
Abstract
Background:
In 2015, we performed a cost analysis of a prenatal remote monitoring (RM) program compared with conventional care (CC) for women diagnosed with gestational hypertensive disorders (GHD).
Introduction:
We investigated where the cost savings were distributed by dividing our patient population into three subgroups, according to the gestational age (GA) at the time of delivery: (1) <34 weeks; (2) 34–37 weeks; and (3) >37 weeks of GA.
Materials and Methods:
Health care costs were calculated from patient-specific hospital bills at Ziekenhuis Oost Limburg (Genk, Belgium) in 2015–2016. Cost comparisons were made from the perspectives of the Belgium national health care system (HCS), the National Institution for Insurance of Disease and Disability (RIZIV), and the costs to individual patients.
Results:
A total of 256 pregnant women were included, 80 (31.25%) of whom received RM and 176 (68.75%) of whom received CC. The greatest difference in costs between RM and CC was in the group that delivered before 34 weeks of GA, followed by the group who delivered after 37 weeks of GA, and then the group of women who delivered at 34–37 weeks of GA. Most of the cost savings were in neonatal care, for both the three separate study subgroups and the total study group.
Discussion and Conclusion:
Our data showed that RM is more cost-effective than CC for pregnant women with GHD. Further investigation of the effects of RM on the long-term economic and social costs is recommended, together with an analysis of the price that should be asked for RM services.
Introduction
Gestational hypertensive disorders (GHD) are one of the most common complications during pregnancy. According to the Flemish Study Center of Perinatal Epidemiology (SPE), 4.9% of all pregnancies are complicated by these disorders: of the 64,323 deliveries in 2016, 3,152 were complicated by GHD. 1 GHD is defined as a systolic blood pressure (BP) >140 mmHg and a diastolic BP >90 mmHg. It refers to any of the following four conditions: (1) preexisting hypertension; (2) gestational hypertension; (3) preeclampsia; and (4) unclassifiable hypertension. 2 GHD is a major cause of maternal, fetal, and newborn morbidity and mortality. 2,3 The assessment of women with pregnancies complicated with GHD includes a clinical follow-up, serological investigation, and fetal ultrasound evaluation. The type and frequency of follow-up depend on the kind and severity of the hypertensive disorder. 2 The goal of treatment is to prevent significant cerebrovascular and cardiovascular events in the mother, without compromising fetal well-being. 4
Recently, new techniques for medical monitoring have been developed, such as remote monitoring (RM), which can be broadly defined as the use of telecommunication technologies to facilitate the transmission of medical information and services between health care providers and patients. 5 RM is a relatively new approach (dating back to the early 1990 s) that allows patient management at home. 6 As part of the Hasselt University and Limburg Clinical Research Program (LCRP), Ziekenhuis Oost-Limburg (Genk, Belgium) added RM of the blood pressure, activity level, and weight gain to its prenatal care for women with GHD in the Pregnancy Remote Monitoring (PREMOM) Study. The initial results were promising, 7,8 and other feasibility studies, within and outside pregnancy, have also successfully tested the possibility of sending data such as BP and/or body weight from the patient's home. 9,10 However, until now, few studies have evaluated the economic impact of RM compared with that of conventional care (CC). 11 –14 Our research team performed the first economic analysis to assess the costs of RM versus CC and we concluded that the RM prenatal follow-up of women with GHD is cost-effective for the global health care system (HCS). 15 A second cost analysis was performed in which data were collected in 2015 and 2016. In this study, in which we divided our patient population into three subgroups according to the gestational age (GA) at the time of delivery, we analyzed the cost savings made with RM and identified where these savings were made.
