
Abstract
Background:
Use of technology in language rehabilitation has grown significantly in recent years, and there is increasing evidence of its effectiveness in the treatment of poststroke aphasia. Technology has the potential to foster intensity and repetition by enabling people with aphasia to improve their skills without the constant presence of the clinician. The main objective of this article is to review and illustrate key factors for the success of self-administered treatments of poststroke aphasia using technologies.
Methods:
We briefly reviewed technology-based treatments of aphasia and described three determining factors for the success of self-administered treatments delivered by technology, namely, treatment-related, technology-related, and patient-related factors. Two clinical cases were also presented to illustrate issues and challenges related to the various factors to be considered before proposing such treatments.
Conclusions:
Self-administered treatments of poststroke aphasia using new technologies enable patients to be more independent in their rehabilitation and to benefit from more intensive and extended treatment. These benefits are important in the current economic context, where human and financial resources for clinical practice are limited. Speech-language therapists should consider these opportunities and propose new methods to deliver attractive and intensive treatments of poststroke aphasia.
Introduction
The main objective of this article is to review and illustrate key factors for the success of self-administered treatments of poststroke aphasia using technologies. Aphasia is an acquired language disorder resulting from an injury to the brain. In the majority of cases, the disorder is caused by stroke, which is the leading cause of long-term disability. 1 About one-third of people affected by stroke suffer from aphasia at onset, and 60% of them have chronic aphasia 12 months postonset. 2 In addition, poststroke aphasia is associated with high healthcare costs. 3
Aphasia symptoms can range from mild to severe and affect functional communication to varying extents. The severity of aphasia depends on factors such as the location and extent of brain damage, presence of concurrent disease, and cognitive impairment. People with aphasia may experience mild-to-substantial difficulties in the production or comprehension of language, as well as in the ability to read or write. Since language is at the heart of human communication, aphasia has a significant impact on the lives of those affected and their families. 4 Negative repercussions include emotional distress and depression, 5 poorer quality of life, 6 and social isolation. 7
The prognosis for aphasia depends on a number of stroke-related and patient-related factors, as well as on speech therapy. 8 However, in the actual health context, the availability of speech-language therapy services remains insufficient to meet the need of people with chronic aphasia. The use of technology (i.e., computer and smart tablet) in language rehabilitation has grown significantly in recent years and provides new possibilities to overcome this lack of services. Moreover, there is increasing evidence of its effectiveness in the treatment of poststroke aphasia. 9,10
This article is structured as follows: first, technology-based treatments of aphasia are briefly reviewed; second, the key factors that contribute to the success of these treatments are presented and discussed; third, two clinical cases are presented to illustrate issues and challenges related to the factors to be considered before proposing a technology-based self-administered treatment of poststroke aphasia; and finally, the article ends with a general conclusion.
The use of Technologies for the Treatment of Poststroke Aphasia
The primary objective of aphasia rehabilitation is “to help the individual achieve the highest level of independent function for participation in daily living.” 11 In their recent Cochrane systematic review on aphasia treatment, Brady et al. concluded that therapy at high intensity or over a long period may be beneficial to achieve better outcomes. 9 However, due to personnel and financial constraints, optimal treatment intensity and length is rarely observed in face-to-face treatments. 10 To this respect, the use of technology in rehabilitation might increase treatment intensity. This use has grown significantly in recent years and became a topic of interest in the aphasia domain. In 2016, Zheng et al. conducted a recent systematic review of the effect of computer therapy in aphasia. 12 They analyzed seven studies assessing the effectiveness of computer programs for the treatment of various language domains (e.g., word finding and reading comprehension) and concluded that computer therapy was effective compared to no therapy. Zheng et al. also reviewed three other studies to support preliminary evidence that computer-delivered therapy could be as effective as clinician-delivered therapy for the treatment of chronic aphasia.
Also recently, Lavoie et al. conducted a systematic review of the effectiveness of treatments delivered by technology in the management of poststroke anomia. 13 They examined 23 studies and found that computers constitute the most popular technology by far; only a few studies explored the effectiveness of other technologies such as smart tablets. All the studies examined by Lavoie et al. confirmed the effectiveness of therapy provided by technology in improving naming of trained items. 13 In some of them, technology was used as a therapy tool in a clinical setting, in the presence of the clinician, while in others therapy using technology was self-administered at home, without the clinician.
