
Abstract
Introduction
Blood pressure (BP) is a vital measure. It reflects the BP against artery walls when the heart beats, known as systolic blood pressure (SBP), and the pressure when the heart is at rest, also known as diastolic blood pressure (DBP). It allows to monitor strokes, hypertension, and other cardiac diseases, and is expressed as SBP/DBP mmHg.
BP can be measured with two types of blood pressure monitors (BPMs): Wrist blood pressure monitor (W-BPM): it measures BP at the wrist level. Upper-arm blood pressure monitor (U-BPM), also known as cuff BP monitor: it measures BP from the upper arm.
Most manufacturers produce and commercialize both models. However, since W-BPM tends to overestimate BP, 1 the European Society of Cardiology, and other learned societies, recommend using U-BPM. 2 Now, W-BPMs are more intuitive and user friendly than U-BPM and, so, it is important to use them in the best conditions to minimize overestimation. W-BPMs are also cheaper. We analyzed 130 BPMs that can be obtained on Amazon.fr using the key phrase “blood pressure monitor.” Forty percent of these devices are W-BPMs. In addition, the average price of a W-BPM is 29.18 ± 14.92 €, whereas the average price of U-BPM is 48.18 ± 35.1 €.
To measure BP properly, the BPM must be positioned correctly. As a matter of fact, Deutsch et al. demonstrated that measurement accuracy could be improved by guiding patients to position correctly their arm when using a W-BPM. 3 The device should be 2 cm away from the wrist joint, the hand palm side up, and the BPM device must be facing upright at the heart level, which corresponds to an angle between 10° and 30° in regard to a horizontal plan. The patient must sit still during the measure. 4
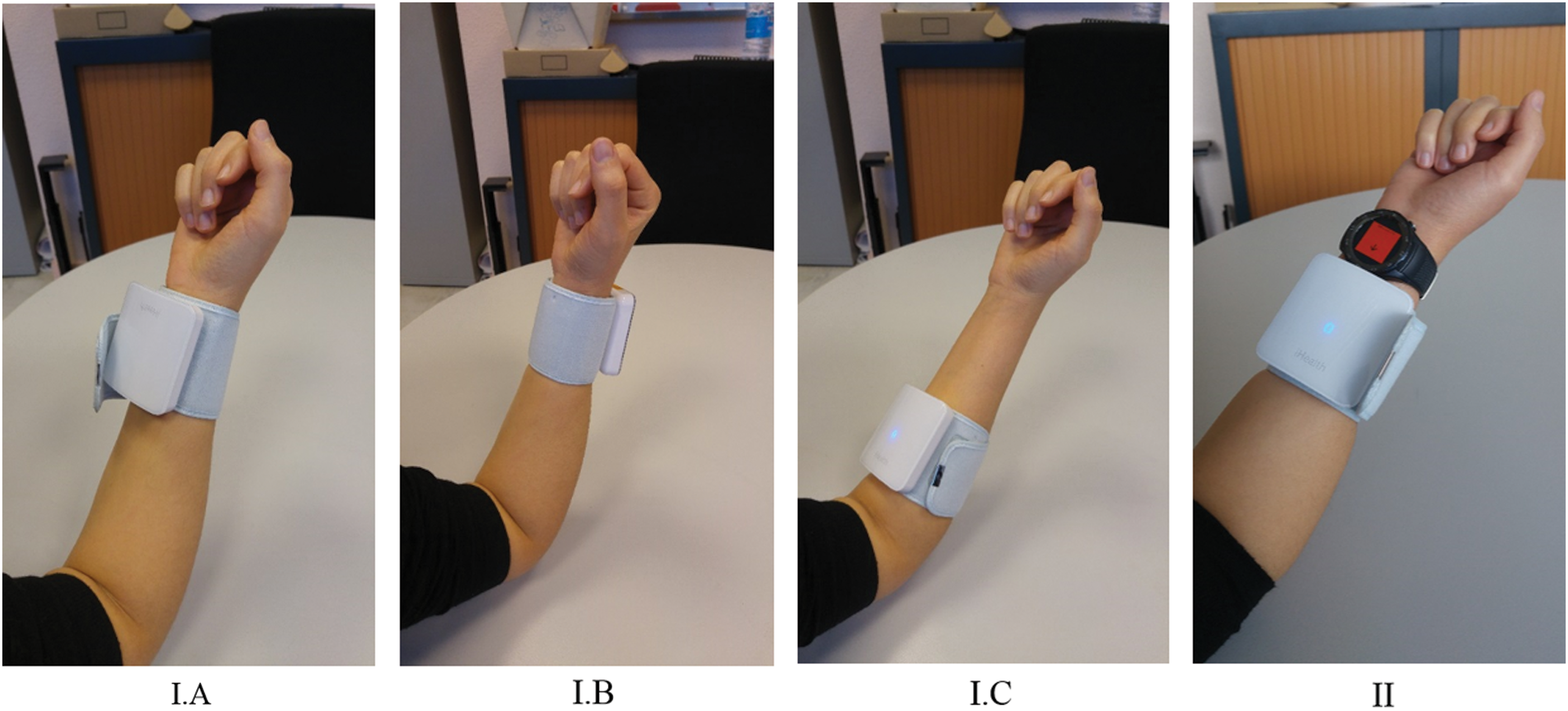
Measuring BP without respecting these instructions might result in erroneous measures, 5 influencing badly the medical diagnosis or follow-up. Even if some manufacturers added an angle sensor to W-BPM to check the device position to help patients in taking their BP, this is not sufficient. As a matter of fact, the angle sensor can read an acceptable angle, between 10° and 30°, whereas W-BPM can be positioned incorrectly. For instance, Figure 1 illustrates two incorrect positions that current BPMs cannot detect.
