
Abstract
Introduction:
Veterans with low vision who live in rural communities have limited access to low-vision rehabilitation services, unless they are able to travel several miles to a specialty low-vision clinic. A low-vision optometry telerehabilitation evaluation is a thorough assessment of patient's functional vision. Following each low-vision optometry telerehabilitation evaluation is a low-vision telerehabilitation initial assessment with a blind rehabilitation therapist. Our objective was to estimate the acceptance and practicality of low-vision telerehabilitation and investigate the travel cost and time savings.
Methods:
Utilizing Google Maps™, round-trip travel mileage and travel time can be estimated between the veteran's home and the Buffalo Veterans Affairs (VA) and compared with the round-trip mileage and travel time between the veteran's home and local community-based outpatient center (CBOC) or local VA for low-vision telerehabilitation services. The difference is the savings in travel miles and time. Cost saving can be calculated by multiplying difference in travel miles by cost per mile.
Results:
Veterans who chose not to schedule face-to-face low-vision rehabilitation at the Buffalo VA due to an average round-trip travel distance of 151 miles scheduled a low-vision telerehabilitation at a local CBOC or local VA with an average round-trip travel distance of 29 miles. Adding low-vision telerehabilitation services from fiscal year (FY) 13 to FY 17 resulted in a 24% increase in low-vision patient care. The median saving of travel miles for rural veterans was 122 miles per veteran, and the median saving of travel time was 2.09 h per veteran. Overall, the median saving of the travel cost was $65.29 per veteran.
Conclusions:
This study shows and supports low-vision telerehabilitation as an accepted, practical, time-saving, and cost-saving alternative option to traditional face-to-face consultations with a low-vision optometrist and blind rehabilitation therapist.
Introduction
Low-vision rehabilitation services provided as early as possible after visual impairment diagnosis are important to prevent potential decline in functional ability over time. 1,2 Basic low-vision services are sufficient for most patients with mild low-vision impairment, but basic low-vision services plus low-vision rehabilitation is more effective than basic low-vision services alone for patients with best corrected distance visual acuity, better eye worse than 20/63 to 20/200. 3
A low-vision optometry telerehabilitation evaluation is a thorough assessment of patient's functional vision. Throughout the low-vision evaluation, a low-vision optometrist asks specific questions, listens to the patient's answers, and responds to the patient's questions appropriately. 4,5 The main goal is to prevent depression by addressing the psychological effects of low vison and provide each patient with the knowledge of his or her clinical information to help him or her during this challenging visual transition. Optical and nonoptical devices are discussed and some are demonstrated during the telehealth session with the assistance of a telehealth clinical technician. 4 Training is recommended in the future with a blind rehabilitation therapist in the patient's home. After each low-vision optometry telerehabilitation evaluation is a low-vision telerehabilitation initial assessment performed by a blind rehabilitation therapist. This initial assessment prepares the patient for adaptive skills to be utilized in the home.
Veterans with low vision who live in rural communities have limited access to low-vision rehabilitation services, unless they are able to travel several miles to a specialty low-vision clinic. When you add the loss of the ability to drive, travel becomes an insurmountable obstacle to receiving low-vision rehabilitation services. Access to a specialty clinic with a low-vision optometrist and blind rehabilitation therapist becomes cumbersome, expensive, and time consuming for many patients and their families.
Visual impairment service team (VIST) coordinators are case managers at Veterans Affairs (VA) facilities to coordinate available resources for visually impaired and legally blind veterans. Their major responsibility is to coordinate services for the visually impaired veterans and their families, thus serving as the entry point into the continuum of care for visually impaired veterans. In western New York, VIST coordinators in rural areas noted that family members and/or friends of the visually impaired are more willing to drive a few miles to a local VA community healthcare facility instead of several miles to a specialty clinic. Those veterans and their families, who chose not to schedule low-vision services at the Buffalo VA, scheduled low-vision clinical video telehealth services at a local community-based outpatient center (CBOC) or local VA that was significantly closer. Ultimately, low-vision telerehabilitation decreases a major barrier to access low-vision rehabilitation services. Low-vision telerehabilitation (also known as low-vision clinical video telehealth) currently allows low-vision rehabilitation with a low-vision optometrist and a blind rehabilitation therapist in a timely manner, without the need for the patient to travel long distances to receive services. 4,5
Veterans with low vision can be scheduled for face-to-face low-vision rehabilitation services at the Buffalo VA. By adding low-vision telerehabilitation services, low-vision veterans who schedule care with their local optometrist and/or ophthalmologist, but cannot travel to the Buffalo VA, have the option to schedule at three rural VAs and 10 CBOCs in western New York. 5 Home low-vision optometry telerehabilitation is an option for veterans who are enrolled in home-based primary care services, provided they have been seen by a local eye care provider. 5 Increasing access to low-vision rehabilitation services by utilizing telehealth 6 –11 enables estimation of travel mileage and thus calculation of time savings.