There are a number of advantages to self-administered treatments using technology. First, such treatments, self-administered by computer 14 –16 or smart tablet, 17,18 might enable more intensive and extended treatment delivery. This advantage is particularly relevant when clinical resources are limited and insufficient to meet the needs of people with aphasia, which compromises their rehabilitation potential. Moreover, getting to an outpatient clinic is sometimes difficult or impossible for people with aphasia because of mobility problems, financial constraints, need for support from a family member, distance between home and clinic, and so on. Therefore, therapy self-administered by computer 16 or smart tablet 17 –19 can expand access to treatment for these people. However, the successful use of technologies in the management of poststroke aphasia depends on various factors, which are described below, followed by clinical illustrations.
Key Factors for the Success of Self-Administered Treatments of Poststroke Aphasia Using Technologies
Various factors are known to contribute to the success of aphasia treatment. These factors are linked to the treatment itself (e.g., approach, type, goal, and intensity) and to the personal status of the participant (e.g., cognitive status, motivation, and family support). 20 In this section, we focus on three determining factors for the success of self-administered treatments delivered by technology: treatment-related, technology-related, and patient-related factors. A graphic summary of these key factors is presented in Figure 1.
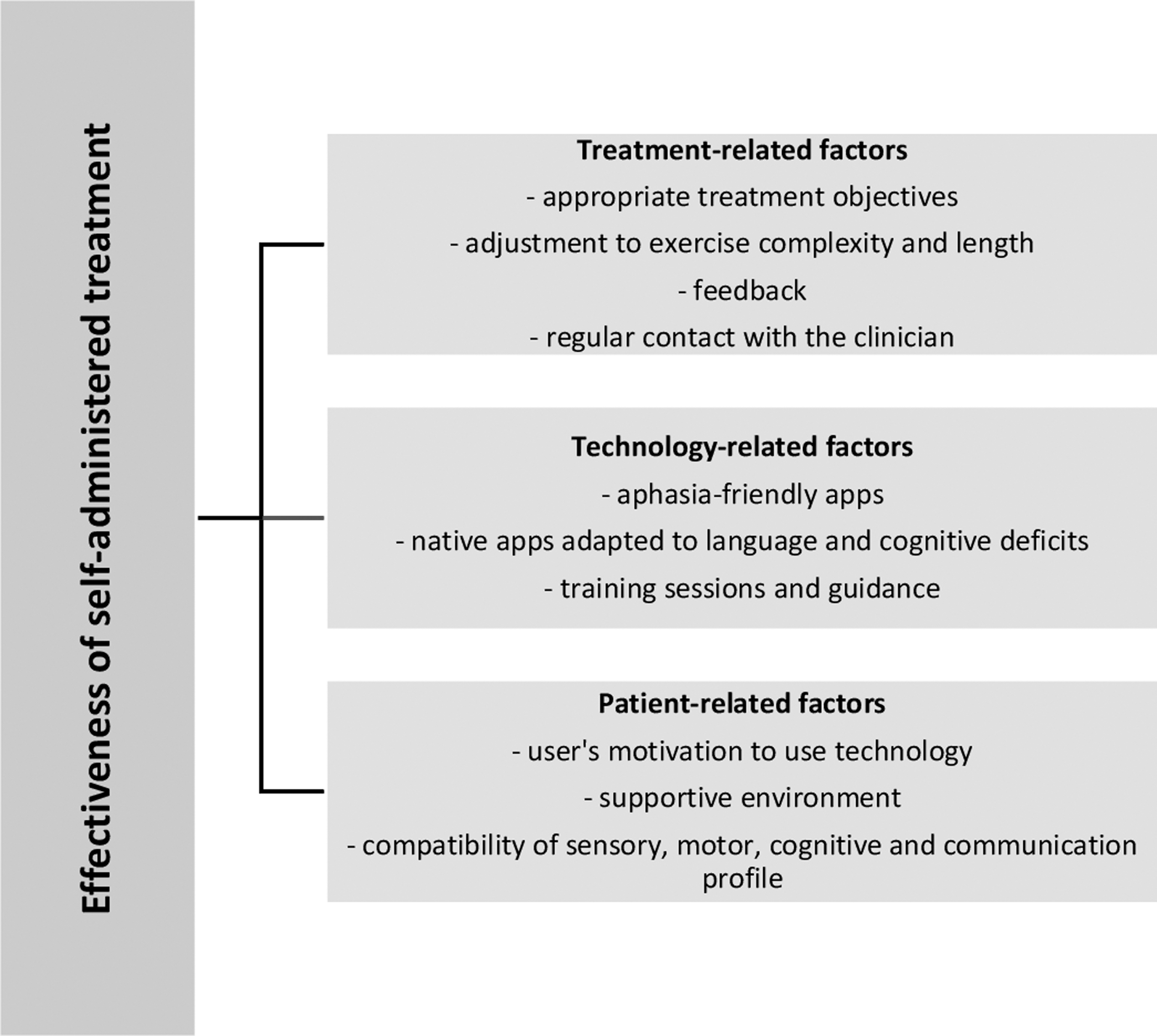
Graphic summary of key factors for the success of self-administered treatments delivered by technology.