In this work, we propose to fill this gap by combining a BPM with a connected smartwatch, integrating an Attitude and Heading Reference System (AHRS) algorithm to help the user to position correctly the device and, therefore, perform a BP measure in proper conditions.
Materials and Methods
To perform a reliable BP measure, the BPM should be rightly positioned. In this section, we detail which sensor is used and how its position is determined.
Materials
The sensor used in this work is iHealth® BP7. It is a W-BPM certified as medical device. Medical devices are certified by the European directive 93/42/CEE, which guarantees their reliable and safe use for medical diagnosis and treatment aims. 6 Another important characteristic of connected devices concerns their interoperability, defined as the ability of two or more systems or components to exchange information and to use the information that has been exchanged. 7 While connected sensors market, also known as internet of things, keeps expanding, manufacturers are more likely to privilege their proprietary communication protocols to standard ones in their products. This makes exchanging data between sensors from different producers more difficult. 8 Indeed, a recent study showed that among 92 health sensors, only 40% provide a Software Development Kit (SDK) or an Application Programming Interface to exchange their data with other platforms. 9
A sensor is naturally interoperable with its own smartphone application companion, but not necessarily with third-party systems. In this study, we wanted to cope with this notion of “open-interoperability,” which means that an open-interoperable sensor is able to communicate its data to other systems than its manufacturer. The iHealth BP7 is open-interoperable since any one can retrieve its data as well as control it. As a matter of fact, iHealth provides an SDK to communicate directly with the sensor, which enables us to access a set of functionalities like starting and stopping the measure, reading measures history, getting battery level, and so on. Direct communication with sensors allows also protecting user's privacy, as it prevents third parties from accessing data.
In addition to the BPM, we used the smartwatch Huawei® Watch 2 (HW2) powered by a Qualcomm Snapdragon Wear 2100 CPU rated at 1.2 GHz and running Android Wear 2.0 as an operating system. Among integrated sensors, it has a heart rate monitor, a GPS/GLONASS chip for geolocation, an accelerometer, a gyroscope (ST LSM6DS3), and a magnetometer (AKM AK09911). It is powered by a 420 mAh battery. It has Bluetooth and WiFi capabilities. Therefore, it can be used independently from a smartphone.
Methods
As described previously, to determine if W-BPM is positioned correctly, we need to calculate the device orientation. This can be done by the fusion of at least two sensors: an accelerometer and a magnetometer. A gyroscope can also be added for more precision. Many algorithms allow to calculate device orientation. Michel et al. 10 compared several algorithms. 11 –15 They concluded that, globally, Fourati et al.'s 13 and Martin and Salaün's 15 algorithms are the best ones. The comparison of attitude estimation by each algorithm is detailed in Table 1. Regarding power consumption on battery-powered devices, they recommended implementing Madgwick's algorithm, which uses three sensors: accelerometer, gyroscope, and magnetometer. The gyroscope consumes more energy than an accelerometer or a magnetometer. Therefore, we compared Madgwick's algorithm consumption, which needs the three sensors (accelerometer, gyroscope, and magnetometer), to Android orientation algorithm consumption, which needs only an accelerometer and a magnetometer. We used Battery Historian tool to estimate sensors consumption. Even if it delivers an extremely rough estimation, it can be considered to evaluate the relative performance of both methods. Table 2 shows their power consumption average measured over 10 min. Measures were repeated thrice. We observe that Android algorithm consumes 70% less power than Madgwick's algorithm. This is due to the absence of gyroscope. In our development, we retained Android algorithm to estimate the orientation of the W-BPM. As a matter of fact, the accuracy difference between Android algorithm and Madgwick's one is only 3.42°, which can be admissible for human movements. Consequently, the Android algorithm was programmed on the smartwatch. Acceptability was studied using a survey, including Likert scale-based questions LS−2:2 (−2: strongly disagree, −1: disagree, 0: neither agree nor disagree, 1: agree, and 2: strongly agree). ANOVA was used for statistical analysis.
Comparison of Attitude Estimation by Each Algorithm
Extracted from Michel et al. 10
MAE, Mean Absolute Error; QAD, Quaternion Angle Difference; STD, Standard Deviation.
Power Consumption for Madgwick and Android Algorithms Over 10 Min
Values are expressed in milliampere hour (mAh).
