
Abstract
Results: Telepsychiatry significantly reduced the total monthly LOS for nonhospitalized patients in the PedsER during the study period compared to all prior months (285–193 h;
p = 0.032) and compared to a similar prior seasonal time frame (329–193 h; p = 0.017). Telepsychiatry use reduced travel for face-to-face evaluations by 75% and saved 2.22 h per call day.
Introduction
Telepsychiatry has increased access to health care using real-time interactive videoconferencing, allowing clinicians and patients in separate locations to have a meaningful clinical encounter. Its use has increased over the past several years primarily due to the relative ease of use, the dire need of psychiatric (and in particular child psychiatry) services in remote underserved areas, and its benefit with regard to improvement in quality of care in select clinical settings. 1,2
Telepsychiatry has been noted in the literature to demonstrate equivalent efficacy in evaluations as face-to-face evaluations, and patient satisfaction is generally high. 1,2 Studies have shown improved outcomes (decreased dwell time and reduction of costs) and improved access in emergency settings (for children and adults). 3,4 No such studies have been done evaluating implementation in psychiatric training programs and developing subsequent competencies. This despite a growing usage of telepsychiatry in residency training programs and an importance given to acquiring specific knowledge and skills relevant to this practice, particularly in child psychiatry training. 5,6 Increasing access to use of telepsychiatry for trainees would improve access to valuable experiences during training that would decrease barriers to use post-training.
One benefit would be an enhanced understanding of potential cost savings through improved access for patients. However, a larger benefit for the training psychiatrist would be through mitigation of contributors to burnout. Burnout is a syndrome caused by work related stress, characterized by emotional exhaustion, depersonalization, and low sense of personal accomplishment. 7 The prevalence of burnout has been notably high during residency training. 8 Interventions such as increasing competence in the clinical work environment, reduction in work hours, and nurturing ones personal life have been described as beneficial in reducing burnout. 9,10 There have been no studies measuring the impact of using telepsychiatry for reducing dwell time/improvement in patient satisfaction while also considering the impact on resident/clinician burnout through reduction of clinical time burden when appropriate.
Our child psychiatry service has implemented telepsychiatry as a treatment intervention allowing us to evaluate patients (ages 3–18 years old, primarily under-represented minorities) who present to the pediatric emergency room (PedsER) in need of psychiatric care. Before institution of telepsychiatry, all patients were evaluated face-to-face, in person. During the week, the designated clinician would travel to the PedER when called to evaluate the patient while being still responsible to cover other services. On the weekend, the on-call child fellow would travel to the PedsER from home to the hospital to evaluate the patient. The previous face-to-face evaluations of these patients would contribute to the enhanced clinical burden for Child Psychiatry Fellows. This is the case during the week and also while on weekend call (who at times would travel great distance, incurring much cost). There was similarly a great burden on the PedsER system manifested in prolonged lag times to evaluation, decreasing the available space for other patients who are in need of medical or psychiatric care.
There are two study assumptions as follows: (1) use of telepsychiatry will decrease length of stay (LOS) of pediatric psychiatry patients in the PedsER and (2) use of telepsychiatry would sufficiently decrease the time investment for the evaluating clinician (which includes the evaluation time and time of travel to and from the evaluation site). This reduction of burden within clinical activities is a factor to be considered in the context of burnout among training physicians.
Materials and Methods
In this study, we offered all patients presenting to the PedsER the option of evaluation by the physician on duty through telepsychiatry (through informed consent with the legal guardian). These patients evaluated are of all diagnostic presentations and previously were evaluated face-to-face. For the purposes of this study, no patients are directly solicited or questioned regarding their experience. During the study period (July 1, 2017 to December 30, 2017), we evaluated data regarding physician use of telepsychiatry, clinical evaluation time, travel time, and reasons for refusal of telepsychiatry through a prospective real-time questionnaire that each child psychiatry fellow filled out at the end of their weekend call (Fig. 1—questionnaire). Patient LOS was measured from the patient's registration time through time of discharge, and data from study period were compared to data collected before the implementation of telepsychiatry.
Child Psychiatry Fellow Questionnaire.
We have worked to obtain a secure telepsychiatry communication on the patient end (hardwired into the hospital network) and on the provider side (through hospital administered laptops on a secure VPN hospital network). Encryption is at standard level as required for the practice of HIPAA compliant telemedicine. In addition, as a result of hard wired installation, the quality and reliability of the video and audio quality have been established as a result of adequate bandwidth.