Treatment-Related Factors
Self-administered treatment is an interesting option in language rehabilitation since it may combine two principles related to neuroplasticity after brain damage, namely intensity and repetition. 21 However, the decision to propose a technology-based self-administered treatment of aphasia must be based on specific treatment objectives, as in the case of traditional face-to-face treatments. This treatment is particularly well suited for language stimulation. For example, various apps can be used to enable the patient to practice language abilities through stimulation exercises, such as the computer-provided reading treatment used by Katz and Wertz. 22 In this multisite randomized control group study, 55 individuals with chronic aphasia used computer reading treatment software, 3 h per week for 26 weeks, consisting of 32 activities involving visual matching (e.g., letter, number, and word matching) and reading comprehension (e.g., words, sentences, and questions) of various levels of difficulty. Compared to computer nonlanguage stimulation and to no treatment at all, the computer reading treatment displayed significantly more improvement on standardized measures of communication and language.
For similar reasons, speech-language treatments delivered by technology also lend themselves well to cognitive-oriented treatments (i.e., treatments based on cognitive neuropsychological models of language), such as reactivating the spoken, for example, 19 or written form, for example, 18 of words in the case of lexical access deficits, improving sentence comprehension and production in agrammatic aphasia, 23 improving reading in acquired alexia, 24 etc. Apps could also be used effectively to enable patients to relearn linguistic rules and procedures, such as grapheme-to-phoneme conversion rules involved in reading, phoneme-to-grapheme conversion rules involved in written spelling, or inflectional rules involved in verb conjugation. Self-administered treatments using technology are particularly well suited for such relearning involving many steps and multiple graded exercises. Compared to other treatment types, relearning rules and procedures has the great advantage of being transferable/generalizable to every context to which the rule or procedure applies. To the best of our knowledge, no study on this topic has been conducted to date.
In traditional face-to-face treatments, the clinician continually adjusts task difficulty based on an ongoing online analysis of the individual's performance and progress, fluctuation in attentional abilities, discouragement, etc. Such supervision cannot be provided in self-administered treatments using technology. Therefore, before the beginning of the treatment, exercise complexity and length must be precisely determined and adjusted to each patient. In the majority of cases, self-administered treatments are implemented after traditional therapy delivered in the clinician's office, thereby facilitating the adjustment of complexity level and exercise duration.
Feedback is another important factor in the success of speech-language therapy. Various studies have shown the importance of providing feedback for language recovery in aphasia. 25 Feedback is not always imperative; other studies have reported significant language improvement following simple associative learning through repetition 26 or following errorless and errorful learning. 27 Various mediums (e.g., icons and written or spoken message) should be used as far as possible to provide feedback in self-administered treatments using technology. Although feedback is possible in these treatments, it cannot be as specific and adjusted as that provided directly by the clinician. For that reason, these treatment types are not well suited to therapies in which the active presence of the clinician is essential to provide feedback and demonstration, such as those aimed at improving articulation, comprehension, or production at the discourse level, pragmatics, etc.
Regular contact with the clinician is also an important key factor in self-administered treatments using technology. Without such regular contact, adherence to the treatment could be compromised. For example, in their randomized controlled trial designed to measure the effectiveness of a self-managed computer treatment of aphasia, Palmer et al. reported that three of the four participants who did not practice at the recommended frequency did not receive contact and support from volunteers. 28 These researchers suggest volunteer support to foster the continued practice of self-administered treatment by computer. Finally, regular contact with the clinician may also help minimize the fact that these treatments provide less control over how long and how often people do the exercises, as well as the negative influence of other factors (such as a noisy environment) and other sources of distraction (e.g., pop-up windows and on-screen and sound notifications).
