
Abstract
Introduction:
Depression is the leading cause of disability in the world. Despite the prevalence of depression, a small proportion of individuals seek mental health services. A cost-effective method for increasing access to mental health services is the implementation of telemental-health programs. This review aims to summarize the state of the field on the efficacy and effectiveness of videoconferencing psychotherapy (VCP) for the treatment of depression.
Materials and Methods:
Systematic literature searches were performed using PsychINFO, PubMed, and EMBASE. Specific inclusion criteria were used to identify controlled and uncontrolled studies evaluating VCP for the treatment of depression. Data extraction included study assessment quality, research design, sample size, intervention details, outcome results, intervention effect size, and statistical differences between VCP and in-person (IP) therapy.
Results:
Of the 1,424 abstracts screened, 92 articles were critically reviewed. Thirty-three articles were included in the review, with 14 randomized controlled studies, 4 controlled nonrandomized studies, and 15 uncontrolled studies. Sample size ranged from 1 to 243 participants. Twenty-one studies reported statistically significant reductions in depressive symptoms following VCP, and the median effect size for studies ranged from medium to the very large range. Most controlled studies reported no statistical differences between VCP and IP groups receiving the same intervention.
Conclusions:
VCP for the treatment of depression is a promising method for delivering mental health services. More rigorous research is needed to evaluate VCP on depression in various contexts and participants.
Introduction
Depression is the leading cause of disability, affecting more than 300 million people worldwide. 1 In the United States, an estimated 16.1 million (6.7%) adults, ages 18 or older, and 3 million (12.5%) adolescents, ages 12 to 17, have experienced at least one major depressive episode in the past year. 2 Despite the ubiquitous nature of depression, only 35% of people in the United States with severe symptoms of depression report having contact with mental health professionals within the past year. 3 One reason for this discrepancy is the lack of available mental health providers and uneven geographic distribution of existing providers. Over the last decade, telemedicine has been a resource utilized to help meet this shortage. Delivery of healthcare via telemedicine offers several advantages over traditional in-person (IP) healthcare delivery. The cost of a telemedicine consult is typically lower for the patient and there is evidence that quality of care via telemedicine is at least on par with IP care in many settings. 4 –9 Furthermore, patient, and often physician, satisfaction is high with telemedicine. 10 –13
Despite these advantages, telemedicine has seen slow implementation in some areas of healthcare due primarily to ongoing payment concerns and policy limitations. 12,14,15 Secondary obstacles to implementation include learning curves associated with the use of new technology along with connectivity and transportation obstacles—particularly in rural areas. 16 –18 Mental health is an area that has been more successful at navigating these challenges than most. The purpose of this systematic review is to examine the research that includes telemedicine and mental health—with an emphasis on depression—to summarize the state of the field and examine opportunities for research and practice moving forward.
Methods
Search Strategy
Research studies were identified through searching the computerized databases of PubMed, PsychINFO, and EMBASE. Results were limited to English-language, empirical peer-reviewed journal articles during the years January 1991–December 2017. Literature reviews and meta-analyses were excluded from the systematic review. See Table 1 for PubMed database search strategy (full search strategy available upon request).
Article Database Search Strategy—PubMed
Inclusion and Exclusion Criteria
We established three inclusion criteria: (1) participants received live, synchronous videoconferencing psychotherapy (VCP) for treatment of depressive symptoms, (2) psychotherapy was conducted one-on-one between therapist and client via videoconferencing technology (i.e., videophone, computer, tablet, etc.), and (3) study utilized established valid and reliable measures of depression as an outcome variable at a minimum of two time points (pre- and postintervention). Studies were included in the systematic review if the primary focus was not depression, but rather included depression as an outcome of treatment. Studies were excluded if they met one of the following criteria: (1) participants received psychotherapy interventions in conjunction with treatment for a medical condition (i.e., chronic pain, irritable bowel syndrome, cancer), (2) participants received psychiatric services other than psychotherapy (i.e., consultation, medication management) in combination with psychotherapy, (3) the intervention involved use of other nonvideoconference mediums (i.e., telephone, e-mail), (4) the intervention involved self-help or module-based online computer psychotherapy programs (e.g., Internet Cognitive Behavioral Therapy), (5) the intervention involved one session or a crisis intervention service.
Data Extraction
Data extracted for the current review included research design, sample size, VCP intervention and control group details, location of online services, intervention statistical significance and/or clinical change on participant depression outcomes, intervention effect size, and statistical differences between VCP and IP therapy. The first author extracted data for the included studies. After the second author and graduate assistants independently extracted data for each study, they met with the first author to discuss areas of disagreement until they reached a consensus.