Materials and Methods
Data
Data collected from the PREMOM Study, extending from January 1, 2015, to December 31, 2016, were used for this cost analysis. The PREMOM Study design and data collection method are described in detail elsewhere. 7,8 Briefly, the PREMOM Study was a 2-year retrospective study, performed at the outpatient clinic of a secondary prenatal center, where pregnant women at risk for GHD received either RM or CC. In 2015 and 2016, 320 pregnant women were diagnosed with GHD: 90 (28.13%) received RM and 230 (71.88%) received CC. Women consenting to RM underwent obstetric surveillance with a BP monitor, an activity tracker, and a weight scale. Pregnant women in the prenatal remote follow-up program were asked to make one BP measurement in the morning and one in the evening, to make one weight measurement once a week, and to wear an activity tracker day and night until delivery or hospital admission. The data from the monitoring devices were transmitted to a Web-based dashboard developed by the Mobile Health Unit of Hasselt University. Predetermined alarm signals were set: based on international guidelines it was decided to generate an alarm signal when the diastolic blood pressure was greater than or equal to 90 mmHg and/or the systolic blood pressure was greater than or equal to 140 mmHg. 16,17 When appropriate, individual alarm signals were set (e.g., when they started with an antihypertensive therapy and on demand of the obstetrician). All alarm events were communicated to the obstetrician in charge to discuss management options before the patient was contacted and instructed at home. Therapeutic interventions were in accordance with local management strategies.
This study protocol was approved by the local ethics committees responsible for the site. The study conformed to the principles outlined in the Declaration of Helsinki. All patients gave their written informed consent, and all data were treated confidentially.
Study Design
The objective of the study was to determine where the main cost savings were distributed, or which aspect of the prenatal, perinatal, or postnatal care involved an increase in costs, when RM was used instead of CC. The study population was divided into three subgroups: (1) delivery before 34 weeks of GA (which is the cutoff value to determinate whether a pregnant women suffers from early or late preeclampsia); (2) delivery at 34–37 weeks of GA (which is the intermediate measure); and (3) delivery after 37 weeks of GA (which is the cutoff value to determinate whether a pregnant women delivers preterm or
The calculations were made for three major domains and the total costs, presented below. A detailed overview of the included costs is presented in Supplementary Data S1(Supplementary Data are available online.
Cost analysis: prenatal follow-up
All costs related to urgent and nonurgent in-office visits were used in the prenatal follow-up cost analysis: (1) cost of prenatal consultations; (2) cost of ultrasound examinations; and (3) cost of cardiotocographic readings.
Cost analysis: prenatal admission to the hospital
To evaluate the economic impact of RM on the three major stakeholders, the following data points were collected when a pregnant woman was admitted to the prenatal ward: (1) costs related to the laboratory tests of the mother; (2) costs of medicines; and (3) costs related to admission.
Cost analysis: maternal and neonatal care at and after delivery
For both the CC group and the RM group, the following costs were included: (1) cost of the delivery; (2) necessary costs for the care of the neonate; and (3) other costs.
Cost analysis: total costs
After analyzing these data, a cost analysis of the total costs was made. This included (1) the costs of the prenatal follow-up; (2) the costs of admission to the prenatal ward; and (3) the costs of maternal and neonatal care at and after delivery.
Statistical Analysis
Because the baseline characteristics were continuous data, they are summarized as mean ± SD. Categorical data are summarized as counts and percentages and were compared with the χ 2 test or Fisher's exact test, where appropriate. Costs are reported as means and standard deviations or medians and interquartile ranges, depending on if they were normally or abnormally distributed. Differences in costs were calculated with the Mann–Whitney U test, because the cost data were typically highly skewed, 19 in that, a few patients incurred particularly high costs. Nominal level α < 0.05 was considered significant. All statistical analyses were performed with SPSS release 24.0 (IBM Corp. Released 2016. IBM SPSS Statistics for Windows, Version 24.0; IBM Corp, Armonk, NY).
Results
Pregnancy-Related Outcomes
The pregnancy-related outcomes of the patients are summarized in Table 1. Of the 90 patients who participated in the RM study, 10 (11.12%) were excluded because they received (part of) their prenatal follow-up at another prenatal center and the financial bills for those services were not available. In the CC group, 54 (23.48%) patients were excluded for the same reasons. Finally, the RM group comprised 80 patients (31.25%) and the CC group comprised 176 patients (68.75%). The pregnancy-related outcomes of the populations enrolled were almost homogeneous, with no difference between the groups, except in the prevalence of gestational hypertension (80.00% in RM vs. 50.56% in CC, p < 0.001) and preeclampsia (18.75% in RM vs. 41.48%, p < 0.001) in the total study group and in the group with GA >37 weeks (86.15% in RM vs. 56.06% in CC [p < 0.001] and 12.31% in RM vs. 35.61% in CC [p = 0.001], respectively).
