
Abstract
Respiratory rehabilitation is a therapeutic path based on performing regular physical exercise. It aims to modify the impact that the respiratory disease has on the patients' quality of life, reducing the severity of the symptoms, and improving their ability to adhere to the activities of daily life. After an initial assessment, they are prescribed (1) different forms and modes of physical exercise and (2) exercise of pulmonary musculature to improve individual performance and the consequences of the symptoms of the emotional sphere related to the pathological condition. At the moment, the devices for pulmonary exercitation/incentivization, even if gamified, give out qualitative information and are not provided with electronics and/or are not connected to the network. The objective of this opinion article is to introduce new models of rehabilitation in this field of Telemedicine and e-Health at a first stage of research. In particular, a new environment for home rehabilitation is proposed, which is based to gamified devices for pulmonary incentivization integrated to the e-Healthcare system integratable also with automatic systems for the 6-min walk tests proposed by the same authors. A first device has been designed and tested. The next steps will be dedicated to the widening of the environment with the design of other devices and to complete the integration with the healthcare system.
The Respiratory Rehabilitation
Respiratory rehabilitation is a multidisciplinary program of treatment for patients with respiratory dysfunctions. This program is calibrated “tailored” for the patient to optimize his or her autonomy and his or her physical and social performance. The reduced tolerance to the effort of the patient with respiratory problems is due to the establishment of a vicious circle for which the patient reduces physical activity due to dyspnea and, therefore, tends to lose trophism and strength of the peripheral muscles. This negative spiral also strengthens itself through the presence of other factors such as anxiety and depression. The patient then develops disability, loss of autonomy, and limitation in daily activities, sometimes dramatically reducing one's quality of life. Currently, retraining is considered the main aspect of a rehabilitation program.
1
Respiratory rehabilitation is a therapeutic path based on performing regular physical exercise. It aims to modify the impact that the respiratory disease has on patients' quality of life, reducing the severity of the symptoms and improving their ability to adhere to the activities of daily life.
1
After an initial assessment, they are prescribed (1) different forms and modes of physical exercise and (2) exercise of pulmonary musculature to improve individual performance and the consequences of the symptoms of the emotional sphere related to the pathological condition. In general, subjects who can benefit from respiratory rehabilitation are subject to: Chronic obstructive pulmonary disease. Cardiac failure. Various diseases of the respiratory system (including neurodegenerative diseases). Trauma of the rib cage.
Devices that can be load-modulated, for example treadmills or exercise bikes, and those that stimulate respiration are particularly useful. 2 –4
Also of particular importance are the walk tests performed without the aid of a treadmill that can be used both for training/rehabilitation and for measuring progress (they allow the estimation of VO2max without a complex direct measure). A widely used test in this area is the 6-min test (a reduced version of the Cooper test). 5
The measurement of oxygen saturation dynamically during exercise is also of particular importance for safety reasons.
Devices for Respiratory Rehabilitation
The action of the domiciliation of the rehabilitation path is important so that the subject can carry it out more effectively and continuously. Currently there are many types of devices such as treadmills and exercise bikes that can be used for exercise and numerous oxygen saturation meters for finger measurement.
There are different types of pulmonary inspiration and expiration exercisers, most of which have the following common characteristics
6
: They do not have a bioengineering measurement chain. Allow a qualitative visualization of respiratory performance. Proposes the exercise in the form of a game (gamification of rehabilitation).
For example, some expiratory exercisers/stimulators have several balls inside the transparent casing that are raised according to intensity of the trial. A raised ball corresponds, for example, to 600 cc/s; two raised balls correspond to 900 cc/s; three raised balls correspond to 1,200 cc/s (Fig. 1).

A pulmonary exerciser/stimulator.
Similar operations present the exercisers/stimulators for inspiration. Surely the main advantage of these devices is the simplicity of operation and the playful attractiveness (gamification). However, these devices do not allow a quantitative registration of the test. It might be useful to record the test to check both the duration and the intensity of the test as a function of time. Naturally, there are exerciser devices, very similar to real medical spirometers that record respiratory parameters and show them graphically on a stand-alone measuring instrument equipped with a viewer such as the Respifit-s device (Eumedics, Germany).
Integration in Telemedicine and e-Health: The Proposal at the Italian National Institute of Health
The integration into the e-Health-based care process can bring benefits in terms of continuity of home care due to the potential of telemedicine in home monitoring.
The idea of ISS is based on two important aspects (Fig. 2).
