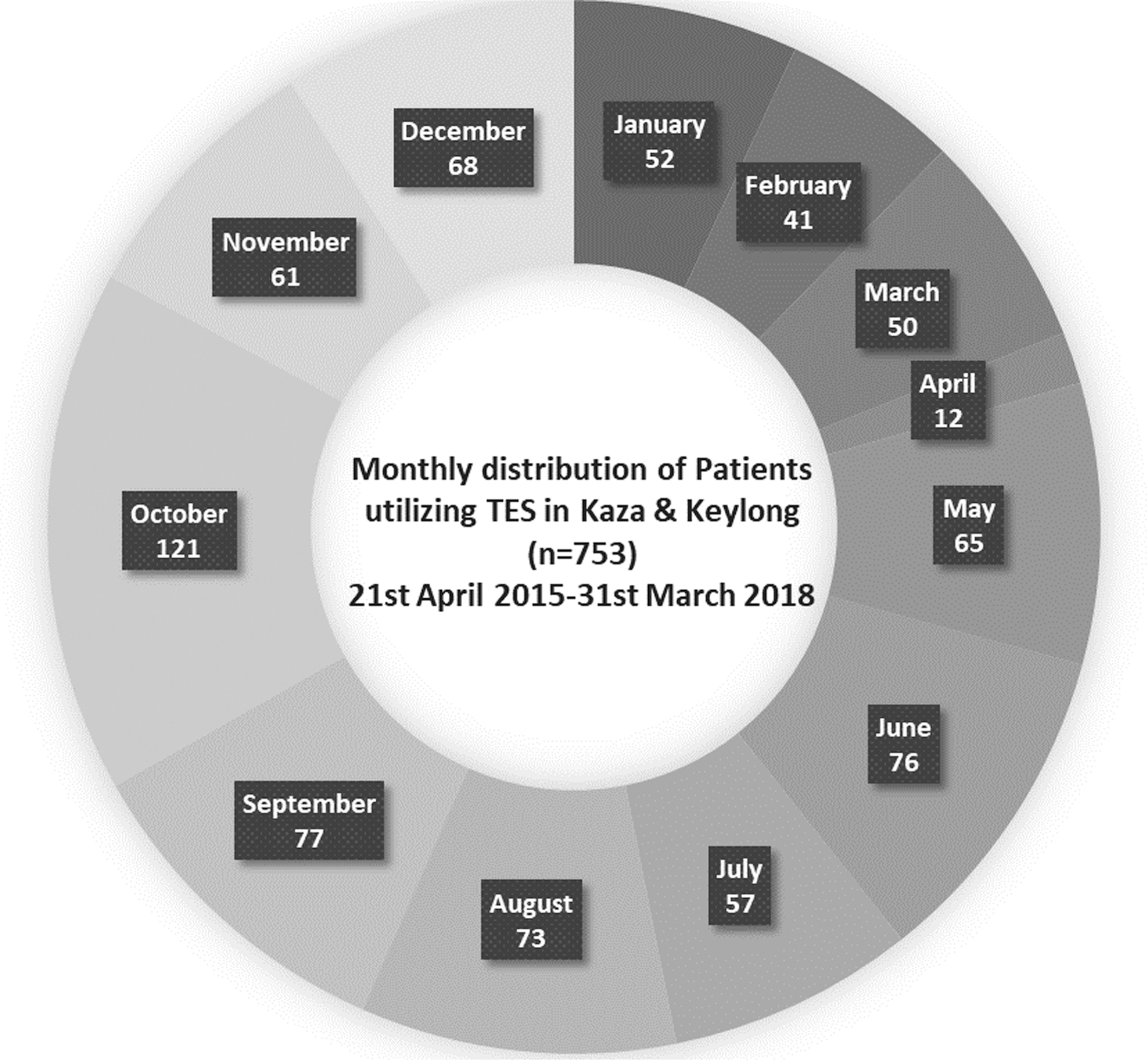
Utilization of TES in different months. TES, tele-emergency services.

