
Abstract
Purpose:
This article describes the design and implementation of a web-based portal developed to provide supported home practice between weekly voice therapy sessions delivered through telehealth to children with voice disorders. This in-between care consisted of supported home practice that was remotely monitored by speech-language pathologists (SLPs).
Methods:
A web-based voice therapy portal (VTP) was developed as a platform so participants could complete voice therapy home practice by an interdisciplinary team of SLPs (specialized in pediatric voice therapy), telehealth specialists, biomedical informaticians, and interface designers. The VTP was subsequently field tested in a group of children with voice disorders, participating in a larger telehealth study.
Results:
Building the VTP for supported home practice for pediatric voice therapy was challenging, but successful. Key interactive features of the final site included 11 vocal hygiene questions, traditional voice therapy exercises grouped into levels, audio/visual voice therapy demonstrations, a store-and-retrieval system for voice samples, message/chat function, written guidelines for weekly therapy exercises, and questionnaires for parents to complete after each therapy session. Ten participants (9–14 years of age) diagnosed with a voice disorder were enrolled for eight weekly telehealth voice therapy sessions with follow-up in-between care provided using the VTP.
Conclusion:
The development and implementation of the VTP as a novel platform for the delivery of voice therapy home practice sessions were effective. We found that a versatile individual, who can work with all project staff (speak the language of both SLPs and information technologists), is essential to the development process. Once the website was established, participants and SLPs effectively utilized the web-based VTP. They found it feasible and useful for needed in-between care and reinforcement of therapeutic exercises.
Introduction
Limited access to healthcare and specialized healthcare providers, especially speech-language pathologists (SLPs), has been the driver in the rapid growth of delivery of services through a telehealth model. 1,2 The application (app) of telemedicine in speech-language pathology has been shown to be a valuable tool in addressing the needs of both the patient and provider by a variety of research initiatives over the past two decades. 3 –9 Specific to the voice-disordered population, published data regarding the assessment and treatment by telehealth reveal increase in accessibility and availability of care with no compromise to voice outcomes. 10 Yet, few investigations have included children and none has addressed the need for a telehealth model that includes a web-based interactive home practice component.
Traditionally, voice therapy is conducted face-to-face for 30–60 min, once/week for 8–12 weeks. After each therapy session, the patient is given individualized home practice to complete over the next week. This typically consists of vocal hygiene (e.g., increase water intake) and voice therapy exercises (e.g., vocal function exercises). Home practice is presented to the patient by paper or CD/DVD, with instructions to document, in writing, each time they complete the exercises. The patient is instructed to bring the documentation back to the next therapy session so the clinician can monitor how the patient is doing while at home. Although this method works for some patients, there are several pitfalls to this practice. For instance, patients will report back that they were unable to remember how to perform the voice exercises, 11 forgot the paper at home, forgot to record when they did the exercises, forgot to do the exercises, and so on. A concern for clinicians is the patient's fidelity to the recommended home practice activities. Home practice fidelity can be affected by the patient's adherence to home practice recommendations and compliance with practice frequency and duration. It has been reported that unsupervised home practice is the least effective type of exercise program for some individuals, when compared to individual and group programs. 12 Home practice is important because it provides opportunities for the patient to work on, improve, and generalize concepts learned in the therapy setting, key components to the success of a behavioral-based intervention such as voice therapy. Therefore, discovering ways to improve delivery mechanisms and adherence to home practice are warranted.
Supported in-between care is a form of home practice we developed that enabled clinicians to remotely review participants' home practice progress and monitor the patient's adherence between synchronous therapy sessions. Today, patients have access to computers, mobile phones, the internet, and videoconferencing software that permit audio and visual interaction. These versatile and inexpensive tools permit clinicians and patients to interact virtually. Furthermore, web-based tools also provide a conduit for accessing educational materials. Currently, public and some private schools are utilizing specialized web portals to facilitate home study. The extension of a web-based portal for therapy-based home practice is in line with current education practices and may improve patients' home practice fidelity by regulating home practice.