Results
We found that use of telepsychiatry significantly reduced the total monthly LOS for nonhospitalized patients in the PedsER during the testing period compared to all prior months. This was a significant decrease from 285 to 193 h with p = 0.032 using unequal variance for one-tailed t test (Fig. 2). Given that emergency room volume tends to demonstrate seasonal variation, we compared the testing period to a similar time period before telepsychiatry implementation and found a similar result for nonhospitalized patients. We similarly found a significant reduction in monthly LOS for nonhospitalized patients, a decrease from 329 h in July 1, 2016 to December 30, 2016 down to 193 h during the study period July 1, 2017 to December 30, 2017 (Fig. 3). Use of telepsychiatry did not significantly reduce the LOS for patients who went on to ultimately be hospitalized. Table 1 details information compiled from the questionnaires administered to the trainee after each call. Use of telepsychiatry on average saved the child psychiatry fellow 2.22 h per call day, as a result of elimination of travel time to the PedsER. This resulted in ∼46.2 h of time saved in total for weekend calls during the study period. Use of telepsychiatry reduced dwell time (time from consultation to evaluation) by ∼1.1 h per call day, a total of 23.1 h during the study period.
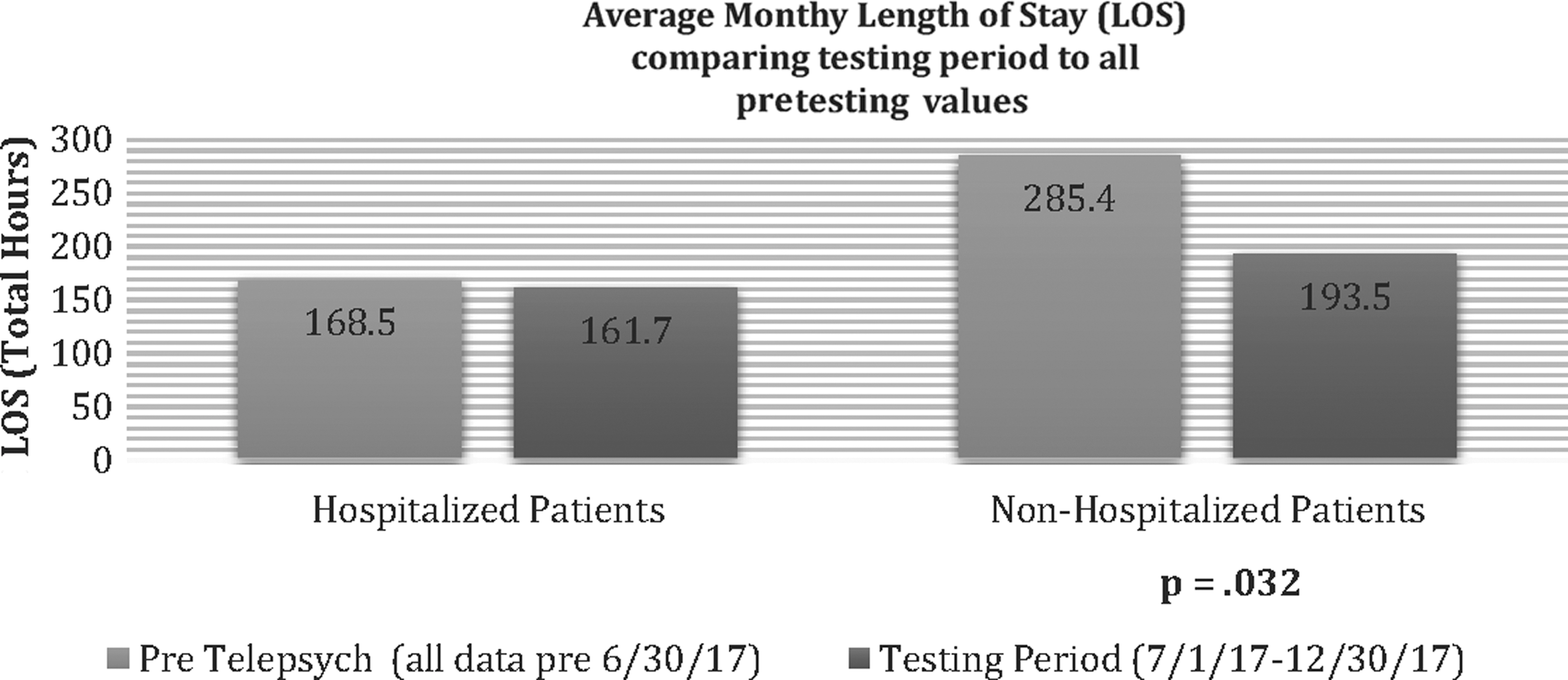
Average monthly LOS for pediatric psychiatry patients presenting to the PedsER comparing the testing period to all prior data points. LOS, length of stay; PedsER, pediatric emergency room.
