
Abstract
Background:
Failure to rescue (FTR) is a benchmark of quality care. Limited evidence exists examining the influence of telemedicine intensive care units (tele-ICU) nursing interventions in preventing FTR. The purpose of this study was to characterize tele-ICU nursing interventions and to determine which combination of documented tele-ICU nursing interventions (DTNI) best predicts prevention of FTR in ICU patients with hospital-acquired conditions (HACs).
Materials and Methods:
We used convergent parallel mixed methods design to conduct qualitative interviews with a purposive sample of tele-ICU nurses (n = 19) from 11 US tele-ICU centers. Quantitative data, including demographics, DTNIs, severity of illness scores, and video assessment times from January 2016 to December 2016 were retrieved for ICU patients discharged from a multihospital health system with a tele-ICU center (n = 861). Findings from both qualitative and quantitative analyses were merged, compared, and contrasted.
Results:
FTR patients had higher severity of illness, longer video assessment by tele-ICU nurses, and were more likely to have DTNIs related to hemodynamic instability. Four themes emerged from qualitative analysis: fundamental tele-ICU nurse attributes, proactive clinical practice, effective collaborative relationships, and strategic use of advanced technology. Mixed methods analysis revealed convergence between DTNIs and tele-ICU nurses' characterizations of their practice.
Conclusions:
Tele-ICU nurses' characterizations of their practice closely align with DTNIs. Tele-ICU nursing practice to prevent FTR involves systems thinking and integration of many complex factors. Tele-ICU nurses can reduce the odds of FTR with focus on support and clinical coordination interventions that avoid hemodynamic instability in ICU patients with a diagnosed HAC.
Introduction
A benchmark of quality for hospital and nursing care, failure to rescue (FTR) is the cause of death in ∼19% of hospitalized patients. 1 FTR, a preventable complication, is defined as a death due to failure to identify and respond appropriately to early indications of patient clinical deterioration associated with a hospital-acquired condition (HAC). 2 –5 Examples of HACs include, but are not limited to, venothromboembolism (VTE), catheter-associated urinary tract infections, and acute kidney injury. 4 HACs are preventable and treatable if recognized early. 4,6
The telemedicine intensive care units (tele-ICU) is a remote surveillance center staffed by experienced critical care nurses and physicians who facilitate proactive clinical interventions in ICUs and other high acuity care areas such as progressive care units. Patients in ICUs with tele-ICU surveillance technology are 26% more likely to survive the ICU, have 12.6% shorter lengths of stay, and have lower overall rates of hospital-acquired complications that result in FTR. 6 –9 Features associated with successful prevention of FTR include early identification of physiological compromise, positive staff perception of work environment, appropriate team dynamics, adequate staffing, and increased nursing surveillance. 10 –14
Although several studies indicate that optimized technology, along with enhanced nursing surveillance are imperative to decreasing the risk for FTR, 10,15 –18 the influence of tele-ICU nurse activities and interventions that prevent FTR is not well established in the literature. Recent studies of acceptance of the tele-ICU model of care suggest that variations in practice, lack of knowledge and understanding of the tele-ICU nurse role, and the perception that tele-ICU intrude or interfere with patient care limit ICU collaboration and engagement in clinical interventions initiated by the tele-ICU. 19 –22
The tele-ICU nursing specialization is an expansion of traditional critical care nursing practice and is estimated that in the United States 800–1,000 critical care nurses practice in the tele-ICU setting. 23,24 High-resolution cameras, computer software applications with clinical decision support algorithms, early warning alerts, and best practices protocols help to facilitate tele-ICU nursing surveillance and interventions. 24 –30 The tele-ICU nurse practice generally includes camera rounding, clinical surveillance, responding to physiological trending alerts, facilitating and expediting patient treatments and therapies, being a resource of expert knowledge for ICU nurses, and ensuring best practice compliance. 28,31 Table 1 presents similarities and differences between the tele-ICU and ICU practice setting.