Apps on various devices provide excellent tools for monitoring patients' progress, including self-monitoring and remote monitoring. Boster and McCarthy conducted a small focus group to discuss and evaluate novel interface designs of interacting with three different modes: communication, plan, and incentive systems, for children with autism spectrum disorder. Such tools may provide an excellent capability for provider, patient, and parent. 13 Furlong et al. evaluated and analyzed current apps for Android and iOS mobile phones and tablets using a structured quality appraisal tool. 14 The evaluation included the following elements: (1) engagement, (2) functionality, (3) the look and feel of the app, (4) quality of information, and (5) the impact. A protocol was developed from the appraisal tool and this can be used by SLPs in reviewing apps in clinical practice.
Hill et al. studied asynchronous telerehabilitation in SLP by evaluating the usability of Enabling Speech and Language Therapy (eSALT) in adults with aphasia. 15 This research showed that technology refinements must occur with end-user input. In addition, the iPad-based Constant Therapy reported on by Kiran et al. showed great promise for remote monitoring as well. 16 Pulga et al. evaluated technology apps for SLP in Brazil, where two groups were evaluated, one with technology and one without. 17 The group with the technology showed improved performance.
Web-based tools have also been shown to be effective in speech training. In their 2010 article, Beijer et al. discussed the use of the web for patients with dysarthria in the Netherlands. 18 They used e-learning-based speech therapy (EST), which permitted the patient to maintain their rehabilitation after face-to-face sessions were complete. Patients and SLPs will gain additional knowledge as the telecommunications and mobile apps that operate personal computing devices become commonplace.
Methods
Recently, a team of SLPs, information technology (IT) experts, clinical researchers, and telehealth experts from the University of Cincinnati and Cincinnati Children's Hospital Medical Center (CCHMC) conducted a 2-year Agency for Healthcare Research and Quality (AHRQ) study (Access to Quality Pediatric Voice Therapy) to assess a telehealth solution. This study was approved by the Institutional Review Boards of the University of Cincinnati and CCHMC.
The main objective of the study was to determine the feasibility of using a synchronous telehealth solution for delivering in-home pediatric voice therapy through secure teleconferencing and asynchronous web-based systems. The motivating hypothesis was that an informed, feasible, and personalized approach to pediatric voice care through telehealth is possible and would result in improved patient access to quality care, while encouraging greater self-management and clinical monitoring. The research team believes that this model of service delivery can be used to consistently deliver a high standard of care, evaluate treatment outcomes, and reduce the chronic nature of childhood voice disorders, all the while providing relief of the family's burden related to access, travel, and the complex nature of family schedules and scheduling therapy.
This article focuses on the design and implementation of a web-based asynchronous voice therapy portal (VTP) for supported home practice. The VTP provides an opportunity to complete home voice exercises and is an easy link between the patient and provider in between therapy sessions. The VTP was developed for participants to access at home through the internet and complete their voice exercises (versus the traditional paper documentation). To accomplish this, our group in collaboration with a team of bioinformatics specialists, envisioned, designed, and deployed a practice portal for participants in this study.
VTP Design Process
The multidisciplinary team developed the functional requirements for the web portal, and they developed a series of paper-based and electronic prototypes to refine the details of the design. A series of usability tests with volunteer patients and clinicians to enhance the ease of navigation and clarity of the user experience was conducted.
Initial meetings determined what the researchers and clinicians envisioned the VTP to include: (1) Participant web session to be informative and interactive; (2) Data elements collected to be stored and retrieved by both the study staff and participant; (3) A message or chat function that permits secure communication between parent/participant and clinician; (4) Store and retrieval system for voice samples; and (5) Operations management for setting up accounts, granting permission, and other activities related to account management.
Subsequent meetings focused on how to incorporate these elements into the web-based platform and the overall visual design of each web page. The participants' age range (8–15 years) was considered when designing the visual and functional aspects of the web page. Additional details specific to accessing the web portal from outside the CCHMC firewall, and the content each user would have access to (administrators/clinicians, patients, and parents) were also discussed. Figure 1 illustrates the overall process of the development of the VTP and Figure 2 illustrates the final VTP system structure.

Workflow of design and development of the web portal.

Web portal system design.