The aim of this retrospective study was to evaluate patient acceptance and practicality of low-vision telerehabilitation in providing early intervention by a low-vision optometrist and blind rehabilitation therapist. By eliminating the need to travel long distances to a specialty clinic, low-vision telerehabilitation may offer significant travel time and cost savings.
Methods
VIST coordinators are case managers at VA facilities and receive consults from various healthcare providers to coordinate services for visually impaired and legally blind veterans. In fiscal year (FY) 2013, VIST coordinators in rural western New York areas began to offer face-to-face low-vision rehabilitation services at our specialty low-vision rehabilitation clinic at the Buffalo VA or low-vision telerehabilitation at a local CBOC or local VA. Those veterans and their families, who chose not to schedule low-vision services at the Buffalo VA, scheduled low-vision clinical video telehealth services at a local CBOC or local VA that was significantly closer. For our home-based primary care veterans, a home low-vision optometry telerehabilitation appointment was scheduled. This retrospective study investigates the travel cost saving and practicality of low-vision telerehabilitation. VA Western New York Healthcare System facilities and travel distances include several counties that encompass one-third of New York State (Fig. 1). Examples of one-way and round trip distances from the Buffalo VA to the following places are: (1) Batavia, NY, 44 miles and 88 miles; (2) Bath, NY, 110 miles and 220 miles; (3) Canandaigua, NY, 93 miles and 186 miles; and (4) Rochester, NY, 76 miles and 152 miles, respectively.

The Western New York Healthcare System facilities include several western counties that encompass one-third of New York State (gray shaded area).
Initially, only face-to-face low-vision rehabilitation services were offered at the Buffalo VA. Geographically, many of our veterans live in rural areas of western New York and were unable to access our low-vision rehabilitation services at the Buffalo VA (Fig. 1). Adding low-vision telerehabilitation services at three rural VAs and 10 CBOCs increased access by providing other options to those veterans who could not travel to the Buffalo VA, resulting in additional veterans who scheduled low-vision clinical video telehealth services beginning November 2012 (FY 13).
Utilizing Google Maps™, round-trip travel mileage can be estimated between the veteran's home and the Buffalo VA and compared with the round-trip mileage between the veteran's home and local CBOC (or local VA) for low-vision telerehabilitation services. The difference is the saving in travel miles. When veterans are evaluated utilizing clinical video telehealth in their home, their travel is 0 miles. Cost saving can be calculated by multiplying the difference in travel miles by cost per mile. The Internal Revenue Service determines the standard mileage rate used to calculate deductible costs. The rate used for business deductions is based on an annual study of the fixed and variable costs of operating an automobile. Beginning on January 1, 2017, the standard rate of the fixed and variable cost that was determined to operate a vehicle is $0.535 per mile. 12
Round-trip travel time can also be estimated between the veteran's home and the Buffalo VA and compared with the estimated round-trip travel time between the veteran's home and local CBOC (or local VA) for low-vision telerehabilitation services. The difference is the saving in travel time for the veterans and their driver. When veterans are evaluated utilizing clinical video telehealth at their home, their travel time is 0 minutes. The travel time saving of the veteran's presumed driver was not included in our data, but not excluded from acknowledgment of the importance of time saving for the sighted driver.