Key Similarities and Differences Between Tele-ICU and ICU Nursing Practice
Tele-ICU, telemedicine intensive care units.
The purpose of this mixed methods study was to investigate the relationship between tele-ICU nurses' documented interventions and characterizations of their practice related to prevention of FTR. Both the qualitative and quantitative phases of this mixed-methods study were given equal priority and analyzed independently. The methods and results for the quantitative and mixed analyses are presented. Medical University of South Carolina and Baptist Health South Florida Institutional Review Boards approved this study.
Methods
A convergent-parallel mixed methods design was used in this study (see Fig. 1), which involved simultaneous but independent collection and analysis of qualitative and quantitative data. 32 The American Association of Critical Care Nurses (AACN) tele-ICU Model of Success (MOS) 33 provided the deductive framework for this study. Qualitative data were collected from interviews of nurses working in 11 tele-ICU centers across the United States. Details of the qualitative study are reported elsewhere. 34
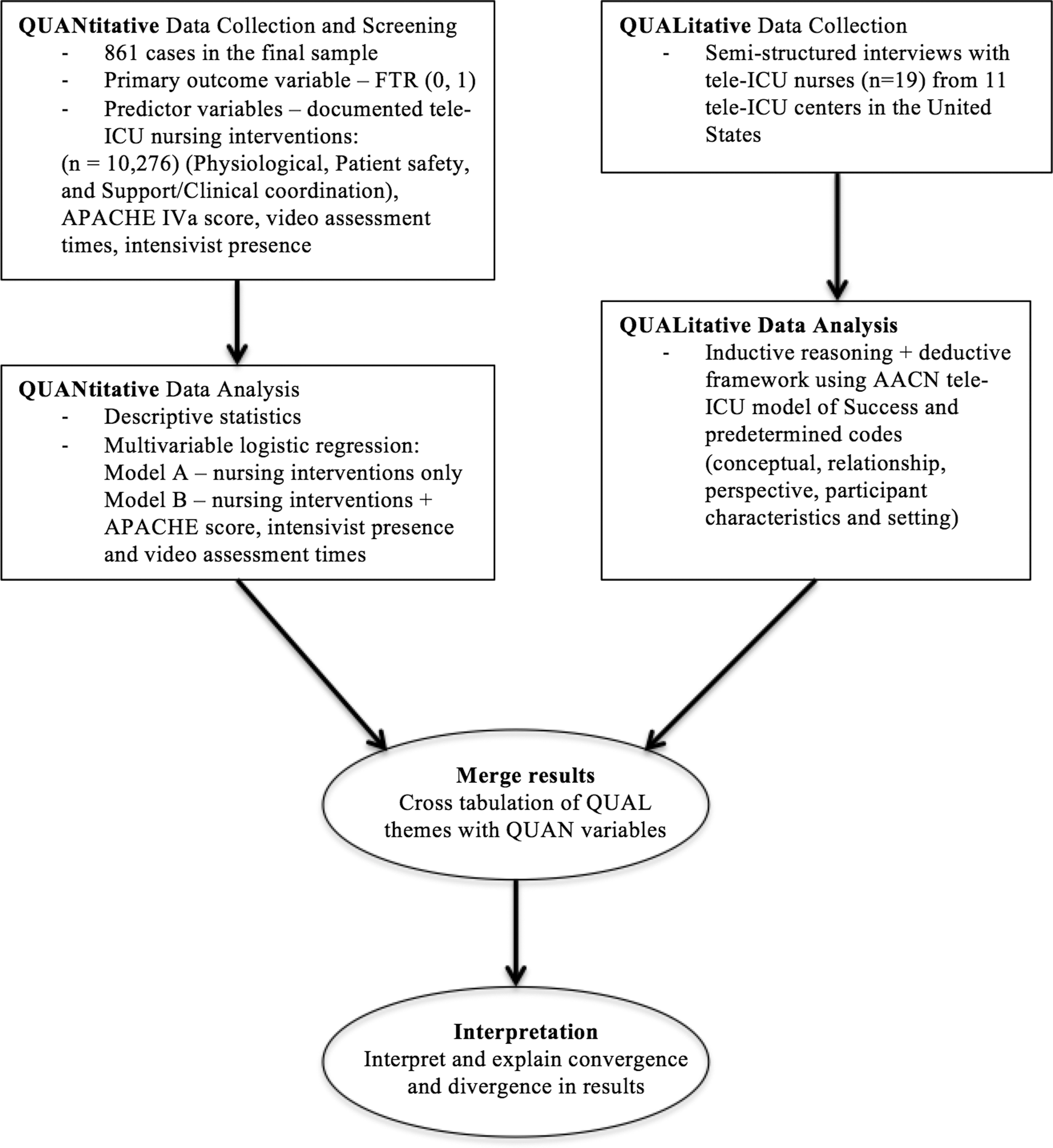
Data analysis plan: triangulation using convergent parallel mixed methods design. AACN, American Association of Critical Care Nurses; APACHE, Acute Physiology and Chronic Health Evaluation; FTR, failure to rescue; tele-ICU, telemedicine intensive care unit.
Clinical and administrative data were retrieved from the electronic health records (EHR) of a multihospital telehealth center. The telehealth center monitors six hospitals with only half having ICU intensivists on site 24/7. The quantitative study site was selected due to the principal investigator's access to the data and the tele-ICU