Results
We developed an Android Wear application implementing Android algorithm 16 and running on the HW2 smartwatch. It integrates iHealth SDK to communicate with the BPM directly. The set of devices is worn as shown in Figure 1.II. The application was tested on 30 individuals (average age 31.63 ± 8.89, 53.3% female), among which 96.7% have a smartphone and 33.3% wear a watch. When asked which type of BPM (U-BPM vs. W-BPM) they preferred to employ, 66.7% of them indicated the W-BPM. No significant correlation was found between the sensor type choice and age (p = 0.465), gender (p = 0.804), or educational level (p = 0.785). After being told how to use this device, they tested two scenarios. The first scenario consisted in testing the W-BPM with the smartphone. This is the standard way for manufacturers to develop their BPM devices. The second scenario consisted in combining the W-BPM with the smartwatch (including Android algorithm) to determine if a smartwatch, placed on the same arm as the BPM, can provide better feedback of a BP measure. The aim of this experiment was to determine if a smartwatch is more user friendly than a smartphone in giving the user a better feedback to correctly position W-BPM.
After the experiment, the participants were asked several questions about how they perceived our application. We observed that 96.7% of participants judged that it was useful to be guided to position correctly the BPM. Before the experiment, all participants received clear oral instructions to use the W-BPM correctly. Now, after the experiment, when they were asked to recite them, 83.34% of them should admit that they were not able to do it, which confirmed our conviction they have to be guided.
Regarding experimented scenarios, 83.3% of participants preferred using the smartwatch to control the BPM instead of the smartphone. No significant correlation was found between this choice and age (p = 0.24), gender (p = 0.833), or educational level (p = 0.684). Users were guided with arrows to position correctly their arms. Different reasons were mentioned to justify the smartwatch preference, for example, “….less devices to handle since I'm wearing already a watch,” “….it is more intuitive to adjust my hand when having the feedback from the watch itself.” As for the graphical user interface, smartwatch feedback (LS−2:2 = 1.067 ± 0.944) was globally preferred to the smartphone one (LS−2:2 = 0.7 ± 0.988).
Discussion
The AHRS algorithm we implemented detected easily positions I.A and I.B described in Figure 1 and the smartwatch did not activate the BPM in these positions unlike current solutions on the market. This was made possible, thanks to the fusion of an accelerometer and a magnetometer. Current commercialized W-BPMs include only one accelerometer, which is unable to detect these incorrect positions without combining the accelerometer with a magnetometer. Position I.C cannot be detected using AHRS. However, we noticed that, when the smartwatch was used to perform the measure, all participants positioned—quite naturally—the BPM next to the watch, which limited noticeably this issue. A large number of health manufacturers commercialize both BPM and actimetry sensor in the form of wristband or smartwatch. Therefore, they can add a physical switch that prevents BPM from performing a measure unless it is well positioned. Regarding the acceptability of the developed solution, most participants (all age, gender, and educational level combined) agreed that the smartwatch scenario was more pleasant than the smartphone one. Statistical analysis confirmed that this choice was not influenced by age, gender, or educational level.
To the best of our knowledge, research studies on BP monitoring in the literature have been done using a U-BPM in compliance with international recommendations. 2 Wagner et al. have used the Microlife® BP A100 U-BPM to conduct a study in which pregnant diabetic patients had to self-measure their BP. 17 In a second study, 18 they have employed the A&D UA-767PBT U-BPM to measure the adherence of hypertensive patients to a BP self-measurement system. In a similar work, 19 Evans et al. have used the same BPM model to evaluate the adherence of older adults to remote health monitoring systems. Kusk et al. 20 have integrated also the A&D U-BPM in the development of a context-aware system to help patients take a reliable BP measurement, while respecting international guidelines. Researches involving W-BPM aimed to evaluate the accuracy of devices. For instance, in Wang et al., 21 it was proven that iHealth BP7 BPM could be recommended for self-measurement in an adult population. In Kang et al., 22 the same conclusion was obtained on AVITA® BPM15S for home use. In the same manner, Deutsch et al. 3 concluded that the dedicated positioning sensor function in Omron RS6 was an important function in improving measurement accuracy and could be recommended for home BP measurements where the accuracy and reliability of the device are imperative. However, as mentioned previously, this sensor cannot detect incorrect positions as illustrated in Figure 1-I.A and I.B.
Our developed solution can help patients in positioning any W-BPM even if this device does not integrate sensors to detect BPM position. Furthermore, it can prevent incorrect positions as illustrated in Figure 1-I.A and I.B.
Conclusions
In this work, we developed a smartwatch application that can be downloaded by wide public to help users position any wrist BPM correctly using AHRS. Results showed that a majority of them preferred W-BPM (all age, gender, and educational level combined) and that the proposed solution helped them position the W-BPM correctly in a user-friendly way.
Footnotes
Acknowledgments
We would like to thank Pr. Dominique Somme for his fruitful discussions. This work was supported by ANRT (Contract No. 915/2015).
Disclosure Statement
No competing financial interest exists.