In addition to data extraction, the quality of study was evaluated using the Effective Public Health Practice Project (EPHPP) Quality Assessment tool. This tool, which contains content and construct validity, possesses the capability to appraise a wide range of research designs. 19,20 The EPHPP assesses six domains of a study: (1) selection bias, (2) study design, (3) confounding variables, (4) blinding, (5) data collection methods, and (6) withdrawals and dropouts. Each domain was rated as “strong,” “moderate,” or “weak,” and an overall rating was assigned for each study.
Results
The electronic database search revealed a total 1,424 articles (see Fig. 1 for flow chart). Following the removal of duplicates, 1,285 articles were initially screened. Of the 92 articles critically assessed for systematic review eligibility, 33 articles met the inclusion criteria. 21 –54 Characteristics of the included studies are outlined in Table 2. Nine studies exclusively evaluated depression as a primary outcome, 6 studies examined a combination of depression and other mental-illness symptomology (i.e., anxiety, post-traumatic stress disorder [PTSD]), and 18 studies measured depression as a secondary outcome.
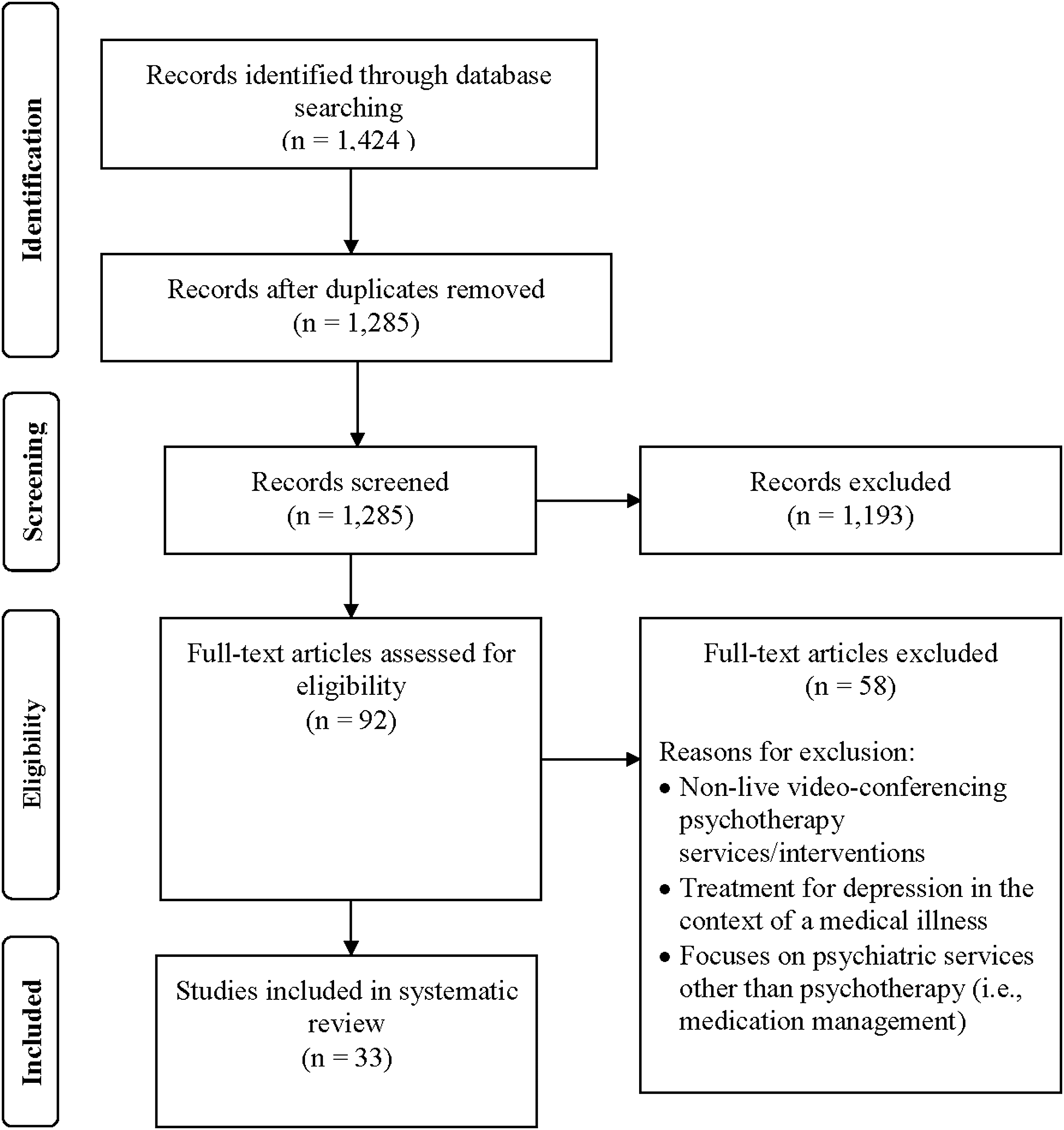
Process for study inclusion in the systematic review.