nurses' ubiquitous use of the tele-ICU nursing electronic documentation. After independent analyses of both qualitative and quantitative data, the results were merged, compared, and contrasted. This study aimed to answer the following questions: (1) which combination of tele-ICU nursing interventions best predicts prevention of FTR among patients with HACs? and (2) Are tele-ICU nurses' characterizations of prevention of FTR consistent with documented tele-ICU nursing interventions (DTNIs)?
DTNIs were categorized into three types: physiological, patient safety, and support/clinical coordination. HAC ICD-10 codes were retrieved for all cases that met the inclusion criteria. Centers for Medicare and Medicaid Services (CMS) coding indicator for diagnoses that were present on admission were used to differentiate between diagnoses that were chronic health conditions and those that were acquired during the hospitalization. Figure 2 presents the data selection flow diagram.
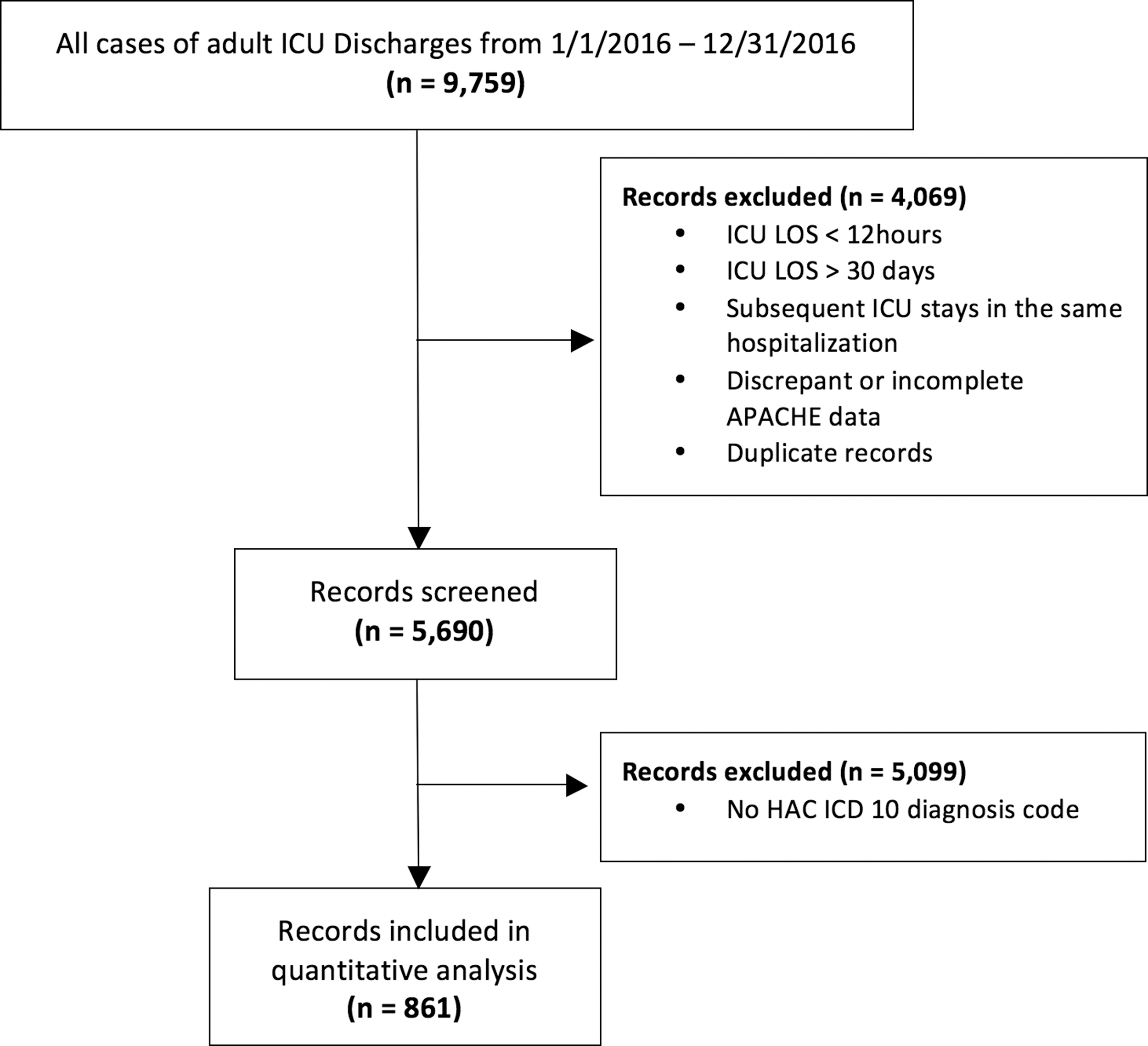
Flow diagram of records selected for quantitative analysis. HAC, hospital-acquired condition.
Measures
The outcome variable of interest, FTR, was constructed as a “yes/no” dichotomous indicator based on patients who died who were diagnosed with a HAC. The independent variables that were examined, included DTNIs, Acute Physiology and Chronic Health Evaluation (APACHE) score, video assessment time (total time tele-ICU nurses used camera to assess each patient the duration of their ICU stay), and presence of ICU intensivist. Intervention subgroups with counts less than 100 were transformed into categorical variables. Patient safety intervention category was treated as a dichotomous independent variable (yes = 1, no = 0) due to the small number of DTNIs in the category (n = 75).