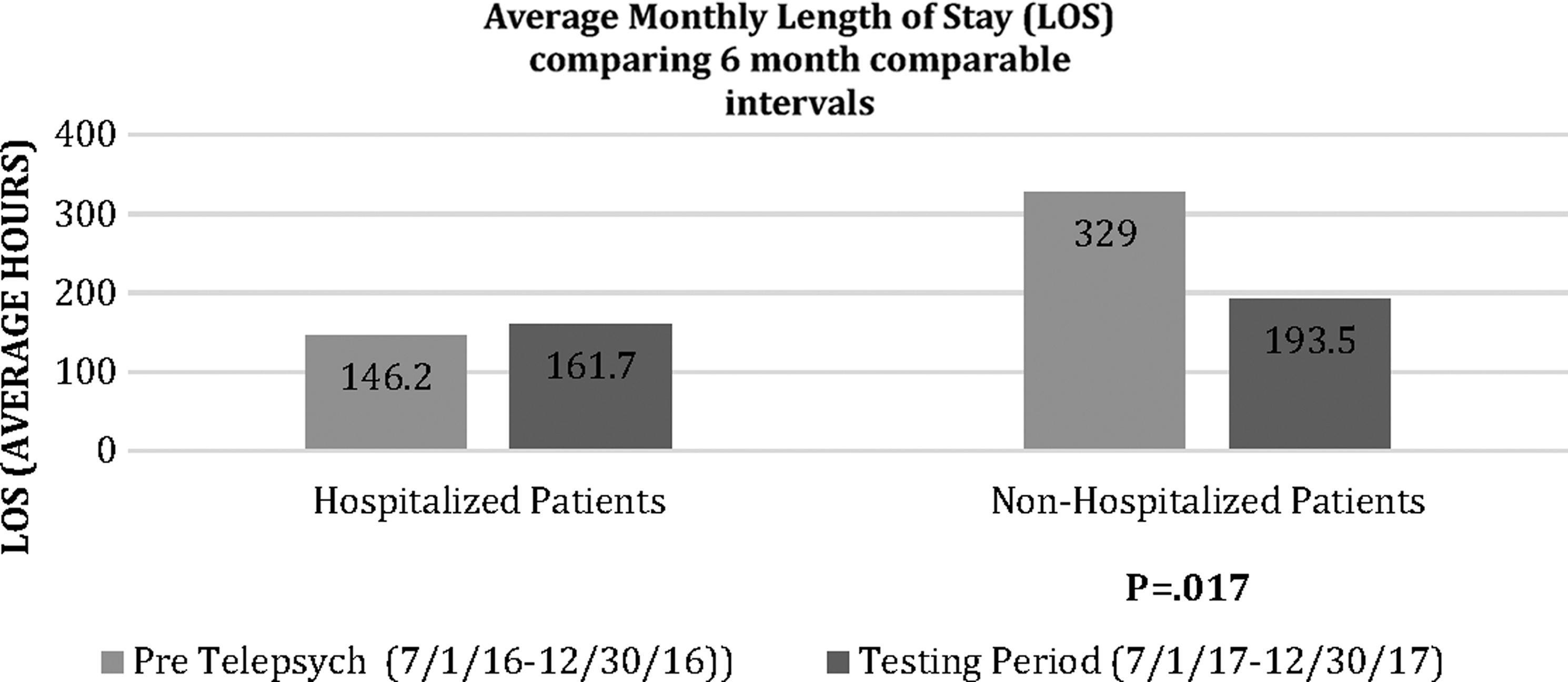
Average monthly LOS for pediatric psychiatry patients presenting to the PedsER comparing the testing period (July 1, 2017 to December 30, 2017) to the same time frame 1 year earlier (July 1, 2016 to December 30, 2016).
Data Table from the Child Psychiatry Fellow Questionnaires Gathered During the Testing Period July 1, 2017 to December 30, 2017
PedsER, pediatric emergency room.
Discussion
Use of telepsychiatry significantly reduced the total monthly LOS for nonhospitalized patients in the PedsER during the testing period compared to all prior months from 285 to 193 h. In addition, when comparing a similar seasonal time frame (comparing July 1 to December 30 of 2016 and 2017), there was similarly a significant reduction in LOS from 329 to 193 h. The importance of the latter reduction is that volume for psychiatric presentations in PedsERs can vary depending on the time of year. Volume is typically highest in the mid to late spring and just after the start of school, but lowest in the early winter. The faster turnaround time for patients presenting for psychiatric reasons allows for vacancies to be used by other patients who are waiting for emergency medical care. The use of telepsychiatry in this study showed promise in our system for improving access to other forms of specialized care consultation in the PedsER. Other medical specialties could similarly use telemedicine to improve access, turnaround time in their consult of patients in the PedsER (i.e., neurology).