Technology-Related Factors
Technology is evolving at a very rapid pace, and it is difficult to keep up to date on new devices and new apps. To date, the computer has been the most commonly used device to deliver treatments in studies using self-managed speech therapy for aphasia. 13 However, smart tablets are making their way into rehabilitation research and clinical practice. Because of their portability, ease of use, and control, these devices have many advantages over computers, such as allowing people to do their exercises where and when they like. The use of smartphones in the treatment of acquired deficits of language is another promising avenue. For example, we recently used smartphones in two individuals with the semantic variant of primary progressive aphasia (i.e., this syndrome is a particular form of frontotemporal dementia characterized by the progressive loss of semantic memory) to help them search for information related to lost concepts, either with internet search engines or a visual dictionary. 29,30 However, to the best of our knowledge, no treatment study with a smartphone was conducted with individuals with poststroke aphasia.
There are various apps specifically designed for aphasia, such as Naming or Reading TherAppy (Tactus Therapy Solutions) or Constant Therapy (The Learning Corp), that can be used to stimulate language functions with the aim of restoring or facilitating abilities. The features of these aphasia-friendly apps are generally adapted to language impairment (short messages, simple language, unequivocal icons and thumbnails, etc.). Native apps, not specifically developed for rehabilitation, can also be used for people with aphasia. For example, Routhier et al. 19 and Lavoie et al. 18 inserted stimuli in a PowerPoint presentation in the self-administered treatment of poststroke anomia using a smart tablet. In every case, the usability of technology must be established for each patient by identifying the best technology device and most adapted app, including the need for internet access.
No matter what is chosen, users with aphasia must have training sessions to teach them how to use the device and the app, as was done in both the Routhier et al. 19 and Lavoie et al. 18 studies. These sessions should be individually tailored to the specific needs and particularities of users. Ideally, the training sessions should be made in person to intervene directly on specific difficulties the participant may encounter and answer his/her questions. Participants should be guided through each step, for example, using an errorless learning method, 31 until they are able to complete the process without help. Users should also be given a reference guide with illustrated steps and simple instructions. The application must be easy to use and as intuitive as possible. The interface should be designed so that only the necessary content is displayed. To maximize the potential for success, the application should be customizable so that visual and auditory aspects can be adapted to the user's characteristics. Finally, as mentioned above, the application should allow feedback (encouragement and response accuracy) when necessary and when possible. For self-administered treatments, this feedback should be directly triggered by the participant's responses to avoid the intervention of a family member.
Patient-Related Factors
Greater independence 32 and increased self-esteem 16 are important advantages of self-administered treatments, allowing patients to work independently and to choose when, where, and for how long they practice. However, such treatments may not be suitable for everyone. One of the most important factors contributing to success is users' motivation to use technology. This motivation is likely to be influenced by the perceptions they have regarding technology, a factor that is particularly relevant with older adults who were not born in a technology-driven environment. In a recent study by Vaportzis et al., a focus group was conducted with older adults and their families to identify barriers to interacting with technologies and tablets. 33 Although most participants proved willing to learn using a tablet, they worried about the lack of instructions and support. According to Ramsberger and Marie, technology-based treatments could be associated with difficulty maintaining motivation because of less clinician contact. 16 Therefore, a highly supportive environment can be a key factor for better treatment outcomes. Friend, relative, or volunteer may play an important motivating role and also serve as an intermediary between clinician and patient in the event of technical problems or difficulty with treatment exercises.
Contrary to what might be assumed, prior experience with computers is not a determining factor in the decision regarding whether a technology-based self-administered treatment should be proposed or not. 17 Of course, training sessions could be shortened and less support with technical problems be provided in situations where the participant already uses a computer or smart tablet. Finally, fatigue and interference with other commitments were the major barriers identified by Palmer et al. who studied factors associated with the acceptability of independent home-based computerized practice from the perspective of both participants with aphasia and carers. 34
More importantly, clinicians should take into account the sensory, motor, cognitive, and communication abilities of individuals with aphasia to determine the possibility of implementing technology-based self-administered treatments. Sensory impairment is common after stroke and includes perceptual deficits such as hemianopia, agnosia, and unilateral neglect. Unless very severe, these impairments are not usually barriers to technology-based treatment and can be circumvented through simple adaptations (e.g., larger text size, portrait mode presentation, response button and icons on the right or left of the screen), at least for native apps. Following a stroke, motor impairments affecting the upper limb, such as hemiplegia, hemiparesis, and limb apraxia, may also cause difficulty with using technology (e.g., typing on the keyboard and moving the mouse). 35 In such cases, assistive devices such as trackballs could be used or, more simply, touch screen computers or tablets. Poststroke aphasia is often accompanied by cognitive deficits affecting visuospatial processing, attention, executive functions, short-term and working memory, and episodic memory. 36 However, little is known about the relationship between concurrent cognitive deficits and aphasia recovery. For people with aphasia, deficits affecting attentional, episodic, and executive abilities may cause additional difficulties in participating in self-administered treatments delivered by technology. These deficits may interfere with learning the sequential steps to follow to access and use an app, as well as to complete tasks and exercises. Finally, communication abilities should also be considered in the decision to implement a self-administered treatment using technology. Due to the severity of impairment affecting comprehension, people with global aphasia may not be good candidates for this type of treatment unless they are supported by a relative or volunteer. Among difficulties affecting communication in aphasia, impaired comprehension of spoken and written language constitutes another significant barrier to such treatment.