Statistical Analyses
The Statistical Package for Social Science (SPSS®, version 24) was used to conduct the quantitative analyses of records retrieved from the EHR. Descriptive statistics (including median and interquartile range) and frequency distributions were used to summarize both continuous and categorical variables. The variables were screened for missing data, outliers, and multicollinearity. Data transformations were applied as needed. For categorical and continuous variables, 95% confidence intervals (CIs) were used to determine significance in proportions. Contingency tables were used to determine the need to collapse tele-ICU nursing interventions and covariates into larger categories. 35
Bivariate associations were calculated for each of the independent variables in relationship to FTR. A relaxed p-value, p < 0.25 was used to identify candidate variables for the multivariable analysis. 36 Forward stepwise logistic regression was applied to develop the final model. 37 Subsequent variables were entered into the analysis from highest correlation to lowest after adjusting for covariate previously entered into the model. Nagelkerke R Square was used to determine the amount of variance in the primary outcome (FTR) accounted for by the predictor variables. Hosmer-Lemeshow chi-square statistics at level of significance α = 0.05 was computed for each step in the model development. A 95% CI was used to estimate proportions of patients with FTR using maximum likelihood estimation. −2 Log- Likelihood assessed model fit by determining the odds that FTR will occur. A model was considered a good-fit if the −2 Log-Likelihood was low and chi-square significant. Results of the multivariable analysis were reported as odds ratios with 95% CIs.