Pregnancy-Related Outcomes
Values are mean (±SD) or numbers (percentages).
Bold and underlined values denote a significant level of p < 0.05.
CC, conventional care; EH, essential hypertension; GA, gestational age; GH, gestational hypertension; GHD, gestational hypertensive disorder; HELLP, hemolysis, elevated liver enzymes, and low platelets; PE, preeclampsia; RM, remote monitoring.
Total Costs
An overview of the total costs per study group is presented in Supplementary Tables S1, S2, S3, S4 and in Figure 1. Figure 1 presents the average costs (±SD) for the three study subgroups and the total study group. The costs are categorized according to the patient costs (not refunded by the health insurance), RIZIV costs (refunded by the Belgium national health care insurance), and health care services costs (which is the sum of the patient and the RIZIV costs). There were no significant differences in the three study subgroups (< 34 weeks of GA, 34–37 weeks of GA, and >37 weeks of GA), or when all three subgroups were combined, between RM and CC in the total costs for HCS and RIZIV, or patient costs. There was a reduction of 50.52% (€9,125.17) in the HCS costs for women who delivered before 34 weeks of GA, 1.16% (€35.94) for women who delivered after 37 weeks of GA, and 25.00% (€1293.86) for the total study group when RM was compared with CC. There was an increase in the total HCS cost of 3.90% (€227.12) for the RM group women who delivered at 34–37 weeks of GA. Among women who delivered before 34 weeks of GA, there were reductions of 56.23% (€8,929.77) in the RIZIV costs and 8.95% (€195.18) in the patient costs when the women were treated with RM rather than with CC. Women treated with RM who delivered at 34–37 weeks of GA had a reduction in RIZIV costs of 21.03% (€652.13) and an increase in the patient costs of 67.04% (€863.79) compared with the CC women. Among the women who delivered after 37 weeks of GA, the RIZIV costs were 5.09% (€102.42) lower in the RM group than in the CC group, but the patient costs were 6.08% (€66.49) higher in the RM group than in the CC group. In summary, the total cost for RIZIV was 35.17% (€1,383.72) lower in women treated with RM than in women treated with CC, but the patient costs were 7.07% (87.89) higher for the women in the RM group than for those in the CC group.
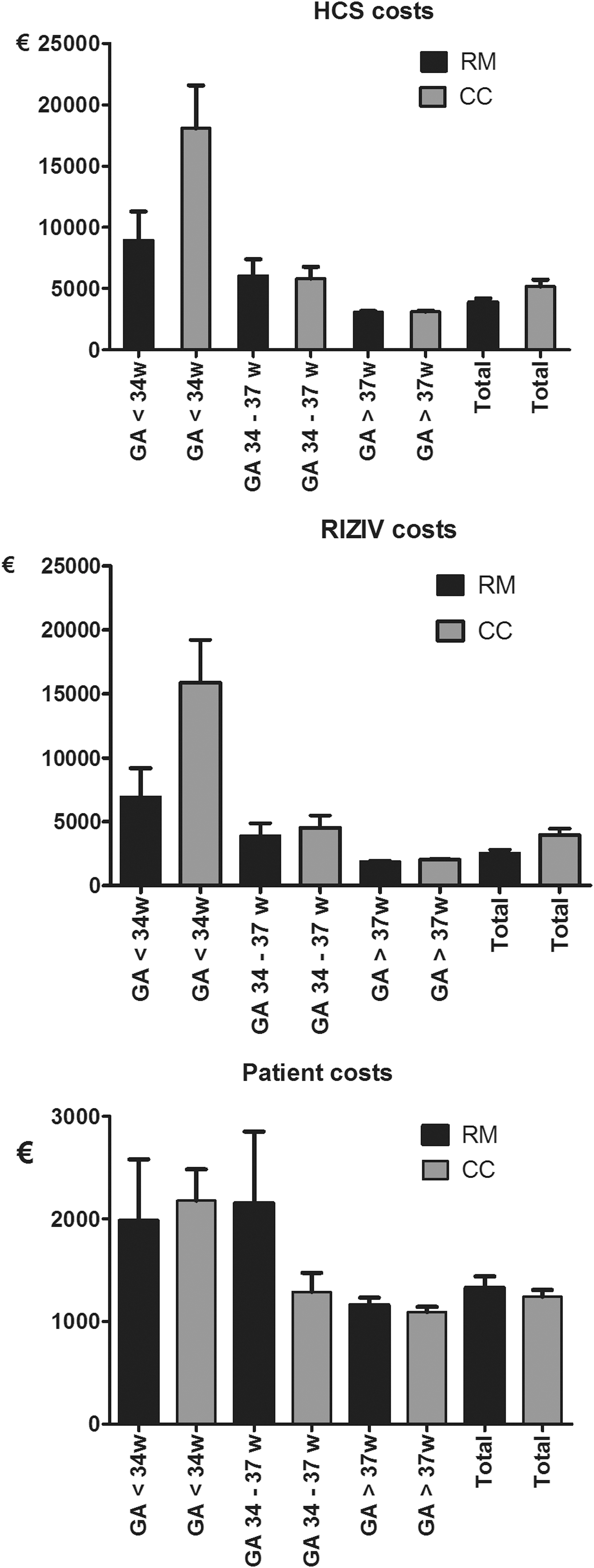