Below, we present two clinical cases to illustrate issues and challenges related to various factors to be considered before proposing a technology-based self-administered treatment of poststroke aphasia.
Clinical Illustrations
The demographic data, language and cognitive profiles, and treatment characteristics of two clinical cases, L.M. and P.L. are presented in Table 1. In L.M., the self-administered treatment of anomia using a smart tablet resulted in significant improvement of naming, while no significant improvement following treatment was observed in P.L. The possible explanations for these contrasting results, according to treatment-, technology-, and patient-related factors, are addressed in this section.
Language and Neuropsychological Profiles of Participants
SFA, Semantic Feature Analysis.
Treatment-related factors
The self-administered treatment used with the two participants was particularly well suited for the cognitive-oriented treatment of anomia since it combined the two important principles of intensity and repetition related to neuroplasticity in rehabilitation. 21 These principles are rarely observed in traditional face-to-face treatments due to personnel and financial constraints. Moreover, feedback was provided for each of the treated words, and both L.M. and P.L. had regular contact with the clinician who came to his home once a week to measure improvement, provide encouragement, and address technical issues. These factors contributed to treatment success in L.M. However, P.L. presented with impairment of repetition and reading aloud, and he did not receive any help from a family member during therapy sessions. Therefore, the feedback hierarchy may have been less effective for him.
Even though it is not yet possible to determine precisely the optimal treatment parameters regarding frequency and intensity for each patient, therapies targeting anomia are usually intensive and long. 37 In the present case, a longer duration of therapy may have led to different and significant results in P.L., as shown by the small improvement observed at follow-up. Moreover, although an increasing cue method was used, and naming is a relatively simple task, adjusting task difficulty was not allowed in the research protocol and therefore the treatment could not be modulated according to P.L.'s progress from week to week. In clinical settings, speech-language therapists would probably have made some changes (e.g., type of treated words, nature of feedback, or number of treated words) after noticing the lack of improvement in the early weeks. The treatment targets may also explain partially the discrepancy in treatment outcomes between the two participants. For L.M., words were chosen according to his interests and activities of daily living, which is likely to have increased his motivation for the treatment. For P.L., verbs were pretargeted as part of the study in which he enrolled. However, it may not have been the best target for him, and maybe more functional words could have led to more improvement in this participant.
Technology-related factors
The self-administered treatment was delivered using an Android tablet. The custom-developed application used for the treatment in the two participants included various aphasia-friendly features such as reduction of content, use of simple words, large font, combination of words and symbols, and so on. To complete the therapy sessions, no connection to the internet was required. Participants simply had to click on the app button to open it and to click « Start » to begin the therapy. Moreover, before treatment began, L.M. and P.L. had two training sessions to increase their confidence with the smart tablet. On several occasions, they reported that they appreciated its ease of use. L.M.'s wife was present to assist him with reading, but he was very proud to manage the smart tablet by himself. P.L.'s wife was also very supportive and engaged in his rehabilitationm but the research protocol did not allow her to help her husband during exercises, what could have helped him improve more. Therefore, the discrepancy in the treatment outcomes in the two participants does not appear to be attributable to technology-based factors.
Patient-related factors
In L.M. the first factor that contributed to the success of the treatment was undoubtedly his great motivation to improve his language skills and use technology. Before the treatment, he and his wife engaged in weekly language exercises at home. The treatment self-administered with the smart tablet therefore met their needs perfectly. From the start, L.M. was positive that the treatment would help him improve. Moreover, throughout the treatment, L.M.'s wife was very supportive. In addition to assisting him in each therapy session, she motivated him and told him how proud she was of his improvement. L.M.'s cognitive profile was also a key factor to consider in the success of the treatment. His episodic memory, executive functions, and semantic knowledge were spared, which is likely to have helped him relearn the vocabulary. In addition, his metacognition (ability to understand mental processes and monitor strategies involved in the treatment) was excellent and supported relearning.