Design of VTP Therapy Modules
Overall structure and flexibility of the therapy modules were essential components when designing and developing the web portal. Although voice therapy protocols typically have specific steps to follow, it was vital to group the steps into levels to allow for ease and clarity of communicating to the patient what exercises needed to be completed for the week. These levels also provided a visual indicator for progression through voice therapy. Pediatric SLPs and clinical researchers, each of whom had over 8 years of experience with pediatric voice therapy, grouped vocal function exercises and resonant voice therapy techniques into levels, based on their clinical experiences. The final therapy design included vocal hygiene questions followed by warm-up exercises, three levels of voice function exercise, and four levels of resonance voice therapy.
Once the levels were established, content of each web page was determined. This included instructions for each exercise, examples of how to complete the exercise through video demonstrations, and a timer to measure sustained phonation for the vocal function portion of the exercises. Because of the participants' age range, two VTP visual interfaces were developed: one for children (8–12 years) and one for adolescents (13–15 years). The two interfaces had the same functionalities, but differed in graphics and video demonstrations. For example, the children's VTP graphics depicted children and the video demonstrations were performed by children of a similar age (∼8 to 12 years), while adolescent performers were used for the adolescent video demonstrations (Fig. 3).
User log-in.
The VTP logged all electronic data, including responses to vocal hygiene questions, what voice exercises were completed, duration of certain tasks (e.g., sustained phonation), length of time spent on VTP overall, and parents' survey responses (surveys were related to the VTP's ease-of-use, burden, and cost). Once the web portal was finished and internal testing was complete, recruitment for the larger telehealth project began and the web portal went live.
Participants
Participants were recruited from the CCHMC Pediatric Voice Clinic and who were referred for voice therapy. Etiology of the voice disorder was not an inclusion or exclusion factor. Participants were to be between the ages of 8 and 15 and live within 100 miles of the hospital. Participants who did not have internet access or a hardwired internet connection were ineligible to participate. All participants and their parents signed consent forms approved by the University of Cincinnati and CCHMC IRBs. The project consisted of synchronous telehealth therapy sessions and asynchronous home practice sessions using the VTP.
VTP Implementation