Immediately after the veteran's completed low-vision optometry telerehabilitation evaluation and initial vision rehabilitation assessment, a low-vision telehealth quickcard survey is completed verbally by most of our veterans in the presence of a blind rehabilitation therapist. Questions asked are: (1) Was service timely? yes/no; (2) Was your privacy respected? yes/no; (3) Were you confident in your provider? yes/no; (4) Was the staff caring? yes/no; (5) Did we help you in your daily life? yes/no; (6) Did you receive information and advice about your eye condition? yes/no; and (7) Overall: How would you rate your overall satisfaction with telehealth low-vision services? excellent/very good/good/fair/poor; What could have been better?
We began offering low-vision clinical video telehealth initially at rural VA hospitals in November 2012 (FY 13) and expanded to rural CBOCs and veteran's homes. The total number of veterans seen from November 2012 (FY 13) to September 30, 2017 (FY 17) was 419 in 5 years and continues in FY 18 (Fig. 2). (FY 18 data are not added to this study.) Of the 419 veterans, 406 are male and 13 are female with the average age of 83 years with a range of 50–101 years. Ocular diagnosis varies with each veteran. Of the 419 veterans, 208 had ocular diagnosis that resulted in noncorrectable or best corrected visual acuity in both eyes up to 20/150 (defined as not legally blind); 149 had noncorrectable or best corrected visual acuity in both eyes of 20/200 or worse (defined as legal blindness); 22 had noncorrectable peripheral visual field loss in one or both eyes >20 degrees (defined as not legally blind); and 40 had noncorrectable peripheral visual field loss in both eyes <20 degrees (defined as legal blindness). Ocular diagnosis within the 419 veterans included exudative and nonexudative macular degeneration, cataracts, retinal detachment, proliferative and nonproliferative diabetic retinopathy, glaucoma, stroke, branch retinal vein occlusion, retinitis pigmentosa, Fuch's corneal dystrophy, epiretinal membrane, anterior ischemic optic neuropathy, ocular histoplasmosis, corneal transplant, Stargardts macular degeneration, birdshot chorioretinopathy, rod/cone dystrophy, pathologic myopia, and acquired monocular vision of various etiologies. Total and median travel cost and time saving was estimated per veteran and graphed per FY.

Veterans accessing low-vision clinical video telehealth at CBOC/home—Total number of veterans seen from November 2012 (FY 13) to September 30, 2017 (FY 17) is 419 in 5 years. CBOC, community-based outpatient center; FY, fiscal year.
Results
Adding a low-vision telerehabilitation clinic to our ongoing face-to-face low-vision rehabilitation clinic at the Buffalo VA, during this time period, noted an increase in overall veterans who were now able to access telehealth low-vision services at three rural VA hospitals, 10 rural CBOCs, and/or in their home (Fig. 3). Low-vision optometry telehealth evaluations increased our workload by 3% (7 telehealth/259 telehealth and face-to face) in FY 13, by 21% (84 telehealth/392 telehealth and face-to-face) in FY 14, by 35% (125 telehealth/361 telehealth and face-to-face) in FY 15, by 32% (124 telehealth/390 telehealth and face-to-face) in FY 16, and by 23% (79 telehealth/342 telehealth and face-to-face) in FY 17. Within this 5-year period, the average workload increase was 24% (419 telehealth/1,744 telehealth and face-to-face). It is important to note that we increased our workload without increasing our staff.