Results
Table 2 presents tele-ICU patient characteristics for the 861 cases included in the final sample. The population was primarily Hispanic (59.9%, n = 515) with a median age of 70 years (interquartile range 53.5–81.0) and evenly distributed by gender. The overall FTR rate was 12.3% (n = 106). Although, black non-Hispanic race accounted for 8% (n = 69) of the sample, the FTR rate was more than twice the Hispanic group (23.2% vs.10.3%, p = 0.004). More than a third of FTR cases (33.0%, n = 35) had an APACHE diagnosis of infection or sepsis. There were 10,276 DTNIs for the 861 cases in the sample (see Appendix Table A1). Documented physiological and support/clinical coordination DTNIs were significantly associated with FTR (p < 0.001). The most frequent combination of DTNIs were physiological and support/clinical coordination (PC), which was also significantly associated with FTR (p < 0.001). Most DTNIs were triggered by rounding or surveillance (96.4%) and were primarily classified as preventative (68%) or communication (32%). Table 3 displays additional details on the types of documented interventions captured by the tele-ICU nurses.
Characteristics of Adult Critically Ill Patients with Failure to Rescue
The Chi-square statistic is significant at the 0.05 level (two-tailed).
Summarized as median and interquartile ranges due to skewed data.
Outcome variable—FTR, Failure to Rescue, which is the actual hospital mortality rate of patients in the sample; APACHE, Acute Physiology and Chronic Health Evaluation; IQR, interquartile range.
Characteristics of Documented Tele-ICU Nursing Interventions
The Chi-square statistic is significant at the .05 level (2-tailed).
Outcome variable—FTR, Failure to Rescue, which is the actual hospital mortality rate of patients in the sample; P, at least one Physiological Intervention documented; S, at least one Safety Intervention documented; C, at least one Support/Clinical Coordination Intervention documented; All three intervention types documented, PSC.
Tele-ICU, telemedicine intensive care unit.
Multivariable Analyses
Odds ratio estimates from exploratory multivariable analyses of predictive factors are presented in Table 4. Data screening led to the elimination of four outliers. The final variables in the analyses were selected to reduce multicollinearity. With respect to the DTNI only model (model A), documented interventions categorized as hypoxia were predictive of increased odds of FTR by 54% (p < 0.001), whereas interventions categorized as consult/education/mentor predict reduced the odds of FTR by ∼15% (p < 0.038). Importantly, abnormal blood pressure increased the odds of FTR more than twofold (odds ratio [OR] = 2.52; 95% CI, 1.65–3.85, p < 0.001).
Multivariable logistic regression (LR) for the odds of Failure to Rescue
p Values < 0.05 were considered statistically significant.
Forward stepwise LR with documented interventions that were included in the bivariate analysis for relaxed p < .25.
Forward stepwise LR with documented interventions from Model A, video assessment time, and APACHE score.
Video assessment increment of 20 points represents mean to the nearest multiple of 10.
APACHE score increment of 25 points represents approximately one standard deviation.
APACHE, Acute Physiology and Chronic Health Evaluation; BP, blood pressure; CI, confidence interval; OR, odds ratio, adjusted for all covariates shown; PC, physiological and support/clinical coordination interventions (at least one of each type).
