
Abstract
Background:
Adolescents at risk for anaphylaxis are a growing concern. Novel training methods are needed to better prepare individuals to manage anaphylaxis in the community.
Introduction:
Didactic training as the sole method of anaphylaxis education has been shown to be ineffective. We developed a smartphone-based interactive teaching tool with decision support and epinephrine auto-injector (EAI) training to provide education accessible beyond the clinic.
Methods:
This study consisted of two parts: (1) Use of food allergy scenarios to assess the decision support's ability to improve allergic reaction management knowledge. (2) An assessment of our EAI training module on participant's ability to correctly demonstrate the use of an EAI by comparing it to label instructions.
Results:
Twenty-two adolescents were recruited. The median (range) baseline number of correct answers on the scenarios before the intervention was 9 (3–11). All subjects improved with decision support, increasing to 11 (9–12) (p < .001). The median (range) demonstration score was 6 (5–6) for the video training module group and 4.5 (3–6) for the label group (p < 0.001).
Discussion:
Results suggest that the use of this novel m-health application can improve anaphylaxis symptom recognition and increase the likelihood of choosing the appropriate treatment. In addition, performing EAI steps in conjunction with the video training resulted in more accurate medication delivery with fewer missed steps compared to the use of written instructions alone.
Conclusion:
The results suggest that mobile health decision support technology for anaphylaxis emergency preparedness may support traditional methods of training by providing improved access to anaphylaxis training in the community setting.
Introduction
Anaphylaxis is a potentially fatal, severe systemic allergic reaction, which requires immediate treatment with intramuscular epinephrine. 1 Food allergies and stinging insect allergies impact 8–10% of adolescents and are a major public health concern in the United States. 1 Both food and stinging insect allergies are managed predominantly in the community by parents and caregivers. Avoidance of anaphylaxis triggers, in conjunction with epinephrine carriage for emergencies, is the mainstay of allergy management. 2,3 If accidental exposure occurs and anaphylaxis ensues, management is centered on the administration of epinephrine intramuscularly using an epinephrine auto-injector (EAI), which requires patient and caregiver training. 4
Multiple studies have reported that anaphylactic reactions in the community were more likely to be fatal when the individual either did not receive epinephrine at all or its administration was significantly delayed due to perceived lack of symptom severity or uncertain diagnosis. 5 –7 In a community setting, during an anaphylactic emergency, the patient or caregiver must do the following when they have access to an EAI: recognize the symptoms as anaphylaxis, decide to give the EAI, and have the procedural skills to perform the injection correctly. However, print instructions listed on the EAIs may not be sufficient for individuals who lack the confidence, experience, and prior knowledge to use the tool. Multiple studies have shown that despite having access to the instructions listed on the EAIs, individuals commonly fail to use them correctly. 4 –10 Due to fading of user memory and ineffectiveness of the directions listed on EAIs, it is critical that there be alternative forms of teaching EAI administration that are both efficacious and available on demand.
Therefore, we set out to design and test a scalable, accessible, smartphone-based decision support application aimed at educating and training those at risk of anaphylaxis fatalities, as well as those who provide care for the at-risk patients. We hypothesize that this application will improve anaphylaxis symptom recognition and management through the use of patient-centered decision support.
One major benefit of this community-based teaching application is the potential of reaching caregivers and laypeople in both urban and rural settings. In the United States, it is estimated that over 90% of adults and 88% of youth ages 13–17 years own a mobile phone. 8 With the high penetration rate of mobile devices and their widespread acceptability among the U.S. population, 8 interactive training material integrated into a smartphone-based application can be a feasible tool to address gaps in education and research. This community-engaged and patient-centered approach to the management of patients with potentially life-threatening food allergy will be an important change in the current dynamic, which currently relies heavily on paper and didactic education methods.
Methods
Application Description
Our m-health application, Simply Epi, was developed through a collaboration between physicians at the Allergy and Immunology Clinic of Children's Hospital of Wisconsin and the Marquette Ubicomp Computer Science Team. It is compatible with smartphones and tablets utilizing either iOS or Android operating systems. The application (app) contains many functions, including a symptom glossary, decision-support module, EAI video-training modules, and food allergy scenarios. The functions are described below:
Symptom glossary
The symptom glossary contains definitions of medical terms pertaining to allergies, nonmedical synonyms, and pictures and sounds of the symptoms, when applicable.