Overview of total costs per study group. CC, conventional care; GA, gestational age; HCS, healthcare system; RIZIV, National Institution for Insurance of Disease and Disability; RM, remote monitoring.
Distribution of Cost Savings
The health care costs for the three major domains, according to study group, are presented in Supplementary Tables S5, S6, S7, S8. In women who gave birth before 34 weeks of GA, 91.96% of the cost savings were in maternal and neonatal care at and after delivery (they were all located in the neonatal care), and less than 10% of the costs savings were located in the prenatal follow-up (0.34%) and the prenatal admission to the hospital (7.70%) (which could be further divided in prenatal visits (0.18%), ultrasound (0.16%), prenatal admission (7.58%), and medications (0.12%)). In women who gave birth at 34–37 weeks of GA, 79.11% of the cost reductions were located in maternal and neonatal care at and after delivery (which all are located in the neonatal care), followed by the prenatal admission until to the hospital (medications (12.16%) and laboratory tests (5.44%)), and 3.29% for the prenatal follow-up (an reduction in the prenatal visits of 3.29%). In women who delivered after 37 weeks of GA, 76.27% of the cost reductions were located in maternal and neonatal care at and after delivery (of which 59.60% is located in the neonatal care and 16.67% in other), 17.92% in the prenatal follow-up (14.91% in prenatal visits and 3.01% in the ultrasounds), and 5.81% in the prenatal admission to the hospital (which are located in the laboratory tests).
Discussion
Principal Findings
We investigated where the main cost savings in an RM prenatal follow-up program were distributed by dividing the patient population into three subgroups according to the GA at the time of delivery.
The findings of this study, performed on a dataset collected over 2 years, showed that the greatest differences in costs between RM and CC were in the group who delivered before 34 weeks of GA (50.52% in HCS costs, 56.23% in RIZIV costs, and 8.95% in patient costs), followed by the group who delivered after 37 weeks of GA (1.16% in HCS costs, 5.09% in RIZIV costs, and −6.08% in patient costs), and was least in the group of women who delivered at 34–37 weeks of GA (−3.90% in HCS costs, 21.03% in RIZIV costs, and −67.04% in patient costs). In the total RM group, the reductions were 25.00% in HCS costs, 35.17% in RIZIV costs, and −7.07% in patient costs.