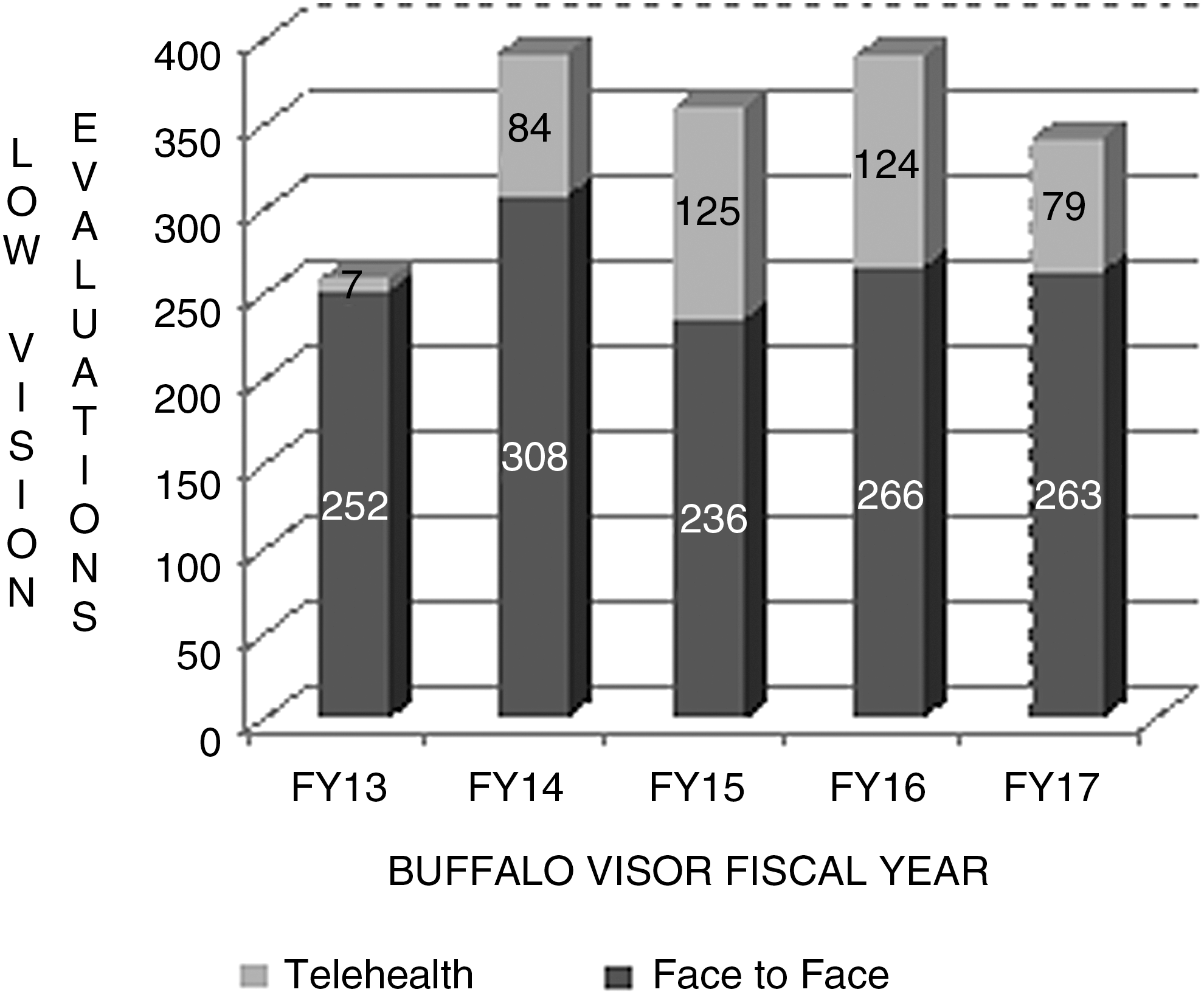
Low-vision evaluations—face-to-face and telehealth per FY.
Round-trip mileage was estimated utilizing Google Maps between each veteran's home and the Buffalo VA and compared with round-trip mileage between the veteran's home and local CBOC or local VA. The estimated round-trip travel that the veteran and his or her family chose not to schedule to receive face-to-face low-vision rehabilitation services was calculated (Table 1). On average, the round-trip travel mileage that they chose not to schedule was 151 miles (63,385/419). The estimated round-trip travel that the veteran and his or her family chose to schedule a low-vision telerehabilitation evaluation at a local VA, CBOC, or in their home was calculated (Table 2). On average, the round-trip travel mileage that they chose to schedule was 29 miles (12,249/419).
Veterans Who Chose Not to Schedule a Face-to-Face Low-Vision Clinic Appointment at the Buffalo VA Due to Estimated Travel Distance from Their Home to Buffalo VA (Miles)
FY, fiscal year; VA, Veterans Affairs.