Decision support module
The decision support module, known as the “Symptom Checker” within the application itself, was designed by clinicians and informaticians to guide users on the appropriate course of action given the symptoms and situational context (e.g., consumption of known food allergen) of a potential allergic reaction (Fig. 1). The decision support algorithm is based on anaphylaxis practice parameters by the American Academy of Asthma, Allergy, and Immunology and the American College of Asthma, Allergy, and Immunology. 9

Screen shot of the decision support function “Symptom Checker.”
EAI training module
The EAI training module within the application utilizes multiple video segments to demonstrate the proper use of EAIs, emphasizing avoidance of the most common errors that individuals encounter when using the devices (Fig. 2). Each video segment demonstrates a single step in the process of using an EAI. The steps were determined using the most recent instructions provided on the EAI manufacturer's Web site.
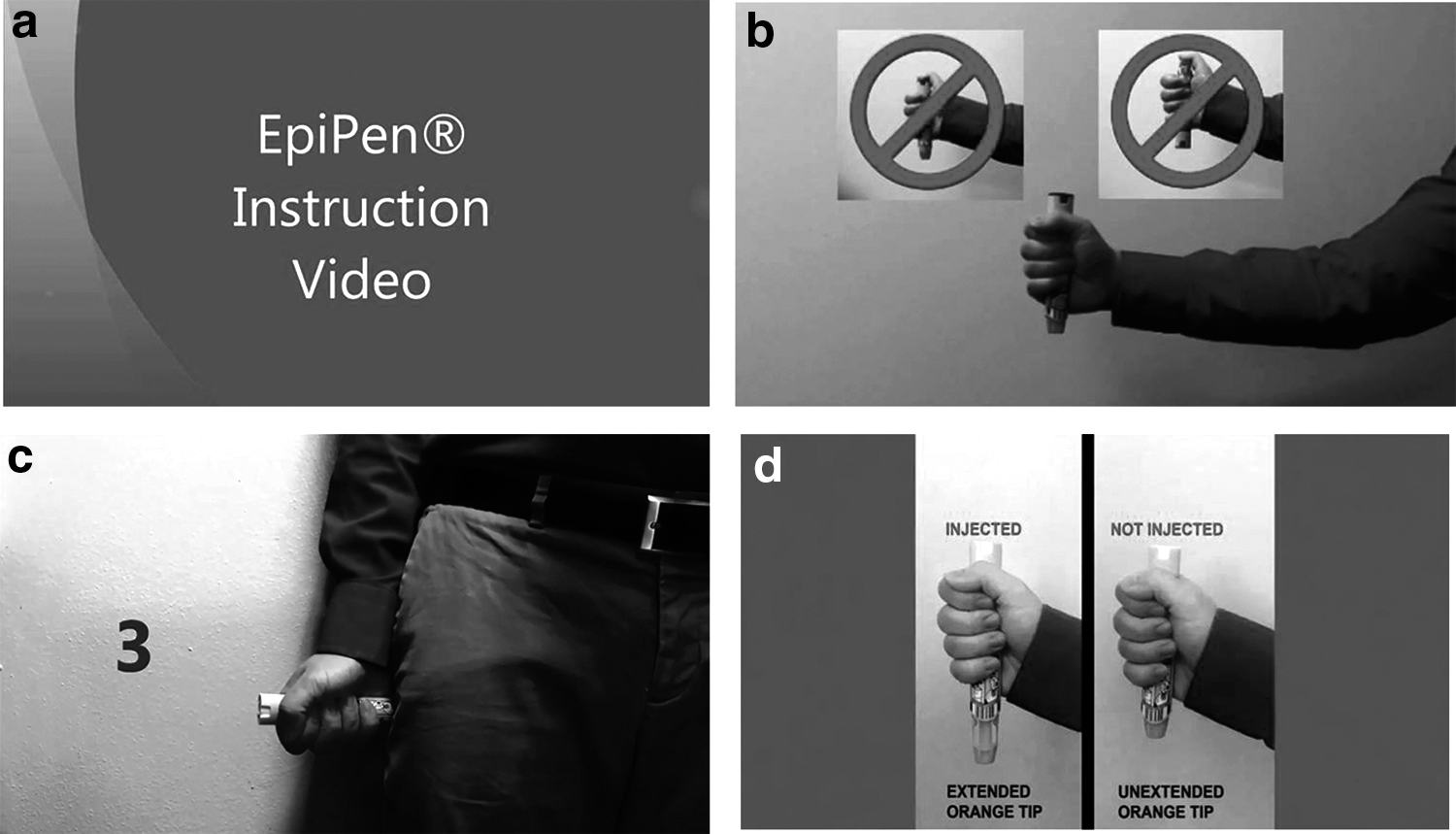
Snapshots of video training modules.