Before the start of the therapy sessions, the study coordinator and information system team visited the participants' homes to install the computers and train the participants and their families on how the system worked. A test session between the participant and the treating clinician was conducted before the team left the house. Families were also provided a user guide to follow for reference, which provided instructions on how to access and navigate the VTP * (Fig. 4).
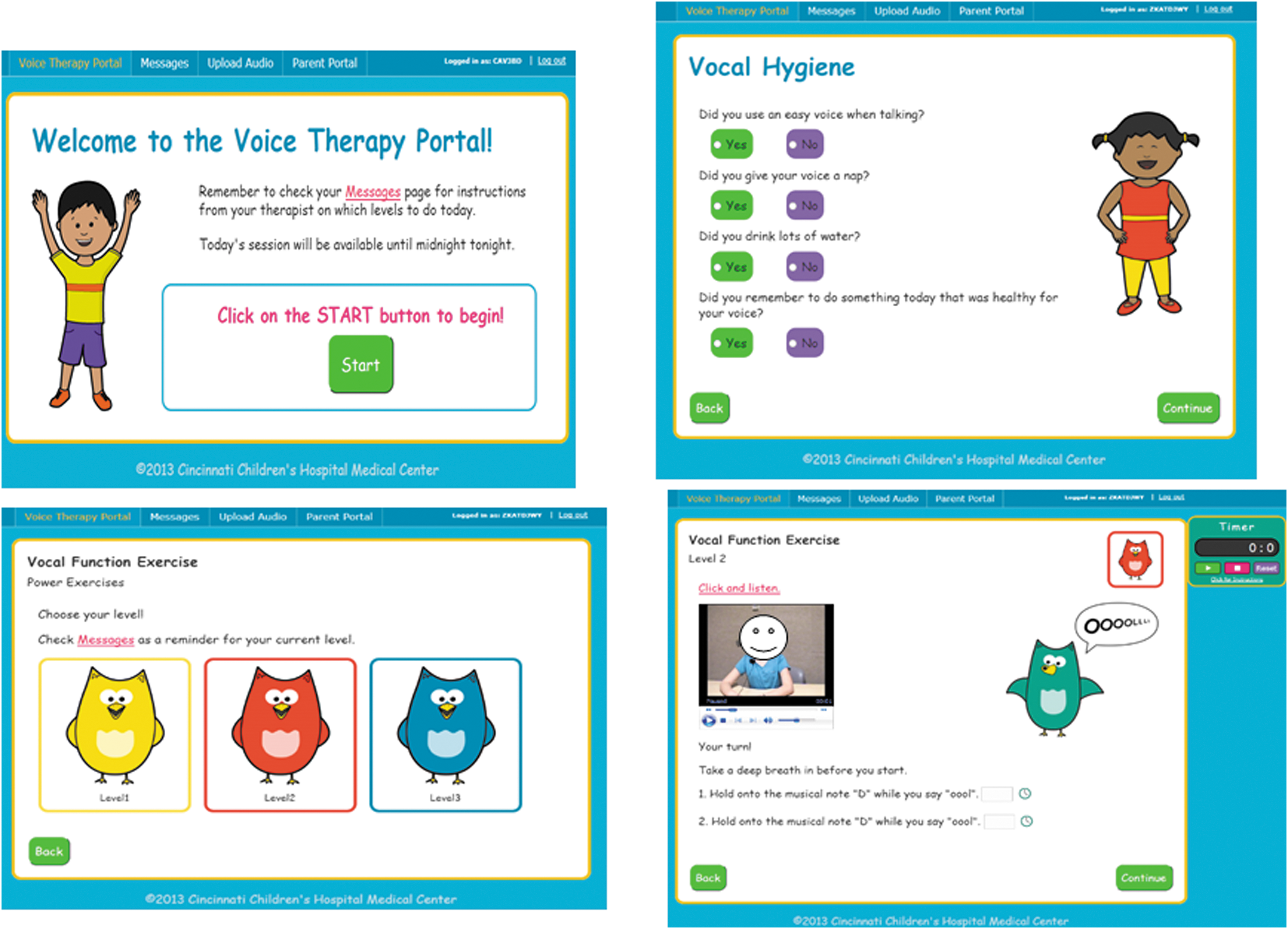
Voice therapy portal sample pages upon launch of
Each participant had a weekly synchronous voice therapy session with their SLP. Following this therapy session, the participant was instructed by the treating SLP to complete specific voice exercises at least 5 days/week, on their own, using the VTP. The VTP logged all the activities the participant completed.
Results
Implementation
The VTP had no significant issues when it went live. Participants and parents were able to access the VTP with ease and had the ability to complete the exercises as intended. Ten children (five male; five female), aged 9–14 years (median age 11.1), participated. Utilization of the web portal by the participants varied. Overall, this group practiced an average of 4 days/week (range 2.5–6.8); practiced an average of 27.5 out of a recommended 40 days (range 10–45); spent an average of 30.14 min/practice session (range 27–36); and had an average of 3.3 days when they logged on, but did not do anything (range 0–10). Overall, parents filled out each of the 4 questionnaires between 7 and 36 times, indicating variability. Over the 8 weeks, on average, parents reported that their child adhered to the therapy practice recommendations “a lot,” 63.4% of the time; “quite a bit,” 28% of the time; “somewhat,” 7.5% of the time; and “not at all,” 0.5% of the time. Qualitatively, the child participants reported enjoying the VTP's messaging system, which allowed asynchronous communication with their clinicians throughout the week. Similarly, the clinicians also found the messaging system helpful because it allowed them to send participants any additional directions needed to accurately complete the home program. Although the clinicians appreciated the VTP's home practice monitoring capabilities, they admitted that they needed reminders to go in and check activity through the week.
Discussion
This is the first report of the development and implementation of a home practice web-based construct specific to pediatric voice therapy. The idea of supported home practice or in-between care not only pertains to home practice for the participants but also the idea that the clinician is able to review progress made on specific home practice activities (e.g., voice exercises) and monitor the participant's adherence throughout the week, which can be advantageous for both the participant and the clinician.
We identified several major lessons from our experience developing the VTP.