Model B included three additional variables to the analysis (APACHE score, video assessment times, and 24/7 ICU intensivist presence). Model B explained 34% of the variance in the dependent variable versus 12% in model A and correctly classified 89.5% of the FTR cases. The final model (model B) indicates that cases with a DTNI for abnormal blood pressure (BP) (a physiological intervention) were 2.26 times more likely to have FTR (p < 0.001). Cases with a combination of documented physiological and support/clinical coordination interventions were retained in the final model but was not a significant predictor of FTR (p = 0.149). The odds of FTR increased by 16% for every 20-min increase in video assessment time (OR = 1.16; 95% CI, 1.03–1.31, p = 0.014). Cases with a DTNI related to an abnormal laboratory value or diagnostic test had a 7.5% (1/.93) lower odds of FTR but was not statistically significant (p = 0.125). DTNIs related to consultation, education, and mentorship were predictive of a 14.9% reduced odds of FTR (OR = 0.87; 95% CI, 0.76–0.99, p = 0.038).
For every 25-point increase in the APACHE score, the odds for FTR was estimated to increase more than threefold (OR = 3.25; 95%CI, 2.48–4.02, p < 0.001). When accounting for video assessment times, severity of illness score (APACHE), and presence of 24/7 ICU intensivist DTNIs in the hypoxia and consult/education/mentor categories were not retained. FTR patients were more likely to be sicker with higher severity of illness scores (APACHE), have longer video assessment times by the tele-ICU nurses, and were more likely to have DTNIs related to physiological instability (abnormal BP, hypoxia, laboratory values, and diagnostic tests). DTNIs related to abnormal BP were retained in both models.
Mixed Analyses
The four interrelated themes derived from qualitative analysis were used to assess the findings from both arms of the study for confirmation, expansion, and discordance. 38 Qualitative interviews confirm that implemented tele-ICU nursing interventions to prevent FTR involved systems thinking and integration of complex clinical, technological, and interpersonal factors. For example, unlike the AACN MOS, tele-ICU nurses in this study characterized their use of technology as a strategic adjunct to proactive clinical interventions rather than the primary driver of their interventions. In addition, skilled communication, a key domain of the AACN tele-ICU MOS, was characterized as one of several tele-ICU nurse attributes that influence prevention of FTR. Other fundamental tele-ICU nursing attributes included empathy, autonomy, and emotional intelligence. DTNIs related to education, consultation, and mentoring captured the influence of these tele-ICU nursing attributes on prevention of FTR. Interviews revealed that collaborative relationships (a domain of the AACN tele-ICU MOS) were as effective as the tele-ICU nurses' ability to navigate seamlessly between the tele-ICU and ICU environments. Convergence between the qualitative and quantitative findings was most prevalent in the proactive clinical practice category (Table 5).
Triangulation of Qualitative and Quantitative Factors
Discordant findings most participants described support or clinical coordination interventions as important in preventing FTR. However, most of these variables were not significant in the multivariable regression.
APACHE, Acute Physiology and Chronic Health Evaluation; BP, blood pressure; CI, confidence interval; ICU, intensive care unit; OR, odds ratio; tele-ICU, telemedicine intensive care unit.
According to participants, tele-ICU physician engagement was more likely to affect tele-ICU nurse implementation of interventions to prevent FTR. DTNIs related to escalation in care captured physician involvement in the interventions. Although more than 60% of tele-ICU nurses interviewed described several support and clinical coordination interventions, only one subcategory (consult/education/mentor) was predictive of reducing the odds of FTR. When accounting for severity of illness, ICU intensivist presence, and video assessment times, there was not enough evidence to determine the efficacy of support and clinical coordination interventions by tele-ICU nurses to prevent FTR. Table 5 displays the compared and contrasted qualitative themes and clinically relevant quantitative variables.
Discussion
The agency for Healthcare Research and Quality designated FTR as a patient safety indicator, while the National Quality Forum recognized FTR as a nurse-sensitive indicator for patients with major surgical diagnoses. 39 As a theoretical basis for tele-ICU nursing practice is necessary, this study made important contributions to the literature by quantitative examination and qualitative exploration of the relationship of tele-ICU nursing practice to patient outcomes, specifically FTR. Our study explored tele-ICU nurses' characterizations of their role in preventing FTR and examined DTNIs influence on FTR among patients with a HAC. Four interrelated themes (fundamental tele-ICU nurse attributes, proactive clinical practice, effective collaborative relationships, and strategic use of advanced technology) emerged and those were then used to triangulate findings from the quantitative analyses.