Telepsychiatry did not significantly reduce the LOS for patients who went on to ultimately be hospitalized. We, however, would not have expected this intervention to address the LOS for hospitalized patients. This is primarily due to the fact that regardless of the speed of intervention, the vast majority of patients who will ultimately need hospitalization will remain in the PedsER over the weekend. Most admissions to inpatient psychiatric units in our system can only occur during the week, as this is the time that most units will engage in admission and discharge work. Nonetheless, patients who would ultimately be discharged benefit from being evaluated quickly as they would be ultimately able to leave the PedsER in a shorter time frame.
We also evaluated the use of telepsychiatry and its impact on the child psychiatry fellow's time commitment to patient care activities during their weekend call (Table 1). Of the 59 total weekend call days, 28 of them were days in which the fellow engaged patients for clinical evaluations (patient activity call days). Of the 35 total patient encounters, telepsychiatry was used in 26 of them, a usage rate of 74% per patient encounter. Of the 28 patient activity call days, only 8 of them resulted in the child fellow having to travel to the PedsER for face-to-face evaluation on the weekends, a reduction of 75%. In addition, the use of telepsychiatry on average saved the child psychiatry fellow 2.22 h per call day, as a result of elimination of travel time to the PedsER. This resulted in ∼46.2 h of time saved in total for weekend calls during the testing period. The reduction in time of travel contributes to the reduction in dwell time (time to evaluation), as well as the overall decreased LOS.
The reduction in LOS for psychiatric patients in the PedsER in the context of utilization of telepsychiatry is a notable outcome. These results certainly carry beneficial implications for our patient care system. Patients are discharged more quickly and not subject to unnecessarily prolonged wait times. A secondary benefit to the system is that resources devoted to care of psychiatric patients are now freed up for those in need of emergency medical care. Other studies have similarly demonstrated reduction in LOS, improved physician satisfaction, as well as cost reduction, and improved patient satisfaction. 3
However, those studies had two notable differences. First, the systems in these studies involved obtained benefit through reduction in need to send patients out to other facilities for psychiatric consultation. While this certainly had an impact with regards to decreased LOS, it did not improve the efficiency of the clinician workload. Our system relies on a consultant who travels to the PedsER to evaluate the patient in person. We demonstrated not only a reduction in the LOS but also a reduction in the frequency that an on-call trainee would have to travel to evaluate a patient in the PedsER. This 75% reduction in travel, translating to a time savings of 2.22 h per call day, is noteworthy for a training physician. Physician burnout, as noted, is quite prevalent in residency training. It would be tempting to see the implementation of telepsychiatry as simply a convenience for the physician, through reducing their workload. A more adaptive way to view this is an enhanced efficiency for the work that the trainee is already engaged. This lessened burden, reduction in hours of work through enhanced efficiency of clinical engagement, can be considered a mitigating factor for training physician burnout.
It has been reported that possible reasons for lack of robust mitigation of physician burnout have been a potential mismatch between the type of burnout and the solution to address it. 9 For instance, existential burnout, thought to stem from loss of meaning in medical practice and uncertainty of professional role, is thought to be mitigated through unique strategies. Recovery is thought to result from strategies such as forming connections with colleagues and patients, finding meaning in medicine, forming a professional identity, and feeling validated in ones experience of burnout. 9
Circumstantial burnout, thought to stem from work environment or personal challenges, is thought to be mitigated through proactive measures such as nurturing personal relationships, addressing high caseloads and long work hours, and taking time to engage in restorative activities outside of work. 9 Addressing inefficiency of workload, particularly through reduction of on-call clinical burden for trainees, can be a significant contributor to reducing circumstantial burnout. We showed that through introduction of a telepsychiatry program in a training program, we were able to reduce the frequency of travel for trainees. This translated to more available free time during a traditionally, and now unnecessarily, burdensome clinical activity. Trainees could theoretically use the time to recharge and spend time doing outside activities such as nurturing their personal lives, potentially lessening a contributor to the onset of burnout.
Limitations of this study were that while we measured the impact on LOS directly, we did not directly solicit improvements in quality of life, nor solicit information directly regarding elements of burnout from the trainees. As described above, the improved efficiency of work through reduced frequency of travel while on call and time saved serves as a proxy for mitigation of burnout. Direct survey of the residents in the future will directly solicit this information. In addition, while we compared data over a 6-month period to data from 2 years prior, it would have been more predictive and informative to have data for a longer evaluation period. And finally while we were able to use telepsychiatry in 75% of patient activity days on the weekend, we did not track the use of telepsychiatry during the weekday. However telepsychiatry during the weekday was less consistently used, and we presume that impact on LOS primarily came from swift intervention on weekend days that previously would have been much greater due to travel (compared to rapidity of intervention during the week due to proximity to the emergency room).
Footnotes
Acknowledgments
A special thanks to the Child Psychiatry Fellows at Harlem Hospital, Jess Shatkin, Shabana Khan, Dan Schechter, as well as to Brian Altonen, MPH for providing statistical support.
Disclosure Statement
No competing financial interests exist.