Veterans Who Chose to Schedule a Low Vision Telehealth Clinic Appointment at the Local Community-Based Outpatient Center or at Home (if Eligible) Due to Estimated Travel Distance from Their Home to the Local Community-Based Outpatient Center (Miles)
The difference between these two estimated round-trip travel distances is the saving in travel miles. As noted earlier, when the veteran is evaluated utilizing clinical video telehealth in his or her home, his or her travel is 0 miles. Total estimated miles saved in 5 years are 51,136 miles for 419 veterans (Fig. 4). Of the 419 veterans seen since November 2012 (FY 13), the median saving of travel miles was 122 miles per rural veteran (51,136 miles/419 veterans). The range of travel miles from the veterans' home to their low-vision telehealth appointment was 0–153 miles. The range of travel miles from the veterans' home to the Buffalo VA was 18–334 miles. Cost saving is calculated as cost per mile ($0.535 per mile). 12 The difference between the round-trip mileage estimated between the veteran's home and Buffalo VA and subtracted from the round-trip mileage between the veteran's home and local CBOC was multiplied by $0.535, making a significant cost saving per veteran. The total saving in 5 years was $27,357.76 for 419 veterans (Fig. 5). The average cost saving per veteran during this 5-year period is $65.29 ($27,357.76/419 veterans) (Fig. 6).
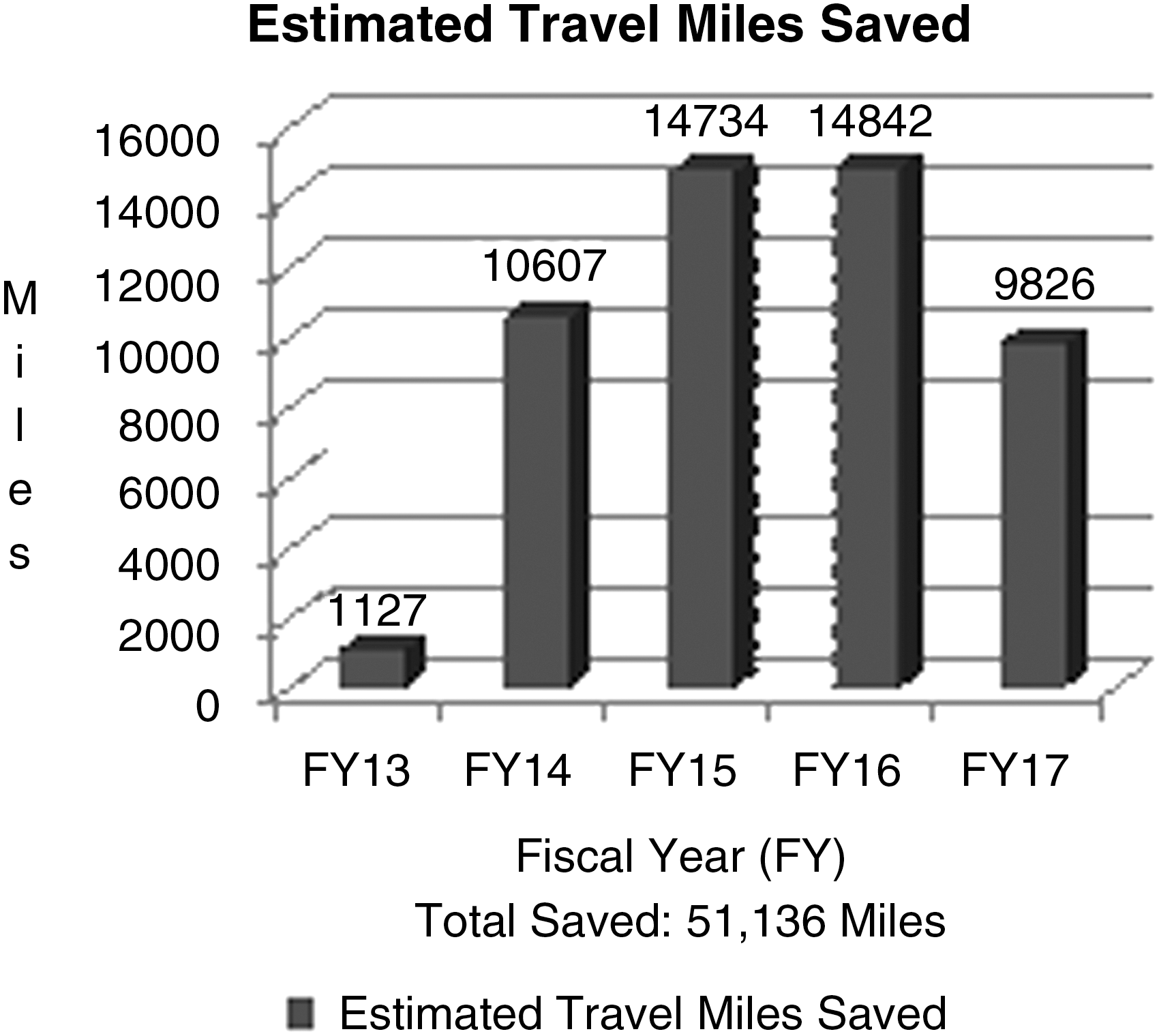
Estimated travel miles saved —shows the significant travel mileage savings each fiscal year. Total estimated miles saved in 5 years is 51,136 miles for 419 veterans.