(1) Regarding the development, having an individual on the team who understands each professions' (programming, design, and content) terminology is essential. This allows all team members to communicate effectively and focus on their specific area of expertise, rather than spending time establishing common understandings.
(2) It is essential to specify the theoretical foundation of the therapy program you wish to use. By nature, the website design does not facilitate the type of dynamic flow and individualized home practice regime available with the in-person therapy/home practice model; therefore, establishing the therapy program and identifying all the required features accessible to the participants is crucial.
(3) The team should develop clear expectations of each team members' responsibilities. For instance, graphic design team members relied upon the SLPs to create image and storyboard drafts to serve as models when developing their vision of the VTP visual interface. The SLPs, however, anticipated members from the graphic design team proposing these image and storyboard ideas to the SLPs.
(4) The project budget and timeline should be expanded. Our final VTP was over budget and took more time to complete than expected. Although some budget overages (e.g., inaccurate quotes) and delays (e.g., turnover of personnel) were out of the teams' control, others were the result of lessons 1–3.
Once the VTP was developed, implementation went smoothly. Although participants utilized the VTP to various degrees, home practice did occur with each participant. At this time, the lack of published data regarding percent adherence and activity with traditional pencil and paper home programs makes it difficult to draw direct comparisons with the performance demonstrated by our participants. Importantly, participants and parents did not report any significant technical issue and, in fact, stated that it was easy to use, had few technical problems, and enjoyed using the VTP. Clinicians indicated they liked the VTP; however, there was a learning curve with getting in the routine of reviewing each participant's web portal activity in between sessions. This may be because with the traditional therapy model, the clinician sees the patient once/week and then provides their homework on paper, with no contact until the following week. In other words, there is no system in place for the clinician to go check how the patient is doing or a platform where the patient or parent is visiting on a daily basis and has the ability to ask questions as needed. This idea of in-between care will become more important as web-based capabilities and models expand.
One issue that arose was that of knowing if the participant did the correct recommended therapy activities (i.e., accessed the appropriate set of exercises the SLP stated). Because the recommended therapy activity was provided at the end of the synchronous therapy (and not always reported to the participant on the message board), a reference to what weekly therapy levels to access was not always available in real time, but could be accessed later. An additional issue pertained to whether the participant actually completed the voice therapy exercises (or did they just click through) or just let the timers run for some amount of time. The timers associated with the sustained phonation tasks were click activated not voice activated. However, this last point is not inherent to this model and can arise with paper form. The benefit of the VTP is that it does have a time stamp (log-in and log-out time) that identifies the participant did actually log in.
Future directions will focus on additional items for participants to access on the web portal and reminder systems. Items for the participant to print off to supplement the home practice exercises provided on the VTP may be beneficial. In addition, a reminder system (e.g., automated e-mail, telephone messages, and texts) that prompts participants to complete their home practice may be helpful. This system could be set up to initially remind the participant, and then gently remind them if they missed a practice day. The ability to do more tracking of activity in real time on all the web pages needs to be incorporated into a next design. Last, a comparative study looking at the adherence of a paper-based home practice model versus web-based is important to define the effectiveness of the model.
Conclusions
New approaches in clinical care, using the internet and web-based tools, can ameliorate many of the challenges patients and their families face. Over the past decade or so, the integration of computers and mobile devices has been shown to be very effective in treating patients with speech language disorders. 3,4,19 –21 This is the first report of a web-based home practice platform for children and adolescents with a voice disorder. Although the design of the VTP has some challenges, overall development and implementation of the home practice web portal were successful. Results indicate child- and adolescent-directed voice and other communication therapy home practice portals have the potential for effective and meaningful utilization.
Footnotes
Acknowledgments
This project was funded under contract/grant number 1R21 HS21781-0109 (2012–2014) from the AHRQ, U.S. Department of Health and Human Services. The opinions expressed in this document are those of the authors and do not reflect the official position of AHRQ or the U.S. Department of Health and Human Services. The authors acknowledge Janet Beckmeyer, MA, CCC/SLP, Kathryn Davidson, MA, and the CCHMC Information Systems and Biomedical Informatics personnel for their time, help, and insight into the design and execution of the web portal.
Disclosure Statement
No competing financial interests exist.
*