Utilization of TES in different local seasons. TES, teleemergency services.
Telelaboratory Services
Using an U.S. Food and Drug Administration-approved POCD Kit, blood biochemistry, including lipid profile, LFT, RFT, HbA1C, Hb, and PCV, tests were made available in later December 2015, 8 months after the TES was initiated. The local staff were virtually trained and soon became adept at using the kit (Fig. 16) in an emergency setting. This resulted in better clinical management. Figure 17 shows distribution of the laboratory investigations done through the TES.

Using Point-of-Care Diagnostics.

Point-of-Care Diagnostics investigations in TES. TES, tele-emergency services.
Review of the Literature on TES
A thorough search was done to review all articles primarily detailing TES, published in peer-reviewed journals, in English. Data bases reviewed included PubMed (Medline), Science Direct, and Scopus. The search strings were combined using “AND” and “OR” for a better search strategy. Duplicates were removed. The titles, keywords, and abstracts were used as a preliminary filter with the agreed to selection criteria, to identify relevant articles. Full texts of relevant articles were reviewed. Additional relevant articles were also extracted from the reference lists of the selected articles. Inclusion and exclusion criteria were setup following rigorous discussion and brainstorming among the authors. A synopsis of the salient points was used in the “Discussion” section.
TES have been provided in rural areas. 9 Fairchild, 10 while reviewing the literature, pointed out that analysis of telehealth applications in the United States revealed that 32% of 4,727 reporting hospitals were using at least one type of telehealth service, and TES are utilized in ∼8% of EDs. A significant increase in the rate of ED admissions to rural hospitals with TES, betterment of quality of emergency care, and retention of physicians in rural areas have been reported as additional benefits of a rural TES. 11 As in this study, other TES have used immediate and synchronous audio/video connections to connect rural low-volume hospitals and an urban “hub” ED. 12 Martínez et al. 13 demonstrated that 9 months after setting up a telemedicine system in the Amazon region of Peru, consults increased from 3 per month per facility to 23. Of 205 emergency transfers from 39 health facilities, teleconsults saved 28%.
Voice and e-mail communication via VHF radio were feasible and useful for rural telemedicine in these inhospitable terrains. TES has been shown to improve clinical quality, expand the care team, increase resources during critical events, shortening time to care, and improving care coordination. There have been reports on medication errors during TES provided to rural EDs. 14 In the United States, inconsistent reimbursement policies and cross-state licensing barriers hinder tele-emergency implementation. Potter et al. 15 have reported that access to a TES improves the work environment, facilitates physician recruitment and retention, enhances physician confidence, provides educational opportunities, easing burden, and supplementing care. These authors have not mentioned patient “delight,” which in our opinion was the most striking. To achieve this, the manner in which the individuals at both ends interact with an already tense patient is critical. Nestel et al., 16 with evidence-based patient-centered interviewing, have confirmed the importance of telephone conferencing skills during remote clinical interactions.