Scenarios
The food allergy practice scenarios are short clinical vignettes describing a minor allergic reaction, anaphylaxis, or no allergic reaction. The decision support function is located below the listed clinical vignette, so that the user may select the symptoms listed in the clinical vignette. After selecting the symptoms, a screen will appear indicating a recommended treatment based on their selections. A summary screen follows, providing feedback on the vignette and the user's selections.
Usability testing was performed with a group of five adolescents to resolve issues involving design, usability, and health literacy to the tool. Feedback was taken back to the design team and used to make significant changes to the application. 10 Adolescents were also engaged to aid in scenario editing to ensure adequate health literacy.
Although our app includes features to improve long-term retention of allergy-related knowledge, it also serves a critical function by providing “just-in-time” instructions (i.e., training that provides knowledge and skill for immediate application to avoid loss of retention due to a time gap). In the event of an emergency situation, the decision support and EAI training module functions can help users identify anaphylaxis and properly administer EAIs. We evaluated the decision support and EAI training modules using a population of 22 adolescents in various scenarios and simulations. Detailed descriptions of the evaluation process of these two functions are provided in the following sections.
Subject Recruitment
The subjects used in this study were recruited from a pool of 204 allergy clinic patients. Inclusion criteria included: (1) having a confirmed diagnosis of either a food or stinging insect allergy and (2) falling within the range of 13–19 years of age. Subjects were excluded from the study if they did not have a handheld device that utilized an Android or iOS operating system (e.g., tablets, smartphones, iPod touch, and so on) or if they had not been prescribed an EpiPen®. We attempted to contact the parent(s) of each patient (or the patients themselves if they were age 18 or older) through telephone. A maximum of three telephone calls with voice mail messages were attempted in trying to recruit each subject. We were only able to recruit 24 subjects from the pool of 204 primarily due to poor response rate (i.e., the telephone calls went unanswered, and the voice mail messages were not returned). Our recruitment rate was also affected by factors such as availability of the subjects for reasons such as after-school activities or moving away for college and lack of ownership of a smart device; however, these were minimal compared to the number of nonresponses. A total of 22 out of the 24 volunteers that consented to participate completed the study. Two subjects did not show up to their scheduled study time. See Supplementary Table S1 for Demographic Data.
Decision Support Evaluation
The decision support function of our app was tested using a self-controlled case series model using all 22 recruited subjects. Testing was performed in a clinical setting. To test their allergy management decision-making at baseline, each subject was asked to choose the most appropriate treatment for the individuals described in 12 clinical vignettes, without the help of any outside resources. The vignettes utilized audio clips and visuals of symptoms to offer a more life-like presentation of potential allergic reactions. For instance, rather than spelling out that the patient had wheals or urticaria, the vignette would show a picture of a rash. After reading the vignettes, the subjects chose one of four options: watch and wait, give epinephrine, have him/her lay down, or give an antihistamine.
After completing the baseline test, the subjects' answer sheets were removed, and the subjects were asked to repeat the same set of vignettes, this time using the decision support modality of the program to help them choose the most appropriate management. Since none of the subjects had access to the decision-support function before the study, each subject was given a brief explanation of how it worked and a 5-min run-in period to practice using it. They were not given the correct answers between each of the two tests. The percentage of correct answers was compared at baseline versus with the use of decision support. During a debriefing, incorrect answers were discussed.
EAI Training Module Evaluation
We tested the efficacy of the EAI training module through a randomized controlled trial in which the subjects demonstrated proper use of an EpiPen with a training device. We chose to test the effect of the training module on EpiPen use rather than other EAIs since it was the most commonly prescribed EAI at our clinic and in the United States. 11 Each of the 24 subjects underwent 1:1 allocation into the following two groups based on age-stratified random sampling: (1) a control group (“Label Group”), in which participants were asked to perform the demonstrations using only their prior knowledge in conjunction with the instructions printed on the label of their EpiPen training device, and (2) an experimental group (“Training Module Group”), in which participants were asked to perform the demonstrations using their prior knowledge in conjunction with the EpiPen video training module.
Each subject in our study was required to make two demonstrations of the use of an EpiPen. The first demonstration served as the baseline testing, where the subjects were instructed to perform a mock injection on themselves using an EpiPen trainer without any instructional resources. Immediately following the blind demonstration, the subjects were required to perform a second demonstration. In the second demonstration, the subjects were allowed to use the instructional resource corresponding to the group to which they were randomly allocated. Each subject could reference their instructional resource while performing the mock EpiPen injection; there was no limit to how often they could refer back to their instructional resource. To avoid influencing their performance in the second demonstration, the subjects were given no feedback regarding their performance in the blind demonstration. The end of each demonstration was determined by one of the following options, whichever came first: (1) the subject stated that they had completed the demonstration, (2) the subject triggered the EpiPen training device, or (3) 7 min expired since the demonstration started.