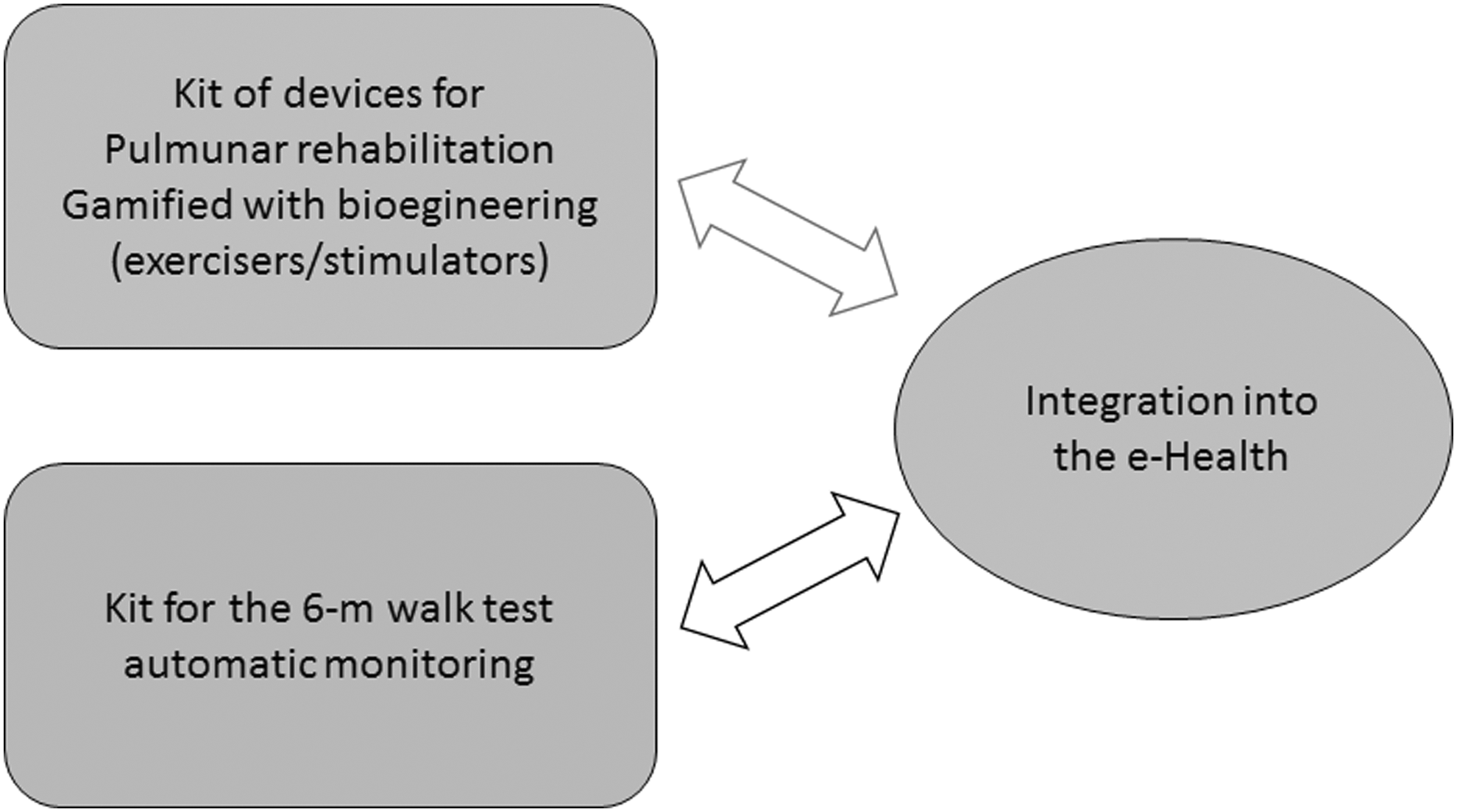
The proposed model.
A first aspect is related to the development and integration in e-Health of respiratory exercisers with the following characteristics/requirements: Connection with a PC, thanks to a bioengineering chain. Real-time PC viewing of the test through a user-friendly and gamified interface. Registration of the trial. Processing of the trial. Sending the trial to the healthcare system.
A second aspect is the integration of automatic systems already developed for the monitoring of walking tests 7,8 with the process of care, which includes the respiratory exerciser/stimulator.
Currently, a first pulmonary rehabilitation device (PURE-D) exerciser has been designed (Fig. 3) for expiration that meets the requirements already described. This exerciser shows in a playful way in the monitor during the test three virtual tanks that are filled according to the intensity of the test. This representation is familiar with traditional ball-based representations. The monitor also reports the flow of air in a Cartesian manner as a function of time and indicators useful during the testing phase. The hardware is based on an appropriately polarized Mini Anemometer series 490 (Kurtz Instruments, Inc.) hot flow measurement sensor and a USB 6008 A/D converter (National Instruments) (Fig. 3A). The software was developed using Labview 2010 (National Instruments) (Fig. 3B). This system has been calibrated and validated. The files related to the trials, once saved, can be sent remotely. Among the elaborations of the trial, we highlight the possibility of obtaining the total area of the recorded trace, an important synthetic index related to the test:

where Vn is the volume/s at the time interval tn .
Work in Progress
The work will continue in two successive phases:
In the first phase, the integration with the healthcare system will be completed with the design of other devices and with the connection 7,8 to the other home device dedicated to the walking test. Subsequently in the second phase, a wide ranging study will be conducted on the categories of subjects already listed, which can benefit from a complete rehabilitation path.
Footnotes
Disclosure Statement
No competing financial interests exist.