Most ED visits in the United States are for minor medical conditions that can be diagnosed and treated virtually. 17 Our experience is similar. With this in mind, board- certified emergency physicians are expanding their technology tools with mobile apps and home-grown EMRs. Telemedicine technology for practicing emergency physicians has been discussed to create the much needed awareness and stimulate the ER community. 18 Westbrook et al. evaluated the effect of TES on patient management and outcome. They also investigated clinicians' perceptions of the impact of the system on care provided and on their work. This included changes in patterns of management [admission, discharge, or transfer], treatment times, number of procedures and outcomes, hours on ventilation or in intensive care, and length of stay. 19
In 1999, Brennan demonstrated that there was no difference in the 72-h return visits, need for additional care, overall patient satisfaction, and time from admission to discharge in a randomized controlled study of patients, presenting to the ER who used TES. 20 We endorse this view. TES was launched at UC San Diego Health System's ED purely to address crowding and decrease patient wait times. Cameras were used to bring on-call doctors outside of the hospital to the patient in need. 21,22 The UPMC Teletrauma Program has demonstrated that patients can receive timely treatment close to their homes simultaneously avoiding delay in timely treatment by avoiding transfer to a higher level trauma center farther away. 23
TES provides an opportunity for more timely access to acute care and specialist healthcare providers supporting patients who require immediate assessment and treatment. 24 Ward et al. in a study of 60,193 ED encounters over a two-and-a-half-year period, showed that TES were used in only 3.5%, mostly in patients requiring transfer or with circulatory or trauma issues. Rapid transfers were facilitated using recommended clinical protocols particularly for patients needing serious and/or urgent attention. 25 Lambrecht, 26 however, reported in 1997 that out of 190 teleconsults, 45 (24%) were for the emergency physician. A study of 161 case records from an ED in a rural hospital revealed that among those using TES, 7.5% were identified as potentially avoidable transfers. 27 Although none of these reports is comparable with our situation, our study reveals that TES utilization was 8.3% of all teleconsultations.
TES has been deployed in special situations. They include deploying a Tele-Airway Management System for intubations of actual patients in a hospital ED, 28,29 tele-emergency mental healthcare, 30 tele-emergency for ICU, 31,32 tele-emergency for tertiary cardiology care, 33 tele-emergency for pediatric critical care, 34,35 trauma, 36 short-term correctional facility, 37 and older adults residing in senior living communities. 38
While racial and ethnic disparities exist in other components of stroke care, Lyerly 39 reported that TES levels the playing ground for minority patients in the availability of acute stroke care. Telecardiology intervention in a TES unit has significantly lowered the Major Adverse Cardiovascular and Cerebral vascular Events rate. The Tele-ECG group had a lower mortality rate. In-hospital tele-ECG triage and interventional cardiologist activation reduced door to balloon time) and was associated with improved late clinical outcomes. Our small experience of telecardiology intervention endorses this report from Chen et al. 40
Conclusion
Objective assessment of user satisfaction is under way. An interim interview of 140 patients who utilized the TES revealed that 72% were “delighted” with the TES provided 41 (Ref. 41 due to patient confidentiality, only a single edited VOC audio has been provided in the public domain). A detailed literature search did not reveal any published data on the establishment of a dedicated TES program in mountainous isolated areas. This program is also unique in that it is probably the first TES program established in a public private partnership (PPP) mode. Emergency Ambulance Services in Tamil Nadu in southern India and mobile hospitals in Uttaranchal in northern India are examples of providing access to regular face-to-face emergency services in a PPP mode. 42
The conclusions drawn from the observations in this study cannot ipso facto be generalized and extrapolated to all TES. Operational details have to be customized, depending on specific requirements and availability of resources and infrastructure. While there is no specific bias in this study, inadvertent culture-specific preferences may have been deployed. The authors believe that they have demonstrated that delivering TES in a PPP mode is doable even in an emerging economy, under difficult conditions.
Footnotes
Acknowledgments
The field workers at Kaza and Keylong Sonam Lamo, Thinley Tsomo, Lamo Butit, Tanzin Yeeyong, Ranjana, Kewal Kishan, Chhering Dolma, Tanzin. Mohan Lal Shashini, Dr. Naresh, Dr. Paramesh, Angdui Norbu, and Balakrishnan helped in different ways. Permission has been obtained from patients and staff to use photographs in which they appear. Shiny, Delci, and Dr Brindha also helped in collecting the data. We are thankful to Ms Sangita Reddy, Joint Managing Director; Dr Prathap C Reddy, Chairman Apollo Hospitals; and Mr. Vineet Chawdhry, Chief Secretary, Government of Himachal Pradesh for the encouragement given.
Disclosure Statement
No competing financial interests exist.