The scoring was determined using the six-point grading scale shown in Figure 3, which is based on a validated scale described in Sicherer et al. 12 and the EpiPen instructions listed on Mylan's Web site. In addition, the time to completion for each demonstration was recorded to compare how each method of instruction affected the time it takes to properly administer an EpiPen. We also recorded whether each subject's demonstration would have resulted in a successful injection if performed using an actual EpiPen. If a subject performed any of the critical errors listed in Table 1, their demonstration was considered unsuccessful. Note that the subjects did not require a perfect score to perform a successful demonstration.
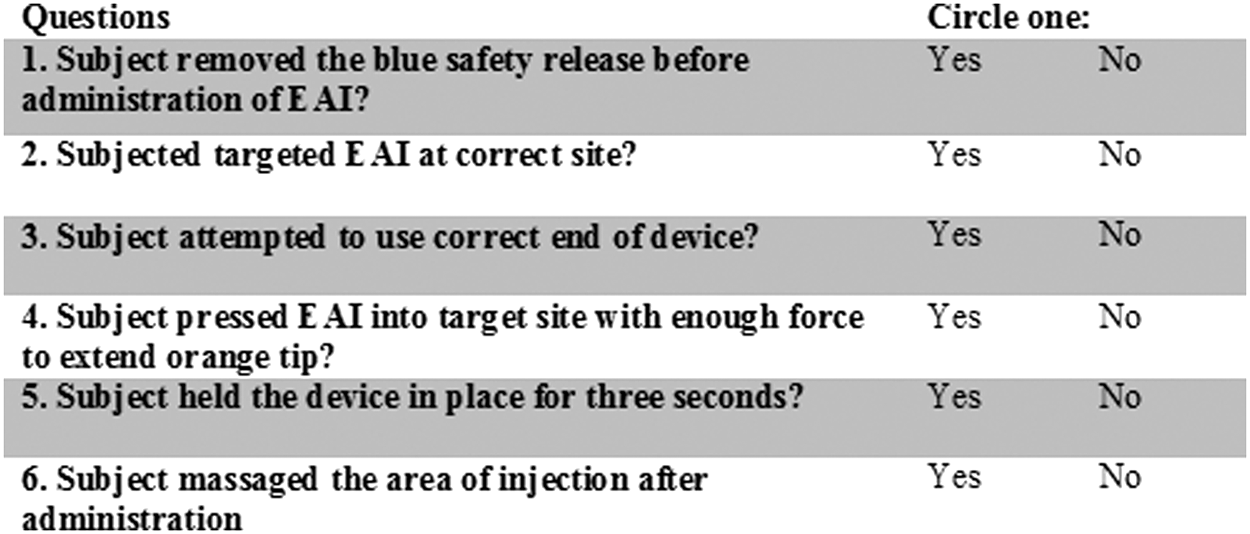
Score card used for grading demonstrations.
Possible Errors During Epinephrine Auto-Injector Demonstration
EAI, epinephrine auto-injector.
Application Usability
One month following the study, the volunteers were asked to answer three survey questions pertaining to the usability and helpfulness of the app. Subject responses were on Likert scale with “1” being Strongly Disagree and “5” being Strongly Agree. Fifteen out of the 22 participants responded to the follow-up survey.
Results
Scenario Evaluation Results
The median (range) correct score out of 12 for the baseline testing was 9 (3–11). After utilization of the application's decision support function (i.e., Symptom Checker), scenario testing increased to 11 (9–12), p ≤ 0.001. There was no statistical difference between those who had previously used epinephrine and those who had not in the baseline testing (p = 0.38) and with the decision support (p = 0.62).
EAI Training Module Evaluation Results
The results for the EAI Training Module Evaluation can be found in Table 2.
Demonstration Results
IQR, interquartile range.
Follow-Up Survey Results
The participants strongly felt the application would help their friends and/or family learn about anaphylaxis with a median (range) of 4.5 (4–5). Responses also suggested that subjects found the application easy to use with a median (range) of 5 (2–5) and that they would download the application if it were freely available with median (range) of 5 (3–5).