Estimated total cost saving in 5 years: $27,357.76 for 419 veterans.

Estimated average cost saving per veteran in fiscal year 13 to fiscal year 17, with an overall average saving of $65.29 ($27,357.76/419).
Round-trip travel time saving was calculated between the veteran's home and Buffalo VA and compared with round-trip travel time saving between the veteran's home and local CBOC. The difference is a significant saving in time in minutes and/or hours. As noted earlier, when the veterans are evaluated utilizing clinical video telehealth in their home, their travel time is 0 minutes. The estimated time saving for 419 veterans in 5 years is 878 h (Fig. 7). The average time saving per veteran is 2.09 h (878 h/419 veterans). The range of travel time from veterans' home to their low-vision telehealth appointment was 0–172 min (0–2.87 h). The range of travel time from veterans' home to the Buffalo VA was 34–352 min (0.57–5.87 h). Regarding completion and review of a segment of low-vision telehealth quickcard surveys from February 23, 2017 to March 27, 2018, 100% of the 62 reviewed noted “yes” to questions 1–6 and rated overall satisfaction of low-vision telehealth as “excellent.”
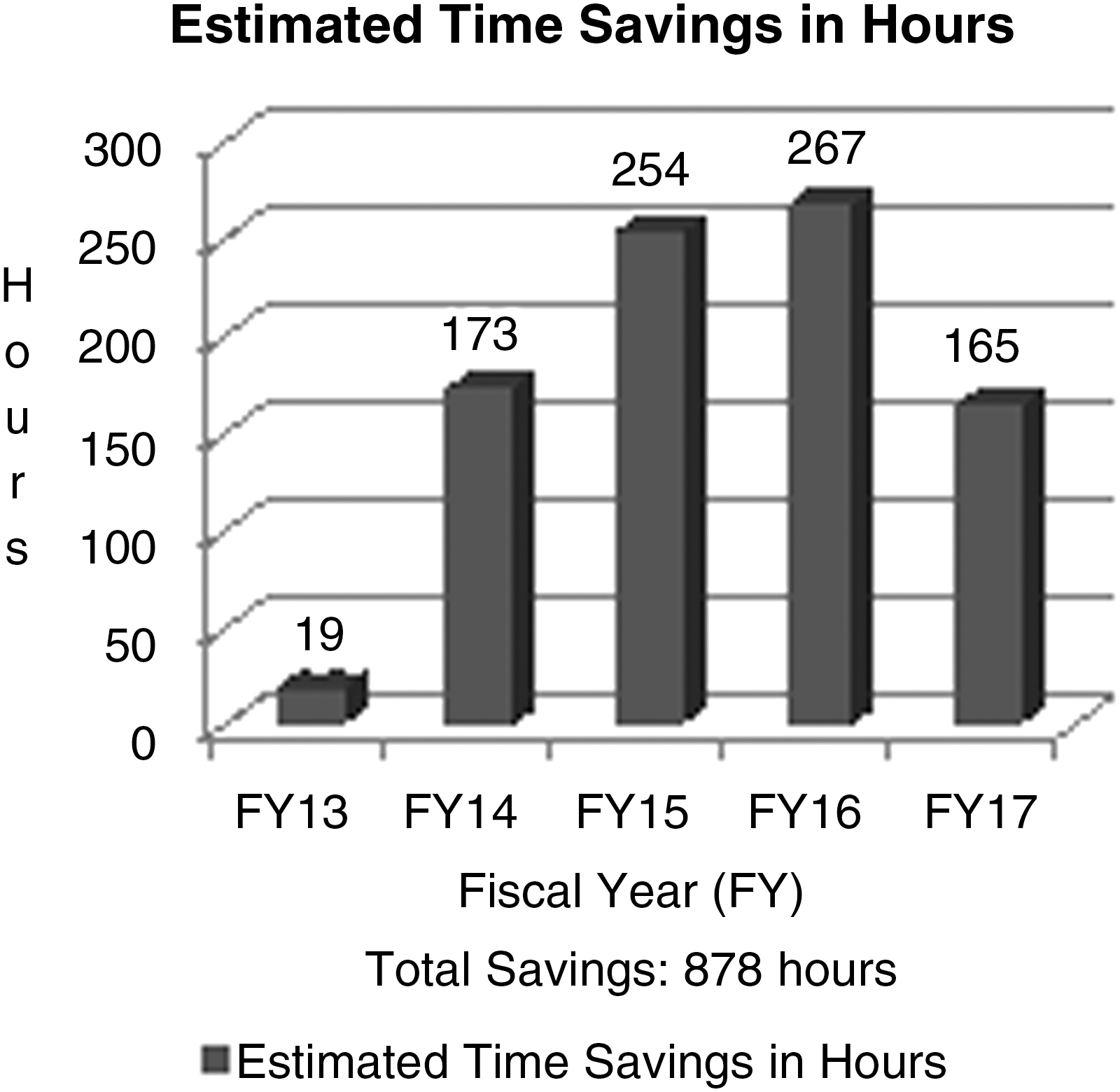
Total estimated travel time saving in 5 years is 878 h.
Discussion
Adding low-vision telerehabilitation services in November 2012 (FY 13) increased access to rural veterans in western New York. For the next 5 years, 419 veterans who were unable to access low-vision rehabilitation due to travel issues were able to access low-vision telerehabilitation services at their local CBOC, local VA, or in their home and increased our overall low-vision rehabilitation workload by 24%. Veterans who chose not to schedule face-to-face low-vision rehabilitation at the Buffalo VA due to an average round-trip travel distance of 151 