Most of the cost savings were in neonatal care for all three study subgroups (birth <34 weeks GA, birth 34–37 weeks GA, and birth >37 weeks GA) and when all three study subgroups were analyzed together. Obviously, the higher the GA at the time of delivery, the lower the cost for neonatal care. In the RM women who delivered after 34 weeks of GA, reductions were observed in the costs of prenatal visits (3.29% with birth at 34–37 weeks of GA and 14.91% with birth at >37 weeks of GA), ultrasound (3.01% with birth at >37 weeks of GA), laboratory tests (approximately 5% in both groups), medications (12.16% with birth at 34–37 weeks of GA), and other costs (16.67% with birth at >37 weeks of GA) compared with the CC group. When the study subgroups were analyzed together, more than 95% of the cost savings with RM were in neonatal care.
Strengths and Limitations
The use of “real-life” data from hospital bills and from the SPE was the main strength of this study. By using these data, the actual situation of pregnancies complicated with GHD (in Flanders) was analyzed and the results are generalizable to settings with similar economic and social characteristics. It is nearly impossible to give all pregnant women with GHD this type of prenatal care, but it is clear that for each woman who received this type of care, the HCS cost was reduced.
The main limitation of this study was that the patients from the PREMOM Study were not randomized. Nevertheless, the PREMOM Study and this financial analysis provide a picture of the “real-life” situation in Belgium. We obtained the data from patient files and hospital bills, although we had no information on patients' acts of hospital and medical consumption and the patients' social costs (such as transportation and travel costs and the loss of employment income during hospital stays). These results may differ in different HCSs and different economic and social settings, such as in other countries. This study was also limited to 6 weeks after delivery. It is clear that neonates who need intensive care at the moment of delivery will have higher health care costs than neonates who do not need this care. These costs usually arise from rehospitalizations, acute care visits, or further intensive care for the rest of the infant's life. Finally, the costs for organizing RM are not taken into account, which are as follows: the RM devices, the midwife who supervised the data, and the technical support. To obtain a complete picture of the cost of and cost savings attributable to this technology, further research is required, which takes these data into account.
Comparisons With Previous Trials
A cost analysis of an RM prenatal follow-up program for women with GHD, for which the data analysis was performed in 2015, was, to the best of our knowledge, the first study to report that RM is cost-effective for a global HCS, mainly through savings to the insurance institution RIZIV. Since that analysis was completed, no new studies have been published on the financial impact of an RM prenatal follow-up program for women with GHD.
Possible Explanations
This study demonstrated that neonatal care is one of the largest costs in the care of mothers and babies. However, this is not new information. Neonatal care is characterized by its intensive character and is known as one of the most expensive services in hospitals. 20 It is recognized that most neonatal morbidity associated with GHD is attributable to the complications of prematurity and the cost of neonatal care correlates with the severity of prematurity. 21 Our research team has shown that the neonates in the RM group, who were born before 34 weeks of GA, were approximately 10 days older than the corresponding neonates in the CC group. RM makes it possible for caregivers to see abnormal events in pregnant women and offer an intervention when necessary to prevent the worsening of the disease. It may not always be possible to prevent a premature delivery, but RM makes it possible to delay a premature delivery by up to 10 days. These 10 days will have a significant impact on the health of the neonate and reduce the costs to the HCS and RIZIV by more than 50%. The lower prevalence of premature births in the RM group compared with the CC group can be similarly explained. The literature indicates that a premature birth at 28–36 weeks of GA is 2.30 times more expensive than a birth after 36 weeks of GA, and that births before 28 weeks of GA are 12.47 times more expensive. 21 Because fewer premature neonates were born in the RM group than in the CC group, the cost savings will increase when RM is extended to all pregnant women in Flanders. This can explain the cost savings that will be reached when we extrapolate this over a large number of women with GHD.