Details of Included Studies
Participants were active military/veterans.
At least part of the study was conducted in a rural setting.
ABBT, acceptance-based behavioral therapy; BA, behavioral activation; BDI, Beck Depression Inventory; BDI-II, Beck Depression Inventory second edition; CBT, cognitive-behavioral therapy; CDI, Children's Depression Inventory; CES-D, Center for Epidemiologic Studies Depression Scale; CESD-R, Center for Epidemiologic Studies Depression Scale-Revised; DASS-42, Depression Anxiety Stress Scales; ERP, exposure and response prevention therapy; GDS, Geriatric Depression Scale; HAM-D, Hamilton Depression Scale; HRSD, Hamilton Rating Scale for Depression; IP, in-person; MADRS, The Montgomery-Åsberg Depression Rating Scale; MHI, Mental Health Inventory; PE, prolonged exposure therapy; PHQ-9, Patient Health Questionnaire; PST, problem-solving therapy; PTSD, post-traumatic stress disorder; TE, therapeutic exposure therapy; VCP, video-conferencing psychotherapy.
Assessment Quality for Included Studies
The EPHPP quality ratings are shown in Table 3. The majority of studies received a strong or moderate rating on research design. All controlled studies, except 3, examined possible confounders between experimental and control groups. All of the studies utilized valid and reliable measures of depression, and a large number (76%) reported moderate to low attrition rates. Most studies received a moderate rating on selection bias, and a moderate to weak rating on blinding. Blinding ratings were primarily due to the difficulty of blinding participants to a psychotherapy treatment intervention.
Quality Assessment Ratings of Included Studies (Using Effective Public Health Practice Project Quality Assessment Tool) *
Study Design and Sample Characteristics: Overview
Fourteen studies employed a randomized controlled research design and four studies utilized a quasi-experimental design. Of these four, one was a multi-location study that was able to randomize treatment conditions at one site but not at the other site, and one study used a controlled, noncurrent multiple baseline design across participants and settings. 26,29 Fifteen studies applied an uncontrolled research design, with 9 single cohort study (pre- and postdesign), 4 case study A-B designs, 1 multiple baseline design, and 1 single-case interrupted time series.
Sample size ranged from 1 to 243 participants. Randomized studies contained the largest number of participants (range = 13–243), followed by uncontrolled studies (range = 1–82) and quasi-experimental designs (range = 6–48). Females outnumbered male participants in 19/34 studies, and the mean age of participants varied from 10.3 to 80.4 years. One study included participants under the age of 18. 45 Dropout rates fluctuated from 0% to 71% in randomized studies, from 0% to 39% in quasi-experimental studies, and 0% to 30% in uncontrolled studies.
Intervention: Overview
Cognitive behavioral therapy (CBT) was evaluated the most (12/34), followed by behavioral activation (BA; 5/34). Seven studies evaluated a combination of CBT or BA with exposure therapy. Of the 15 studies evaluating depression as a primary outcome, 6 studies evaluated CBT and 4 evaluated BA. VCP protocols were well described in each study, and all articles reported that therapists were trained in the intervention provided. Treatment fidelity was found in 11/14 of randomized studies, 1/4 quasi-experimental studies, and 7/15 uncontrolled studies.
The number of sessions ranged from 5 to 25, lasting 30–90 min each. All studies offered sessions either once or twice a week. Participants in 18 studies received VCP in a clinic setting (i.e., mental health facility; healthcare facility), and participants in 13 studies received VCP in-home. Fifteen studies specifically stated that at least a portion of their study was conducted in a rural area.