Fundamental Tele-ICU Nurse Attributes
The results of these analyses revealed that tele-ICU nurses' view of themselves and their role determines their efficacy in prevention of FTR. The tele-ICU nurse attributes were characterized through participant interviews and from analysis of DTNIs. Earlier studies have explored tele-ICU nurses' motivation, job satisfaction, and dynamics of ICU staff acceptance of tele-ICU interventions such as communication and trust, but did not describe how these factors influence patient outcomes. 19,40 Our study revealed that the following fundamental attributes of tele-ICU nurses supported and enhanced prevention of FTR: (1) assertive yet empathetic interactions, (2) emotionally intelligent, (3) collaborative—promotes joint accountability with the ICU, (4) knowledgeable mentor, teacher, or consultant, and (5) skilled communicator.
Effective Collaborative Relationships
Although our study did not find enough evidence to explain the relationship between support and clinical coordination of DTNIs and FTR, evidence exists to support effective collaborative relationships between tele-ICU nurses and ICU teams. Previous studies have determined that tele-ICU nurses' collaboration on best practices such as VTE and sepsis protocols have led to improved bundle compliance. 25,26,41 In addition, previous studies indicate that environments that promote effective collaboration through shared knowledge, shared goals, and mutual respect were optimal for improved patient outcomes such as reduction in FTR rates. 42,43
Future research on the relationship of tele-ICU nurses' support and clinical coordination interventions to prevent HAC rather than FTR, might yield interesting results since HAC is a precursor to FTR and is considered avoidable 44 through proactive evidenced-based best practices. In this study, tele-ICU nurses described ICU staff and leadership lack of acceptance of the tele-ICU model of care as a frequent barrier to effective collaboration in prevention of FTR. While limited research is available on this topic, some studies posit that ICU staff acceptance of the tele-ICU was mostly influenced by knowledge about the tele-ICU, perceived need for the tele-ICU, perceived usefulness, and ICU staff expectations. 19,45,46 Furthermore, the success of tele-ICU interventions is closely related to staff acceptance as evidenced by their intention to integrate the tele-ICU model into critical care practice. 47 –49 Interestingly, interviews highlighted the importance of the influence of engaged tele-ICU physicians in the interventions performed by tele-ICU nurses.
Proactive Clinical Practice
Similar to a review conducted by Taenzer et al., 14 DTNIs and information collected in interviews of tele-ICU nurses indicate that characteristics of prevention of FTR include early identification of negative clinical trends through increased nursing surveillance and effective collaborative relationships between ICU and tele-ICU staff. Tele-ICU nurse involvement in best practice compliance and initiatives resulted in improved adherence to VAP bundle, VTE prophylaxis, and sepsis protocol. 25,26 Furthermore, tele-ICU nurses' ability to closely track and trend hemodynamic parameters such as laboratory values and blood pressure, facilitate early recognition and interventions that prevent FTR. 17,50 Although specific tele-ICU nursing surveillance activities that identify and prevent potential FTR require further study, we noted that physiological interventions were associated with more cases with FTR, indicating likely late interventions from either the tele-ICU or the ICU team. Interview participants identified rounding and surveillance as key features of their proactive clinical practice.
Tele-ICU nurses' experience and clinical expertise are often leveraged to support novice nurses or to ensure adherence to evidenced based practice. 26,51 Our findings suggest that support and clinical coordination DTNIs for example, tele-ICU nurse consultation, education, and mentorship were associated with reduced odds of FTR. Thus, tele-ICU nurses' role as a clinical resource and expert is a key factor in preventing FTR.