The increase in patient costs for the study group who delivered at 34–37 weeks of GA mainly occurred in the categories “prenatal admission,” “neonatal admission,” and “delivery” (39.88%, 41.20%, and 14.98%, respectively). Further analysis of these data showed that pregnant women in the RM group were more likely to choose a single room for their hospitalization than a room shared with other patients. Therefore, the patient costs were higher in the RM group. Moreover, more insurance was reimbursed to the women in the CC group, whose child was hospitalized after delivery, than to the corresponding women in the RM group. This may explain the large difference in the costs incurred by the two groups.
To conclude, of the women who gave birth at >37 weeks GA, significantly more patients were diagnosed with preeclampsia and fewer with gestational hypertension in the CC group than in the RM group. Although these diseases require different treatments, which entail different costs, the GA at which these women gave birth partly explains the slight discrepancy in costs. Women who gave birth at >37 weeks of GA, who were considered at risk for or had preeclampsia, were less likely to be hospitalized due to the GA, but had more frequent prenatal visits and laboratory tests to monitor their vital parameters. This difference in costs is clear in this study, but it did not affect the total costs as strongly as the difference in the cost of neonatal care in the group who gave birth at <34 weeks of GA.
Recommendations for Further Research
This study was restricted to a postnatal follow-up period of 6 weeks after delivery. It would be interesting to monitor the neonates in both the RM and CC groups for more than 6 weeks postpartum to allow a long-term cost–benefit analysis. Because the social costs (such as transportation and travel costs and the cost of lost employment income for the time spent in hospital) were not taken into account in this study, it would be interesting to include this type of cost in a future study. It is possible that the differences in costs will be even greater when these factors are also considered. It would also be interesting to know how much pregnant women are prepared to pay each month to fund the RM service. In this way, it would be possible to fund RM through both RIZIV and patient contributions. The costs required to provide RM were not taken into account in this analysis, but should be included in follow-up studies. To conclude, for future RM programs, it would be interesting to implement screening tools toward the identification of pregnancies at high risk for hypertensive and/or fetal growth. Some screening programs already exist (e.g., for preeclampsia and gestational diabetes mellitus), but most of them are troubled with poor performance both in terms of sensitivity and/or specificity, particularly for late preeclampsia, gestational hypertension, or isolated fetal growth restriction. A prenatal screening tool with a high sensitivity and specificity rate would allow including only high-risk pregnancies in RM programs. This is necessary to prevent an unwanted rise of costs of RM offered to all pregnant women.
Conclusions
When an RM program was included in the prenatal care of women at risk of GHD, the greatest differences in costs between RM and CC were observed in the women who gave birth before 34 weeks of GA, followed by the group who delivered after 37 weeks of GA, and were least in the group of women who delivered at 34–37 weeks GA. In the total study group, saving in both the HCS and RIZIV costs were observed. Most of the cost savings were in neonatal care, both in the three individual RM study subgroups and in the combined RM group. Our data show that RM is more cost-effective than standard care for pregnant women with GHD. We recommend further investigation into the effect of RM on long-term and social costs, and into the price that can be asked for the provision of RM services.
Footnotes
Acknowledgments
We thank the obstetricians and midwives of the Department of Gynecology at the Ziekenhuis Oost-Limburg and the other hospitals participating in the PREMOM project (JESSA Ziekenhuis, Hasselt; Sint-Franciskusziekenhuis, Heusden-Zolder; Ziekenhuis Maas en Kempen, Bree; Mariaziekenhuis Noord-Limburg, Overpelt; Sint Trudo, Sint Truiden; and AZ Vesalius, Tongeren). We also like to thank the financial department of the Ziekenhuis Oost-Limburg (Genk, Belgium) for their assistance and support during this study.
This study is part of the Limburg Clinical Research Program (LCRP) UHasselt-–ZOL–Jessa, supported by the Foundation Limburg Sterk Merk, the province of Limburg, the Flemish Government, Hasselt University, Ziekenhuis Oost-Limburg, and Jessa Hospital. This work was supported by Foundation Mustela (Laureate 2016).
Disclosure Statement
None of the authors have financial interests or other conflicts of interests to report.
Supplementary Material
Supplementary Data S1
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
Supplementary Table S7
Supplementary Table S8
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.