miles scheduled low-vision telerehabilitation at a local CBOC or local VA with an average round-trip travel distance of 29 miles. Of the 419 veterans seen since November 2012 (FY 13), the median saving of travel miles for rural patients was 122 miles per veteran (51,136 miles/419 veterans) and the median saving of travel time was 2.09 h per veteran (878 h/419 veterans).
Overall, the median saving of the travel cost per rural individual (utilizing $0.535 per mile) was $65.29 per veteran ($27,357.76/419).
The low-vision telerehabilitation clinic at the Buffalo VA increased workload by scheduling veterans who declined face-to-face services in the past and current veterans who were referred but would not or could not travel to the Buffalo VA. Travel mileage and time saving resulted in an increase in access to low-vision rehabilitation (24% increase in partially sighted veterans evaluated in 5 years) by reducing the veteran's travel distance, time, and cost.
Conclusion
This study shows and supports low-vision telerehabilitation as an accepted, practical, time-saving, and cost-saving alternative option to traditional face-to-face consultations with a low-vision optometrist and a blind rehabilitation therapist. Utilizing low-vision telerehabilitation increases early access and enables veterans who cannot travel to a specialty clinic the opportunity to prevent potential decline in functional ability over time. 1,2
As technology advances, future cost-saving technology can be utilized for consultations with a low-vision optometrist and blind rehabilitation therapist. Ultimately, a modern interdependent low-vision telerehabilitation service system providing simpler, faster, and cheaper services to veterans who are partially sighted or legally blind could be implemented.
Footnotes
Disclosure Statement
No competing financial interests exist.