Multivariable analyses indicate that increased tele-ICU nurse video assessment of a patient was predictive of FTR. This appears contrary to recent evidence to support decreased FTR with increase in nursing surveillance. 18 However, video assessment was regarded as only one element of tele-ICU nursing surveillance, where increased video assessment time was likely during emergency interventions or extended due to ICU nurse request for tele-ICU nurse assistance with patient evaluation or observation. In addition to video assessment, participants included review of EHR for information or discrepancies and strategic use of advanced technology (e.g., monitoring and managing hemodynamic smart alerts) as imperative factors in tele-ICU nursing surveillance that can prevent FTR.
Limitations
This study provided a comprehensive understanding of the phenomenon of prevention of FTR in tele-ICU nursing practice. However, some limitations are noted. First, DTNIs were evaluated from only one study site. The degree to which the tele-ICU nurses use the documentation software likely varies. Analysis of the DTNIs from all study sites might reveal additional important or confirmatory findings. Secondly, the characteristics of the quantitative sample were reflective of the largely Hispanic population served by a single tele-ICU center. Our findings indicated a disproportionately high FTR rate among non-Hispanic blacks. Access to tele-ICU centers that serve a larger population of non-Hispanic blacks may provide further understanding of FTR in this population.
Finally, given the homogeneity of the interview sample (i.e., similar workflows and documentation software across tele-ICU centers), future research should focus on including tele-ICU centers that use alternative surveillance software and workflows. Despite the limitations indicated, findings from our study establish the basis for a larger study of tele-ICU nursing that can be used to develop evidence-based standards of practice.
Conclusions
FTR patients were more likely to have higher severity of illness scores, longer video assessment times and hemodynamic instability. Interview findings contextualized our understanding of DTNIs. Tele-ICU nurses who are assertive and confident in their contributions to the care team are more likely to intervene sooner to prevent FTR. Results from this study suggest the following standards for tele-ICU nursing practice that may positively influence FTR: tele-ICU surveillance focused on avoiding hemodynamic instability, active involvement of tele-ICU nurses in education and mentorship of ICU nurses, emphasis on tele-ICU-ICU nurse consultation, and integration of tele-ICU nurses in multidisciplinary care by providing support and clinical coordination interventions. Nurses play a significant role in the outcomes associated with the tele-ICU implementation and key findings in this study highlight the positive impact of the tele-ICU nurse role on patient-level interventions and outcomes.
Footnotes
Acknowledgments
Thank you to the tele-ICU nurses for sharing their experiences and making invaluable contributions to patient care and outcomes. Special thanks to Mr. Carlos Valle for his contributions to this research. This study was made possible with the support of the Medical University of South Carolina College of Nursing, Stewart Dissertation Award fund.
Disclosure Statement
No competing financial interests exist.
Types and Frequency of Documented Interventions by Categories (n = 10,276)
| PHYSIOLOGICAL | PATIENT SAFETY | SUPPORT OR CLINICAL COORDINATION | |||
|---|---|---|---|---|---|
| Abnormal laboratory or test | 1,345 | Inadequate waveforms | 18 | Patient evaluation/observation | 3,047 |
| Hypoxia | 324 | Risky behavior or suicidal | 12 | Analyze/interpret laboratory or test results | 1,902 |
| Neurological deficit | 204 | Extubation/decannulation | 11 | Facilitate treatment | 1,149 |
| Pain or agitation | 141 | Fall (intercepted or occurred) | 9 | Consult/educate/mentor | 886 |
| Abnormal blood pressure | 114 | Restraints | 9 | Escalate to provider | 737 |
| Arrhythmias | 67 | Documentation issue—missing incomplete or incorrect | 8 | Troubleshoot (equipment or device) | 155 |
| Other | 19 | Other | 8 | Manage treatment or therapy | 91 |
| Hemorrhage | 12 | Other | 8 | ||
| Total (%) | 2,226 (21.7) | Total (%) | 75 (0.7) | Total (%) | 7,975 (77.6) |