Outcomes: Overview
Twenty-two studies reported pre- and poststatistically significant reductions on depressive symptoms from pre- to post-test following VCP intervention, with five of these studies also evaluating clinically significant improvements on depression symptoms. Five studies reported only clinical change results on depression, and six studies included only pre-post mean scores on depression measures. Effect sizes were documented in 16 studies. Five controlled (range = 0.77–1.41; median = 0.87) and five uncontrolled (range = 0.51–1.24; median = 1.02) studies reported Cohen's d effect sizes. Four controlled studies reported eta-squared (η 2) effect sizes (range = 0.22–0.66; median = 0.36). One controlled study (1.00) and one uncontrolled study (0.75) reported Hedges-g (1.00; 0.75). 40,52
Differences Between Vcp and Control Groups
Sixteen controlled studies examined the differences between VCP and control groups. Control groups in 13 studies received the same intervention as the VCP groups in an IP setting. Two studies utilized a three-arm randomized study, with one control group receiving the same intervention as the VCP group via IP, and the other control group receiving telephone support. 24,25 Seven studies found no statistical differences between the online and IP groups. Results were inconclusive in three studies. 41,48,52 However, one of these studies showed that the rate of decline for depressive symptoms was significantly greater for the VCP group. 41 Two additional studies also found that the rate of decline for depressive symptoms was significantly greater for the VCP group, although no significant differences occurred between groups on depression outcomes. 27,45 Another revealed that, while no significant differences occurred between groups at post-test, the VCP group showed greater significant reductions on depressive symptoms at follow-up. 24 One quasi-experimental study reported that IP treatment showed significantly greater reductions in depressive symptoms. 32 One study found that the IP group was significantly better than the online group on the Hamilton Depression Scale (HAM-D) measure, but that no differences existed between groups on the Beck Depression Inventory (BDI) measure. 44 One study found that participants in the IP group were significantly better at post-test than the VCP group, and that no differences between groups existed at follow-up. 22
Study Analyses
Randomized studies
Fourteen randomized studies were included in this review. Control groups received the same intervention as the online group in IP setting for all studies. Two studies utilized a three-arm randomized design (IP and phone-delivered intervention). 24,25 Seven randomized studies focused on depression as the primary outcome and six conducted a part of the study in rural areas. Participants in nine studies accessed VCP in-home, with seven studies consisting of participants who were active military or veterans.
Eight studies documented statistically significant pre- and postreductions in depressive symptoms for both the online and IP groups, with three of these studies also reporting clinically significant change results. Of the participants who received VCP, the range of participants who experienced clinically significant change ranged from 42% to 82% at post-test. Three studies only reported mean scores on depression measures, with two studies finding improvement ranging from moderate depression to mild depression at posttest. 21,44 In the other study, mean scores improved at post-test but still remained in the moderate depression range. 54 Eight of the 14 randomized studies measured depression symptoms at a follow-up period. Four studies indicate post-test improvement maintenance at follow-up. One found that participants significantly worsened at 3-month follow-up and then significantly improved at 12-month follow-up, and one showed that VCP participants maintained at follow-up and IP participants significantly worsened at follow-up. 27,41 Mean scores in one study worsened from mild to moderate depression for both groups, and one showed that IP participants' worsened from normal range to mild depression range. 21,44 Cohen's d effect size was reported in six studies (range = 0.51–1.41; median = 0.79). Two studies reported eta-square (η 2 = 0.22; η 2 = 0.37) and one reported Hedges g (1.00). 43,45,51
Quasi-experimental studies
Three studies were two-cohort analytic comparison designs and one study a controlled noncurrent, multiple baseline across subjects and settings design. 26 One study used depression as the primary outcome. 26 Three studies reported statistically significant reductions in depressive symptoms for both the online and IP control groups and one study reported clinically significant change results. 26 No participants in the VCP group experienced clinically significant change from pre- to postintervention; however, one participant reported clinically significant change at follow-up. 26 One study reported an effect size of Cohen's d = 1.13 and two studies reported eta squared of η 2 = 0.66 and 0.35. 23,29,32
Uncontrolled studies
Nine single cohort studies, four A-B case-study designs, one multiple baseline design, and one single case interrupted time series design were included in this review. Seven studies used depression as the primary outcome variable. Of the 15 studies, 8 found significant statistical reduction in depression symptoms from pre- and post-test, with 2 of these studies also reporting clinical change results. 30,40 Four studies reported only clinical improvement results and three studies pre- and postmean improvement scores. At follow-up, one study found statistically significant reductions in depressive symptoms. 36 Four studies indicated clinical improvement maintenance at follow-up. Four studies report Cohen's d effect sizes (range 0.86–1.24; median = 1.05), and one study reported a Hedges g effect size (0.75). 40 Six studies reported evaluating the intervention in a rural setting, and seven studies used very small sample sizes.