Discussion
The results suggest that the use of this novel smartphone-based decision support application can improve anaphylaxis symptom recognition and increase the likelihood of choosing the appropriate treatment. This application could potentially prove to be a useful tool to supplement adolescent education on anaphylaxis emergency preparedness by increasing symptom recognition. In addition, the decision support function could be used in the event of an accidental exposure to an allergen similar to the use of an emergency action plan. In comparison, the use of written action plans in educating adolescents on community-based management of allergic reactions and anaphylaxis has several limitations, including access and teen willingness to carry them. 13 Given that most adolescents have access to a smartphone and the fact that in the postintervention survey, the teens noted a willingness to download the application, this tool can address the gap in much needed access to age appropriate EAI training in this high-risk patient group.
As highlighted in the introduction, correctly treating potentially life-threatening anaphylactic reactions in the community setting requires that the adolescents with access to epinephrine first recognize and second decide to treat their symptoms with an EAI. The results showed that adolescents significantly improved their identification of anaphylaxis with decision support. Despite the fact that half of the subjects had utilized epinephrine on themselves, anaphylaxis management was not significantly different between patients with prior epinephrine use versus no prior epinephrine use. Gaps in knowledge shown in the results demonstrate that adolescents at highest risk of life-threatening anaphylaxis—despite their previous training and experience—could still benefit from guidance and continuous access to education and patient-centered decision support tools.
The results of this study also indicate that our video training module is a more effective means of instructing individuals on proper use of an EpiPen compared to the instructions listed on the EpiPen trainer label. There were similar baseline performances between the Label group and Training Module group, and while both groups showed improvement in their demonstration scoring postintervention, the Training Module Group scored higher than the Label Group. Furthermore, when comparing the postintervention success rates, there again was a statistically significant difference between the two groups, with the Training Module Group achieving a 100% success rate and the Label Group achieving a 60% success rate.
Based on our observations, we believe that the difference in the performance between the Training Module Group and the Label Group can be attributed to the difference in delivery (both audio and visual) and clarity of the two forms of instruction. The short clips in the training module addressed common errors users tend to make, therefore, enabling all participants to have a successful postintervention demonstration in a time efficient manner (in comparison to a long continuous feed video). The simple written instructions on the EpiPen label, which our subjects often misinterpreted, failed to do the same.
Regarding demonstration times, the Training Module Group took more time to perform their demonstrations relative to those in the Label Group, as expected. While the postintervention subjects in the Training Module Group performed over a minute slower than those in the Label Group, we believe that this loss in time is worth the gain in performance. If an individual were to take only 10 s to inject their EpiPen, but failed a critical step (e.g., did not hold it in place long enough or injected the wrong location), then it would be as if they had never used the device at all. Once an EpiPen is triggered, it cannot be used again; they would have to wait for treatment by emergency medical services. In addition, an individual familiar with our app who has used the video training module before could easily skip past the introduction section and move straight to the demonstration steps, saving them time.
Furthermore, this tool could be used in the telemedicine model of care to improve access for patients in rural and difficult to reach settings. Recently, Mount Sinai has launched Rx Universe®, a platform used to prescribe medical applications to patients. Apps in this platform are reviewed by the medical community. This type of platform would be an ideal route from which to distribute this application. 14
Feedback was encouraging, with a large percentage of participants reporting that the application would help their friends and/or family learn about anaphylaxis. This suggests a need to fill this gap in community-based education. The need for community-based education is highlighted in multiple studies that have documented the lack of caregiver and peer understanding of this potentially life-threatening condition. 15 –18
In conclusion, this pilot study of a mobile health decision support application for improving anaphylaxis emergency preparedness shows promising results. This application can be used in conjunction with current clinical training models to improve patient access especially with rural and difficult to reach patients. We anticipate that the decision support feature will empower adolescents to engage in the community-based management of potentially life-threatening allergies. The ultimate goal is to engage adolescents at a deeper thought level and provide better anaphylactic emergency preparedness.
Footnotes
Acknowledgments
The authors thank Mandy Lam, Dr. Eldredge's daughter, for her help in editing the text of the scenarios to make them more readable for the adolescent population. This project was approved by the Institutional Review Board at the Children's Hospital of Wisconsin (project no. 859924).
Funding was provided by the Division of Asthma, Allergy, and Clinical Immunology at the Medical College of Wisconsin. In-kind funding was also provided by the Medical College of Wisconsin, as well as the Ubicomp Computer Laboratory at Marquette University.
Disclosure Statement
CEE served on a Multidisciplinary Anaphylaxis Advisory Board for Mylan Specialties, the maker of EpiPen® April 17–18, 2015 in Canonsburg, PA representing Family Medicine/Public Health. For all other authors, no competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.