In P.L., patient-related factors are the most likely cause of treatment failure. First, individuals with anomia due to lexical impairment are usually expected to respond better to treatment than those with semantic anomia. 38,39 However, since P.L. presented with a profile of severe anomia due to lexical and semantic impairments, treatment efficacy could have been compromised. Finally, another important patient-related factor is that P.L. developed depressive symptoms during the study. These symptoms were not observed at the beginning of the study, and P.L. was very motivated by the treatment. However, each time we saw him he was very pessimistic, and, from one visit to the next, it became clearer that depressive symptoms were an issue. This observation was also corroborated by his wife. Stroke and related disabilities were still recent events in their family history and affected P.L.'s mental health. Negative affectivity is known to impact the efficacy of speech-language therapy. 40 In that respect, P.L. would have benefited more from direct, interactive face-to-face interventions with a speech-language therapist to encourage him and refer him to appropriate services if necessary rather than leaving him to do the exercises alone.
Conclusions
Poststroke aphasia has detrimental effects on functional communication, quality of life, and social roles. Therefore, in the current economic context, where human and financial resources for clinical practice are limited, it is crucial to develop new alternatives to allow people with chronic aphasia to maximize their rehabilitation potential. The use of technology in language rehabilitation has grown significantly in recent years. This article reviews key factors for the success of self-administered treatments of poststroke aphasia using technologies, including treatment-, technology-, and patient-related factors. These cost-effective treatments enable patients to be more independent in their rehabilitation and to benefit from more intensive and extended treatment. Moreover, combined with traditional face-to-face treatments, they could be particularly useful for people who have difficulty getting to outpatient clinics because of mobility problems, financial constraints, etc. It must be acknowledged that technology-based treatments do not necessarily differ from home practice in between traditional treatments. However, the preparation of homework is strenuous and time-consuming for clinicians, who, most of the time, provide workbooks, not always adapted to the patients' specific needs. The main advantage of technology-based treatments lies in allowing patients to work independently, without the support of a family member or a relative, especially when feedback is steadily provided by the application.
The clinical illustrations provided in this study are a clear and concrete demonstration of how various factors can influence the success of a therapy self-administered by technology. They corroborate the importance of taking into account all treatment-related, technology-related, and patient-related factors throughout the implementation process, beginning with deciding whether or not to set up such treatment with a particular patient. This implementation obviously requires an investment of time on the part of the clinician at the beginning of the treatment. However, once the self-administered treatment has begun, a considerable time saving is expected, which is a significant advantage in clinical practice. Moreover, by choosing carefully which treatment goals are well suited for self-administration, the clinician can make the most effective use of his/her face-to-face time with the client, working on specific objectives that require direct contact (e.g., apraxia of speech), thus maximizing the overall gains of therapy. When self-administered treatment is carefully planned and all winning conditions are gathered, it can be highly successful and allows the participant to make significant progress, as in L.M.'s case.
Self-administered treatment cannot replace traditional speech therapy but should be seen as complementary or a way to increase practice intensity and frequency. When transportation is completely impossible, other technologies such as telespeech therapy may be chosen. Speech-language treatments delivered by technology are often viewed as pleasant and motivating by individuals with aphasia. In addition, there are a growing number of apps, including some specifically designed for aphasia. Speech-language therapists could build on this to propose new methods to deliver attractive and intensive treatments of poststroke aphasia. Our recent studies also suggest that technology is a promising approach to reduce and/or compensate for language and cognitive deficits in individuals with neurodegenerative diseases. 29,41,42 However, regardless of the origin of acquired language deficits, self-administered treatments using technology are not appropriate for everyone and every clinical objective. This study provides the basis for determining key factors for the success of such treatments. Further studies are still needed to determine other considerations clinicians should take into account before proposing a technology-based self-administered treatment of poststroke aphasia.
Footnotes
Acknowledgments
J.M., N.B., and M.L. were supported by a research grant from the Quebec Network for Research on Aging (Fonds de la recherche du Québec—Santé). N.B. was supported by a salary award from the Fonds de la recherche du Québec—Santé. M.L. was supported by a Vanier Canada Graduate Scholarship.
Disclosure Statement
The authors report no conflict of interest.