Discussion
The aim of this systematic review was to synthesize the literature on the efficacy and effectiveness of VCP on depressive symptomology. Of the 33 studies included for this systematic review, 22 reported statistically significant reductions in depressive symptoms following evidence-based treatment delivered via VCP. Fifteen studies measured depression as the primary outcome variable, and CBT and BA were the most evaluated interventions. The median effect size for studies ranged from medium to the very large range, with uncontrolled studies containing larger effect sizes. This is expected, as uncontrolled studies use a pre-post comparison. Clinical improvement was only reported by authors in four controlled studies. Because clinical significance was rarely addressed, it was not possible to establish whether symptom reductions were clinically meaningful. However, this comprehensive examination of the literature provides preliminary evidence that evidence-based treatments delivered via VCP can improve depressive symptomology.
Overall, the randomized studies were well designed, considered the potential confounding variables in the research design or analysis, and utilized valid and reliable measures of depression. The control group in all the randomized studies received the same intervention IP. However, there was more inconsistency in the manner by which studies reported dropout rates and follow-up measurement periods. Regarding the latter, a number of studies did not follow-up with participants postintervention. Follow-up procedures should be incorporated into future research designs.
Variability existed on whether VCP was either on-par or more effective than IP psychotherapy for the treatment of depression. Most controlled studies reported inconclusive results or no statistical differences between VCP and IP groups receiving the same intervention. One study found that the VCP group showed greater significant reductions on depressive symptoms only at follow-up. 24 Participants of this study were older adults (mean age = 64.80 years old). Only one randomized study revealed that the IP group showed greater reductions at post-test; however, no differences existed at follow-up; this rural study focused on veteran participants. 22 Research should continue to test the noninferiority between VCP and IP interventions for the treatment of depression in different populations and contexts.
When analyzing the participants and intervention location of the included studies, we discovered some noteworthy findings. First, only one study focused on participants under the age of 18, and the majority of studies contained more female than male participants. 45 Second, more than half of the randomized studies used active military and/or veterans. Third, of the six randomized studies that conducted at least part of the study in rural areas, four focused on military and/or veteran participants, respectively. Two of these four studies examined depression as a primary outcome. The two other rural studies focused on bulimia nervosa and PTSD as the primary outcome variable, and contained mostly female participants. 43,44 In review, of the limited randomized studies conducted in rural areas, not one examines VCP with civilian populations and measures depression as a primary outcome variable. To better generalize the effectiveness of VCP for depression in rural areas, future research should conduct VCP evaluations using a more balanced and diverse sample. Future research may also focus on testing the effectiveness of VCP with children and adolescents. Furthermore, future studies should attempt to enroll a more gender-balanced sample. Military studies were comprised mostly of male participants, and only one nonmilitary controlled study had more male than female participants. 45
Limitations Of The Review
One limitation of the current review is that some studies, especially those published in another language, were not included. Moreover, generalizability is limited based on the broad inclusion criteria for this review. While this review aimed to include as many relevant studies pertaining to VCP interventions for depression as possible, many studies did not include depression as a primary outcome variable. Second, this review did not include studies with participants with health conditions. Third, it was not possible to establish baseline severity of symptoms due to variability in outcome measures used in the included studies. Finally, this review also examined a limited range of telemental health interventions. Recently, there has been technological developments for the treatment of depression using online module self-help programs and smartphone applications. Research evaluating these interventions were not considered for this review.
Future Research
In addition to the recommendations above, this review sheds light on directions for future research. First, more randomized studies should examine both statistical and clinical change of VCP. Second, research needs to continue comparing the effectiveness of VCP interventions with other forms of telemental health treatments (i.e., online module-based interventions; smartphone applications). Third, future research should persist in examining the effectiveness of VCP on depression across diverse populations and settings (i.e., rural; urban; suburban). Because the cost of telemedicine is typically lower than IP settings, more controlled studies should focus on the cost-effectiveness of implementing VCP. Future research also needs to explore newly developed modalities for treating depression, such as Acceptance and Commitment Therapy and Mindfulness-Based Cognitive Therapy.
Conclusions
The findings of this review reveal promising outcomes for VCP in the reduction of depressive symptoms. More specifically, evidence-based interventions (i.e., CBT; BA) show promise for reducing symptoms of depression. However, it is important to note that these are preliminary findings and further work is needed before the effectiveness and efficacy of VCP interventions are fully established. In particular, it will be important to identify the types of therapeutic interventions that are best suited to online delivery and the populations and settings for which they are most effective.
Footnotes
Disclosure Statement
No competing financial interests exist.